Last updated: May 20, 2026
Quick Answer: The three main skin cancer types are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma. BCC is the most common and least dangerous; melanoma is the rarest of the three but the most deadly. Early detection dramatically improves outcomes for all skin cancer types, and most cases are curable when caught before they spread.
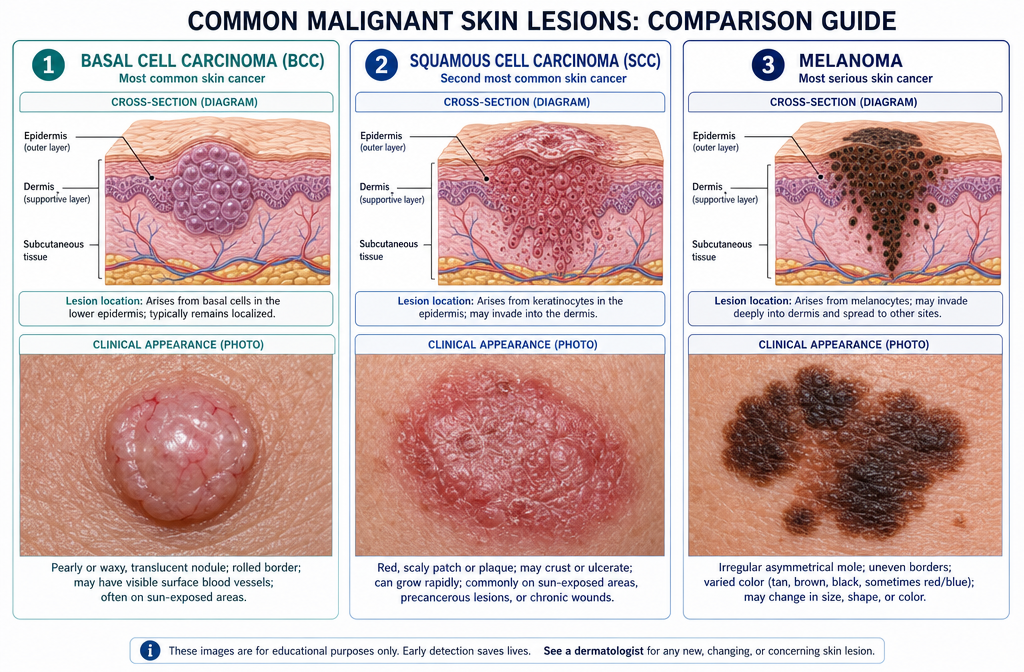
The three primary skin cancer types are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma. BCC and SCC are sometimes grouped together as "non-melanoma" or "keratinocyte carcinomas" because they arise from the skin's surface cells. Melanoma develops from melanocytes, the cells that produce pigment, and is biologically distinct from the other two [3].
BCC is the most frequently diagnosed skin cancer worldwide. It originates in the basal cells at the bottom of the epidermis and almost always appears on sun-exposed areas: the face, neck, ears, scalp, and hands.
What BCC looks like:
BCC rarely spreads to other organs, but it can grow deep into surrounding tissue — including bone — if left untreated for years. For a deeper look at this type, see this guide to basal cell carcinoma removal and treatment.
SCC arises from the squamous cells in the outer layers of the skin. It's the second most common skin cancer type and can develop on any part of the body, including areas not exposed to the sun (lips, inside the mouth, genitals).
What SCC looks like:
SCC carries a higher risk of spreading than BCC, especially when it develops on the lips, ears, or in people with weakened immune systems. Actinic keratoses — rough, scaly patches caused by sun damage — are considered pre-cancerous lesions that can progress to SCC. Learn more about actinic keratosis and its progression to SCC.
Melanoma is the most dangerous of the common skin cancer types. It develops in melanocytes and can appear anywhere on the body, including areas with no sun exposure. Approximately 112,000 new cases of invasive melanoma are expected in the U.S. in 2026, up from about 104,960 projected in 2025 — a trend that continues despite improved awareness [4].
What melanoma looks like (use the ABCDE rule):
LetterStands ForWhat to Look ForAAsymmetryOne half doesn't match the otherBBorderIrregular, ragged, or blurred edgesCColorMultiple shades of brown, black, red, white, or blueDDiameterLarger than 6mm (about the size of a pencil eraser)EEvolvingAny change in size, shape, color, or new symptoms
These are far less common but worth knowing:
For a broader overview of all four main categories, the complete guide to the 4 types of skin cancer covers each in detail.
Basal cell carcinoma is the most common skin cancer type by a wide margin. The Skin Cancer Foundation estimates that BCC accounts for about 80% of all non-melanoma skin cancer diagnoses in the U.S. [6]. SCC accounts for most of the remaining cases, while melanoma represents a smaller proportion of total diagnoses but a disproportionately high share of deaths.
To put it plainly:
Skin cancer overall is the most common cancer in the United States [1], and its incidence continues to rise each year [2].
Melanoma is significantly more dangerous than BCC. While BCC is rarely life-threatening, melanoma can spread rapidly to lymph nodes and internal organs, making it responsible for the vast majority of skin cancer deaths.
Here's a practical comparison:
FeatureBasal Cell CarcinomaMelanomaSpread to other organsVery rareCommon if untreated5-year survival (localized)~99%~99%5-year survival (distant spread)Extremely rare scenario~35%Growth speedSlowCan be rapidTreatment complexityUsually simple excisionMay require immunotherapy
The key takeaway: BCC caught early is almost always curable with minor surgery. Melanoma caught early is also highly treatable, but delayed diagnosis can be fatal. This is why the distinction between skin cancer types matters so much clinically.
For more on what melanoma looks like and how it's treated, see the melanoma surgery and treatment overview.
The earliest warning signs of skin cancer vary by type, but any new, changing, or unusual skin growth warrants prompt evaluation. Most skin cancers are visible to the naked eye, which makes self-examination a powerful first-line tool.
General warning signs across all skin cancer types:
💡 Pull Quote: "Any skin lesion that looks different from your others — dermatologists call this the 'ugly duckling sign' — deserves a professional evaluation, regardless of your age or skin tone."
People often assume skin cancer only looks like a dark mole, but BCC frequently appears as a shiny, skin-colored bump, and SCC can look like a rough patch or a non-healing sore. For a visual reference, see this guide to early-stage skin cancer pictures and signs.
Common mistake: Waiting for a lesion to hurt before seeking evaluation. Most skin cancers are painless in early stages. If you're wondering does skin cancer hurt, the answer is: usually not until it's advanced.
People with fair skin, light eyes, and light hair carry the highest baseline risk for all skin cancer types, but no skin tone is immune. The Fitzpatrick scale (Types I–VI) is the standard tool dermatologists use to assess UV sensitivity and skin cancer risk.
Fitzpatrick TypeSkin ToneRelative RiskType IVery fair, always burnsHighestType IIFair, usually burnsVery highType IIIMedium, sometimes burnsModerateType IVOlive, rarely burnsLowerType VBrown, very rarely burnsLowType VIDark brown/black, almost never burnsLowest (but not zero)
Important nuance: People with darker skin tones (Types IV–VI) are diagnosed with skin cancer less often, but they are more likely to be diagnosed at a later stage — partly because lesions may be harder to spot on darker skin and partly because of lower clinical suspicion. Melanoma in Black patients, for example, often appears on the palms, soles, and under the nails (acral lentiginous melanoma), areas not associated with sun exposure.
For a detailed breakdown of how skin type affects cancer risk, the Fitzpatrick skin type complete guide is a useful reference.
Additional risk factors beyond skin type:
Yes — young people absolutely can and do develop skin cancer. Melanoma is one of the most common cancers diagnosed in adults aged 15–39, and SCC rates in younger adults have been rising, partly due to indoor tanning [2][6].
Choose to screen early if:
The misconception that skin cancer is "an older person's disease" leads to delayed diagnosis in younger patients. Any suspicious lesion should be evaluated promptly, regardless of age.

Dermatologists diagnose skin cancer types through a combination of visual examination, dermoscopy, and skin biopsy. A biopsy — removing a small sample of tissue for laboratory analysis — is the only way to confirm a skin cancer diagnosis definitively.
Common mistake: Assuming a dermatologist can definitively diagnose skin cancer by sight alone. Dermoscopy improves accuracy, but biopsy is always required for a confirmed diagnosis. Conditions like dermatofibroma vs. skin cancer can look similar to the untrained eye.
Skin cancer screening costs range from $0 (covered by insurance as a preventive visit) to $150–$300+ out-of-pocket for a full-body skin exam, depending on your location, provider, and insurance plan. Biopsy costs are additional and vary by complexity.
ServiceEstimated Cost (Canada/US)Full-body skin exam (insured)$0–$30 copayFull-body skin exam (uninsured)$100–$300Dermoscopy add-on$25–$75Skin biopsy (shave/punch)$150–$500+Pathology fee$100–$400Mohs surgery (if needed)$1,000–$5,000+
In Canada, provincial health plans (OHIP and equivalents) typically cover medically necessary skin cancer assessments and biopsies when referred by a physician, but cosmetic or screening-only visits may not be covered.
For those in the Greater Toronto Area, the complete guide to skin cancer screening in Toronto lists specific clinics and what to expect cost-wise.
Decision rule: If you have a suspicious lesion that's changing, bleeding, or worrying you, don't delay because of cost. Most provincial and state health systems cover biopsy of clinically suspicious lesions.
Treatment for skin cancer depends on the type, size, location, and stage. Most early-stage skin cancers are treated with surgery alone. Advanced cases may require radiation, targeted therapy, or immunotherapy.
Basal Cell Carcinoma:
Squamous Cell Carcinoma:
Melanoma:
💡 Key point: Immunotherapy has dramatically improved survival rates for advanced melanoma over the past decade. Patients diagnosed with stage IV melanoma today have significantly better outcomes than those diagnosed ten years ago.
For information on surgical options for skin lesions, the skin cancer surgeries overview covers what to expect before and after procedures.
Yes — the majority of skin cancers are completely curable, especially when caught early. BCC and SCC have cure rates exceeding 95% when treated at an early stage. Early-stage melanoma (Stage I) also has a 5-year survival rate near 99% [6].
The factors that most affect curability:
Edge case: Even after successful treatment, skin cancer can recur or new primary cancers can develop. Anyone treated for one skin cancer has a significantly higher lifetime risk of developing another. Annual skin checks should continue indefinitely after any skin cancer diagnosis [8].
Skin cancers spread through three main mechanisms: local tissue invasion, lymphatic spread, and blood-borne (hematogenous) metastasis. The likelihood and speed of spread varies dramatically by type.
Understanding how each type spreads explains why treatment urgency differs. A small BCC on the nose can wait a few weeks for scheduling. A thick melanoma on the back should be excised as soon as possible.
Skin cancer has a hereditary component, but the majority of cases occur in people without a family history. Genetics influence risk; they don't determine destiny.
Hereditary factors that increase skin cancer risk:
Practical implication: If a first-degree relative (parent, sibling, child) has been diagnosed with melanoma, mention this to your dermatologist. You may qualify for more frequent screening or genetic counseling. That said, UV exposure remains the most modifiable risk factor — sun protection matters regardless of your genetic background [3][6].
The most dangerous mistake is assuming skin cancer only looks one way or only affects one type of person. These misconceptions lead to delayed diagnosis and worse outcomes.
Mistake 1: "I have dark skin, so I don't need to worry."
People with darker skin tones do have lower rates of UV-related skin cancers, but they're not immune. Acral lentiginous melanoma — which occurs on palms, soles, and under nails — is not UV-related and disproportionately affects Black and Asian patients. Bob Marley died of this subtype.
Mistake 2: "It's just a pimple or a sore that won't heal."
Basal cell carcinoma is frequently mistaken for a pimple, ingrown hair, or minor wound. Any sore that hasn't healed in 4+ weeks should be evaluated.
Mistake 3: "Sunscreen is enough protection."
Sunscreen is important but not a complete solution. It must be applied correctly (SPF 30+, reapplied every 2 hours), and protective clothing, shade, and avoiding peak UV hours (10am–4pm) are equally important.
Mistake 4: "Tanning beds are safer than the sun."
Tanning beds emit UV radiation that can be 10–15 times more intense than midday sun. They are classified as a Group 1 carcinogen by the World Health Organization [6].
Mistake 5: "If it doesn't hurt, it's not cancer."
Most skin cancers are painless until advanced. Pain is a late symptom, not an early warning sign.
Mistake 6: "I only need a skin check if I see something worrying."
Annual full-body skin exams by a dermatologist catch lesions patients can't see themselves — on the scalp, back, and between toes.
Q: What is the deadliest type of skin cancer?
Melanoma is the deadliest skin cancer type. Although it accounts for a smaller proportion of skin cancer diagnoses than BCC or SCC, it causes the vast majority of skin cancer deaths because of its ability to spread rapidly to other organs [6].
Q: Can you get skin cancer on areas not exposed to the sun?
Yes. Melanoma can develop anywhere on the body, including the scalp, between the toes, under the nails, on the genitals, and inside the eye. Some subtypes of melanoma have no connection to UV exposure at all.
Q: How often should I get a skin cancer screening?
Most dermatologists recommend a full-body skin exam once a year for average-risk adults. People with a personal or family history of skin cancer, many moles, or significant sun damage may need checks every 6 months [8].
Q: What does basal cell carcinoma feel like?
BCC is usually painless. It may feel like a smooth bump, a slightly raised area, or nothing at all. Some people notice it only because it bleeds easily when bumped or doesn't heal after what seems like a minor scrape.
Q: Can skin cancer come back after treatment?
Yes. Skin cancer can recur at the original site or appear as a new primary cancer elsewhere on the skin. This is why ongoing annual monitoring is essential even after successful treatment [8].
Q: Is melanoma always dark or black?
No. Amelanotic melanoma is a subtype that contains little or no pigment and can appear pink, red, or skin-colored. It's often mistaken for a benign lesion and is more likely to be diagnosed at a later stage.
Q: Does sunscreen prevent all skin cancer types?
Sunscreen significantly reduces UV-related skin cancer risk, but it doesn't prevent all types. Non-UV-related melanoma subtypes, for example, are not prevented by sunscreen. Broad-spectrum SPF 30+ sunscreen, combined with protective clothing and shade, provides the best overall protection.
Q: Can a mole turn into melanoma?
Most melanomas arise as new spots rather than from existing moles. However, a small percentage develop within a pre-existing mole. Any mole that changes in size, shape, color, or texture should be evaluated promptly.
Q: What's the difference between a skin lesion and skin cancer?
A skin lesion is any abnormal area of skin — this includes both benign (harmless) and malignant (cancerous) growths. Skin cancer is a specific category of malignant skin lesion. Most skin lesions are benign. For a comprehensive overview, see this guide to 25+ types of skin lesions.
Q: Are white spots on the skin a sign of cancer?
White spots on the skin are usually benign (e.g., vitiligo, fungal infections, sun damage), but certain white lesions — particularly leukoplakia in the mouth — can be pre-cancerous. Any new or changing white spot should be checked. Learn more about white spots on skin and cancer risk.
Q: How is Merkel cell carcinoma different from melanoma?
Merkel cell carcinoma (MCC) is rarer and arises from nerve-associated cells in the skin, while melanoma arises from pigment cells. MCC is often linked to Merkel cell polyomavirus infection and UV exposure. It tends to be more aggressive than melanoma and has a higher recurrence rate, but it's far less common.
Q: What should I do if I find a suspicious spot?
Don't wait. Book an appointment with a dermatologist or visit a skin cancer clinic. Take a photo of the lesion to track any changes before your appointment. Avoid picking, scratching, or attempting to remove it at home.
Skin cancer is the most common cancer in North America, but it's also among the most preventable and treatable when caught early [1][6]. The key is knowing which skin cancer types exist, what they look like, and when to act.
Actionable next steps:
Skin cancer doesn't have to be a death sentence. With the right knowledge and timely action, the vast majority of people diagnosed with any skin cancer type make a full recovery.
[1] Skin Cancer Is The Most Common Cancer In The U.S. — Here's What You Need To Know In 2026 - https://www.schweigerderm.com/skin-care-articles/skin-cancer/skin-cancer-is-the-most-common-cancer-in-the-u-s-heres-what-you-need-to-know-in-2026/
[2] Skin Cancer Rise: Could Climate Change Be to Blame? - https://www.aamc.org/news/skin-cancer-rise-could-climate-change-be-blame
[3] Melanoma and Skin Cancer Awareness Month - https://www.aacr.org/patients-caregivers/awareness-months/melanoma-and-skin-cancer-awareness-month/
[4] Over 112,000 Americans Estimated to Be Diagnosed With Invasive Melanoma in 2026 - https://www.curemelanoma.org/blog/over-112-000-americans-estimated-to-be-diagnosed-with-invasive-melanoma-in-2026
[6] Skin Cancer Facts & Statistics - https://www.skincancer.org/skin-cancer-information/skin-cancer-facts/
[8] May Is Skin Cancer Awareness Month - https://www.hopkinsmedicine.org/news/newsroom/news-releases/2026/05/may-is-skin-cancer-awareness-month



