Last updated: May 20, 2026
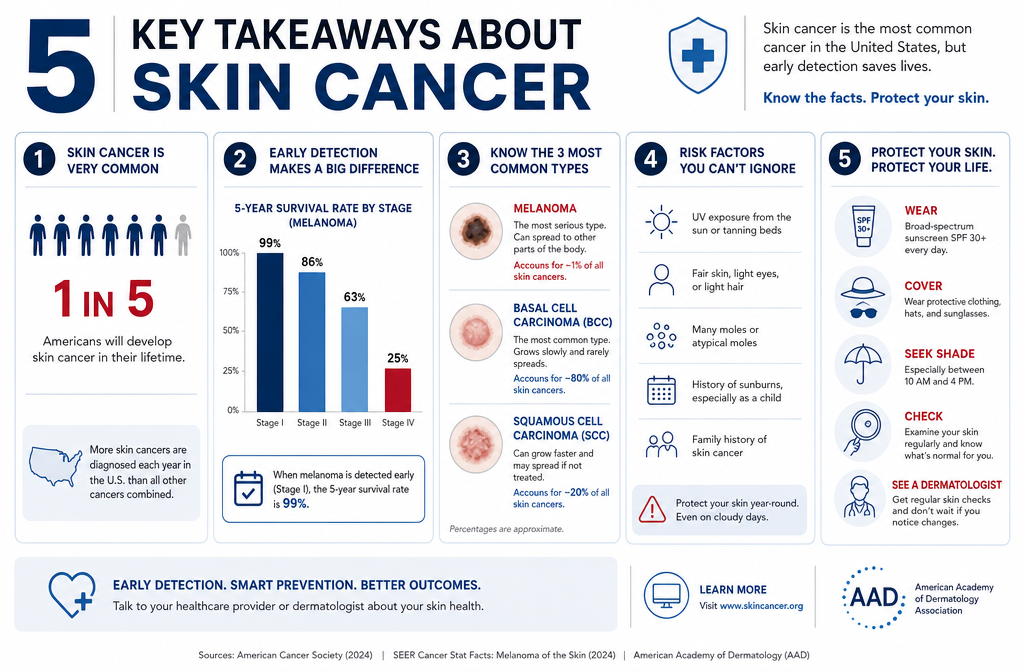
Quick Answer: Skin cancer images show abnormal growths or lesions on the skin that differ from normal moles or spots in shape, color, size, or texture. The three most common types are basal cell carcinoma, squamous cell carcinoma, and melanoma. Reviewing skin cancer images alongside the ABCDE rule helps people recognize warning signs early, when treatment is most effective.
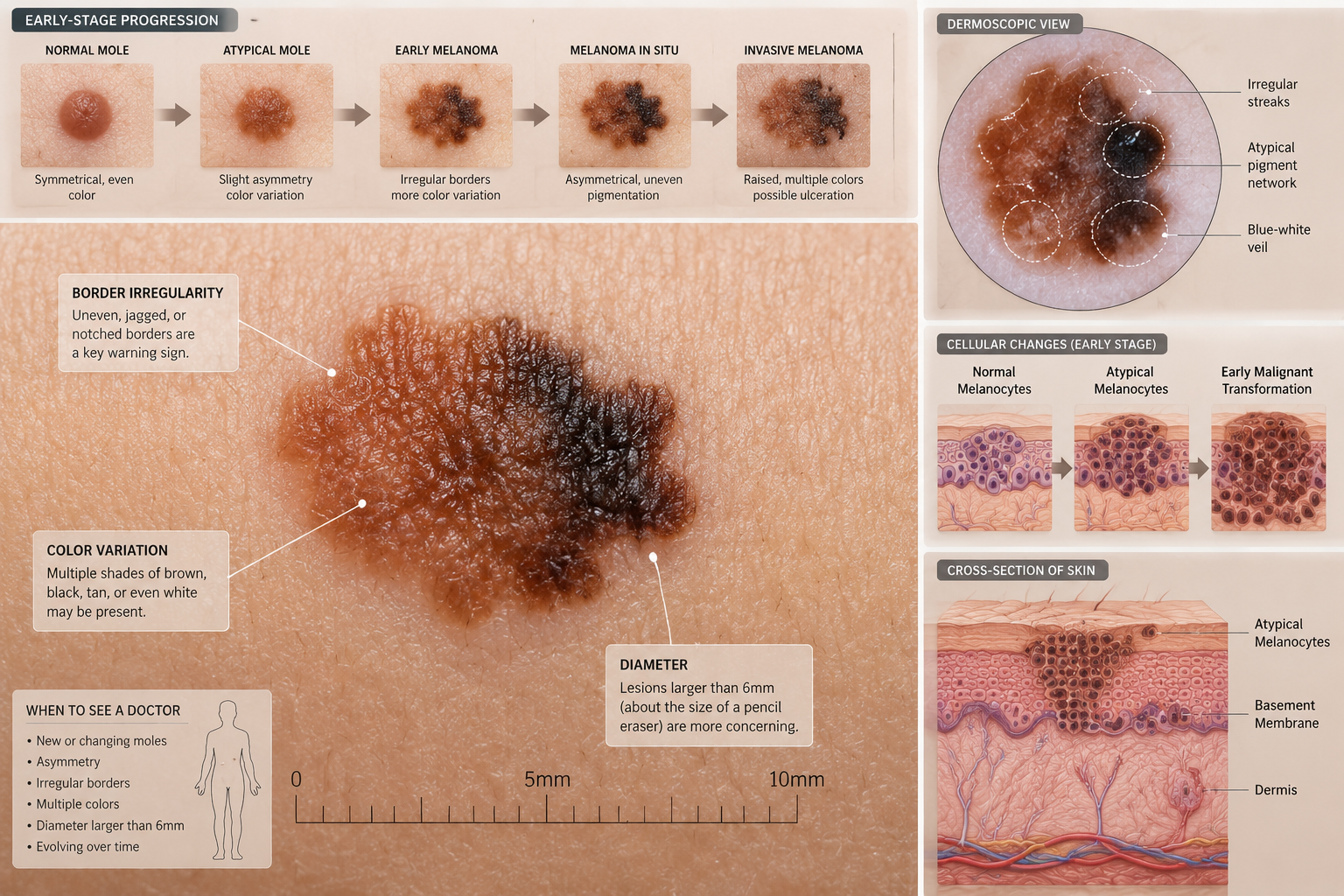
Early-stage skin cancer often looks like a small, unremarkable spot — which is exactly what makes it easy to miss. Depending on the type, it may appear as a pearly bump, a flat scaly patch, a dark irregular mole, or a sore that won't heal.
Here's a breakdown by type:
For a deeper look at early BCC presentations, see this guide on early-stage basal cell carcinoma.
Common mistake: Many people assume skin cancer always looks dramatic or painful. In reality, early lesions are often painless and easy to dismiss as a "regular spot." If a spot is changing or looks different from others, that alone warrants professional evaluation.
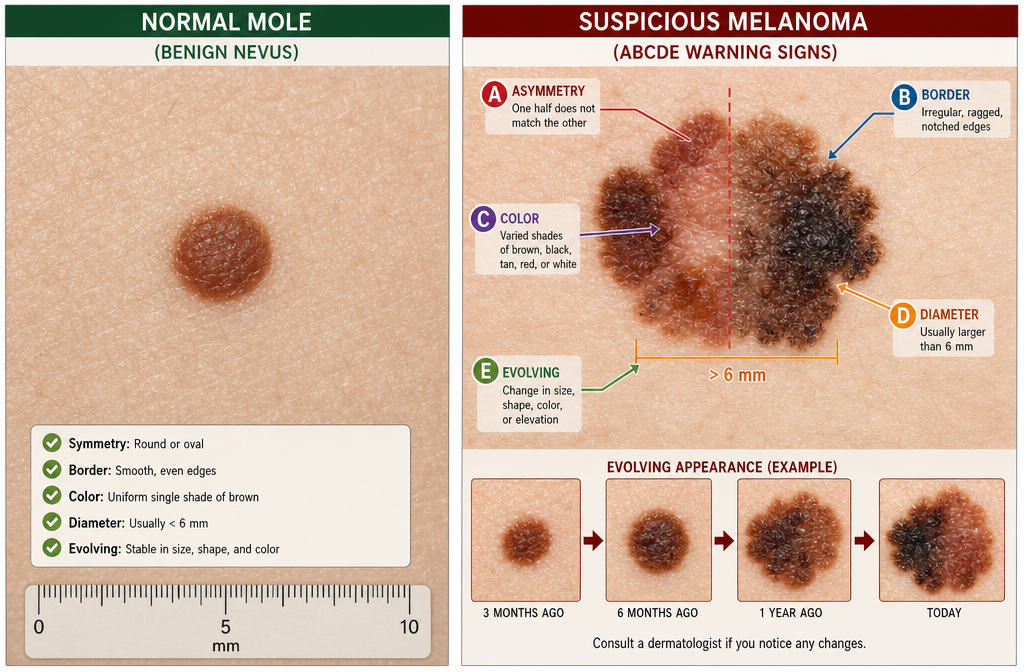
The ABCDE rule is the standard clinical framework for distinguishing a normal mole from a potentially cancerous one. Use it every time you examine skin cancer images or check your own skin.
FeatureNormal MoleMelanoma Warning SignA – AsymmetryBoth halves matchOne half doesn't match the otherB – BorderSmooth, well-defined edgesIrregular, ragged, or blurred edgesC – ColorSingle uniform shade of brownMultiple shades: brown, black, red, white, or blueD – DiameterUsually smaller than 6mm (pencil eraser)Larger than 6mm, though can be smallerE – EvolvingStays the same over timeChanges in size, shape, color, or starts bleeding
Choose professional evaluation if: a spot meets even one of these criteria, or if your gut says something looks "off." Dermatologists call this the "ugly duckling" sign — a lesion that simply looks different from all the others on your body.
For a side-by-side comparison of flat vs. raised moles and cancer risk, see flat mole vs raised mole skin cancer risk.
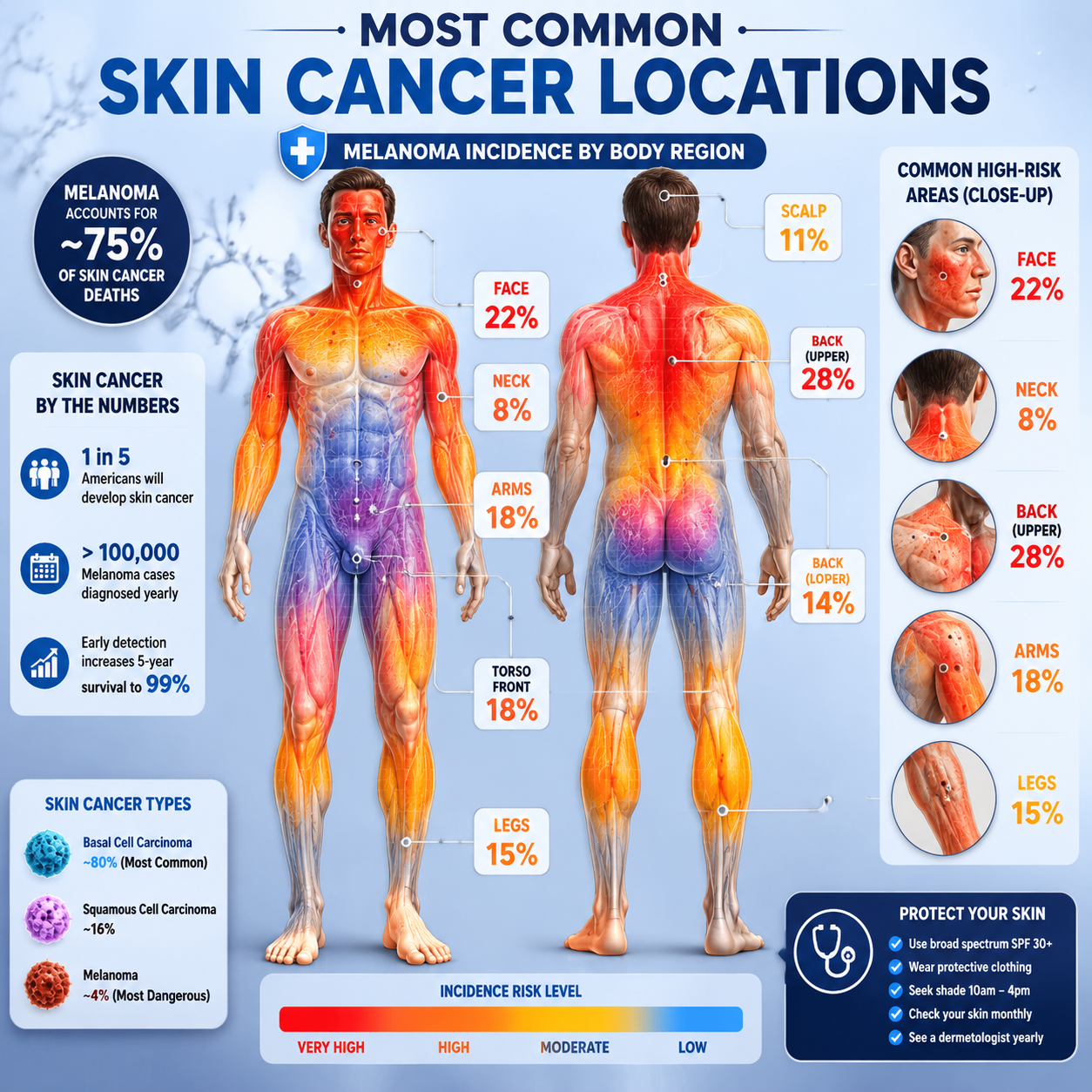
Skin cancers most often appear on areas with the highest cumulative sun exposure, but they can develop anywhere — including spots that never see sunlight.
High-frequency locations:
Less obvious locations (often caught late):
Edge case: Melanoma under a toenail is frequently mistaken for a bruise or fungal infection. If a dark streak under a nail doesn't grow out with the nail over several weeks, see a dermatologist promptly.
For a comprehensive overview of lesion types by location, the guide to 25+ types of skin lesions is a useful reference.
Yes — certain biological and lifestyle factors significantly increase risk. However, skin cancer does not discriminate entirely by skin tone or background.
Higher-risk groups include:
Understanding your Fitzpatrick skin type — a scale that classifies skin by its response to UV exposure — can help gauge baseline risk. See the Fitzpatrick skin type complete guide for details.
Absolutely. Dark-skinned individuals can and do develop skin cancer, and it is often diagnosed at a more advanced stage because both patients and clinicians may not think to look for it.
Melanoma in people with darker skin tones tends to appear in less sun-exposed areas — the palms, soles, under the nails, and inside the mouth. This pattern is called acral lentiginous melanoma, and it accounts for a disproportionate share of melanoma cases in Black, Hispanic, and Asian populations.
Key points:
"Skin cancer in people of color is often caught later, which directly affects survival outcomes. Awareness is the first line of defense." — A principle consistently emphasized in dermatology education.
Most self-checks fail not because people aren't looking, but because they're looking in the wrong places or using the wrong method.
Top self-check mistakes:
A practical self-check routine:
Dermatologists use a layered approach: visual inspection, dermoscopy, and biopsy. No single step alone is sufficient for a confirmed diagnosis.
Step-by-step diagnostic process:
For those in the Greater Toronto Area, the best skin cancer clinic offers board-certified assessment and biopsy services.
Cost depends heavily on location, whether a biopsy is needed, and what insurance or public health coverage applies.
General cost ranges (estimates, subject to change):
ServiceCanada (OHIP-covered)Canada (Private/uninsured)USA (estimate)Dermatologist skin checkOften covered with referral$150–$300 CAD$100–$250 USDDermoscopyOften included$50–$150 CAD add-onVariesSkin biopsyCovered if medically indicated$200–$500 CAD$150–$500+ USDExcision of lesionCovered if malignant$400–$1,200 CAD$500–$3,000+ USD
In Ontario, a referral from a family physician to a dermatologist for a suspicious lesion is typically covered under OHIP. Private clinics offer faster access without a referral. For a curated list of options, see 17+ best skin cancer screening in Toronto.
Decision rule: If you have a suspicious lesion and face a wait for a public dermatologist, a private clinic visit for initial assessment is worth the cost — early detection dramatically changes treatment complexity and outcomes.
Several apps exist that claim to analyze skin cancer images using AI, but their accuracy remains inconsistent and none are approved as diagnostic tools by Health Canada or the FDA.
What the apps can do:
What they cannot do:
Bottom line: Use apps as a tracking and awareness tool, not a diagnostic one. A study published in JAMA Dermatology (2017) found that some smartphone apps misclassified melanomas as benign at rates that would be clinically unacceptable — and technology has improved since then, but regulatory approval for diagnostic use remains limited as of 2026.
Treatment depends on the cancer type, stage, location, and the patient's overall health. Most early-stage skin cancers are highly curable with straightforward procedures.
Common treatment options:
For a full overview of surgical options, see skin cancer surgeries for skin lesions.
Yes — all three major types of skin cancer can spread (metastasize), though the risk varies significantly by type and how early treatment begins.
Early-stage melanoma (confined to the outer skin layer) has a 5-year survival rate above 98% according to the American Cancer Society. Stage IV melanoma, where cancer has spread to distant organs, has a substantially lower survival rate — though immunotherapy has improved outcomes considerably since 2015.
Key point: Metastasis is not inevitable. It is a function of how early the cancer is caught and treated. This is why reviewing skin cancer images and acting on suspicious changes matters.
For most adults with no personal or family history of skin cancer, an annual full-body skin exam by a dermatologist or trained physician is the standard recommendation.
Frequency guidelines by risk level:
Risk ProfileRecommended FrequencyLow risk (no history, fair skin, minimal sun exposure)Every 1–2 yearsModerate risk (fair skin, history of sunburns, 50+ moles)AnnuallyHigh risk (personal/family history of melanoma, immunosuppressed)Every 3–6 monthsPost-treatment surveillanceAs directed by oncologist
When to see a doctor sooner:
For those in Ontario, the Minor Surgery Center's skin cancer screening offers accessible appointments across multiple locations including Toronto, Mississauga, Oakville, and Vaughan.
Q: Can I use skin cancer images online to self-diagnose?
Online skin cancer images are useful for education and awareness, but not for self-diagnosis. Lighting, skin tone, and image quality vary too much for reliable comparison. Use images to learn what warning signs look like, then see a professional for any concerning spot.
Q: What does a cancerous mole feel like?
Most cancerous moles are painless, especially in early stages. Some may itch, bleed, or crust over as they progress. The absence of pain does not mean a lesion is safe.
Q: Is a dark spot on the skin always melanoma?
No. Dark spots have many causes, including age spots, seborrheic keratoses, dermatofibromas, and post-inflammatory hyperpigmentation. A dermatologist can distinguish these from melanoma using dermoscopy. See the guide on age spots vs cancer spots for a practical comparison.
Q: How long does a skin biopsy take to come back?
Most biopsy results return within 5–14 business days, depending on the laboratory and whether additional staining is required.
Q: Can children get skin cancer?
Skin cancer in children is rare but not impossible. Melanoma can occur in adolescents, particularly those with a genetic predisposition (e.g., xeroderma pigmentosum) or a history of severe sunburns. Sun protection habits established in childhood significantly reduce lifetime risk.
Q: What is actinic keratosis and is it skin cancer?
Actinic keratosis (AK) is a pre-cancerous lesion caused by chronic UV exposure. It appears as a rough, scaly patch on sun-exposed skin. Left untreated, a small percentage of AKs progress to squamous cell carcinoma. Treatment is straightforward and highly effective. Learn more in the guide on actinic keratosis to SCC.
Q: Does sunscreen fully prevent skin cancer?
Sunscreen significantly reduces UV exposure and lowers risk, but it does not eliminate it entirely. Broad-spectrum SPF 30 or higher, reapplied every two hours, is the standard recommendation. Protective clothing, shade, and avoiding peak UV hours (10 a.m.–4 p.m.) add further protection.
Q: What is the difference between a skin cancer rash and a regular rash?
A cancer-related skin rash typically doesn't resolve with standard treatments, may be associated with systemic symptoms, and often has an atypical appearance. See the overview of cancer skin rash for a detailed comparison.
Q: Are white spots on the skin a sign of cancer?
White spots are usually benign (e.g., vitiligo, pityriasis alba, or post-inflammatory hypopigmentation), but some can indicate early skin changes worth monitoring. The guide on cancer white spots on skin covers when to be concerned.
Q: What happens if skin cancer is left untreated?
Untreated skin cancer can grow deeper into surrounding tissue, spread to lymph nodes, and eventually metastasize to internal organs. The timeline varies by type — BCC may take years to cause serious harm, while aggressive melanoma can spread within months.
Q: Can removing a mole cause cancer to spread?
No. Properly performed mole removal by a qualified clinician does not cause cancer to spread. This is a common myth. See does removing a mole cause cancer for a full explanation.
Q: What types of skin cancer are most common overall?
Basal cell carcinoma is the most common, followed by squamous cell carcinoma. Melanoma is less common but responsible for the majority of skin cancer deaths. For a complete breakdown, see understanding the 4 main types of skin cancer.
Reviewing skin cancer images is a valuable first step in building awareness — but awareness only matters when it leads to action. Here's a practical checklist for 2026:
Actionable next steps:
If you're in Ontario and want expert assessment, the Minor Surgery Center offers board-certified skin cancer screening and lesion removal across Toronto, Mississauga, Oakville, Vaughan, and surrounding areas — with no long wait times.
Skin cancer is one of the most preventable and treatable cancers when caught early. The difference between a straightforward excision and a complex treatment course often comes down to how quickly a suspicious spot was evaluated. Don't wait.



