Last updated: 2026
Doctors check a mole for cancer by reviewing its history, examining its size, shape, colour, border, surface, and symptoms, and looking for warning signs such as change, bleeding, crusting, itching, or irregular appearance.
At The Minor Surgery Center, mole checks in Toronto are performed by GP Dermatologists. A GP Dermatologist may use a dermatoscope when clinically appropriate.
If a mole or skin lesion requires biopsy, removal, excision, or surgical treatment, patients may be referred or directed to one of TMSC’s board-certified plastic surgeons.
The key distinction is simple:
A mole check is a structured skin assessment. The provider reviews the mole’s history, examines its appearance, checks for warning signs, and decides whether follow-up, monitoring, biopsy, removal, or referral is appropriate.
At TMSC, this assessment is performed by a GP Dermatologist.
A focused mole check may involve one specific lesion. A full-body skin check may be appropriate for patients with multiple moles, risk factors, or broader skin concerns.
No cutting, numbing, or tissue removal happens during a mole check unless a separate procedure is recommended and arranged.
Before examining the mole, the GP Dermatologist may ask questions such as:
Change over time is one of the most important details. A mole that has looked the same for years is different from one that has changed noticeably over weeks or months.
The GP Dermatologist examines the mole under proper lighting and may use a dermatoscope when clinically appropriate.
A dermatoscope is a handheld tool that helps trained providers see structures in the skin that may not be visible to the naked eye.
During the assessment, the provider may look at:
At TMSC, dermoscopy-based mole checks are performed by GP Dermatologists, not plastic surgeons.
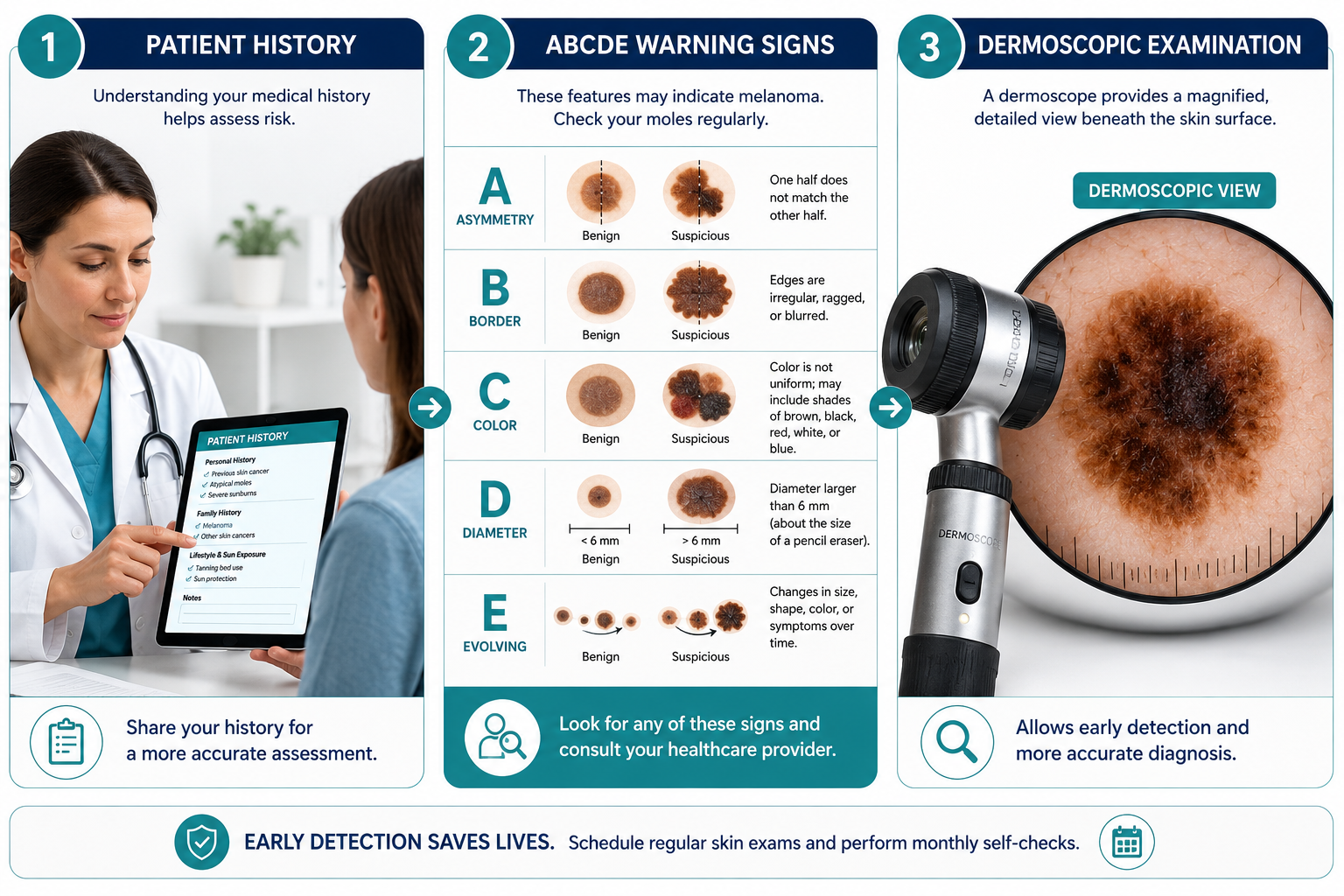
The ABCDE rule is a common framework used to identify moles that may need closer assessment.
One half of the mole does not match the other half.
The edges are irregular, blurred, ragged, or poorly defined.
The mole has multiple colours or uneven colour distribution.
The mole is larger than 6 mm, although concerning lesions can sometimes be smaller.
The mole has changed in size, shape, colour, texture, or symptoms.
The ABCDE rule is useful, but it is not a diagnosis. Some benign moles can look irregular, and some concerning lesions may not match every warning sign.
After the mole check, the GP Dermatologist may recommend one of several next steps.
If the mole does not appear concerning, no treatment may be needed. The provider may explain what changes to watch for and whether follow-up is appropriate.
Some moles may not need immediate removal but may need follow-up if they change. Monitoring recommendations depend on the patient’s risk factors and the appearance of the lesion.
If the lesion requires tissue analysis or removal, the patient may be referred or directed to a plastic surgeon for biopsy, excision, or mole removal.
In some cases, the next step may involve referral to another specialist or a different care pathway, depending on the lesion and clinical situation.
A mole biopsy is a procedure where tissue is removed and sent to a pathology laboratory.
Pathology is what confirms whether the tissue is:
A biopsy may be recommended if a mole has concerning features, has changed, is symptomatic, or cannot be confidently assessed through examination alone.
At TMSC, biopsy and excision are performed by plastic surgeons when appropriate.
The technique depends on the lesion, location, size, depth, and reason for removal.
A shave technique removes the lesion close to the skin surface. It may be used for certain raised lesions.
A punch technique removes a small circular core of tissue. It may be used when a deeper or full-thickness sample is needed.
An excisional biopsy removes the entire lesion with a small margin of surrounding skin. The tissue is then sent to pathology.
This may be used when the full lesion needs to be removed and analyzed.
A mole biopsy or removal is usually performed under local anaesthetic.
The numbing injection may cause a brief sting. Once the area is numb, the procedure itself should not be painful.
After the procedure, patients may have mild tenderness for a short period. The clinic provides aftercare instructions before the patient leaves.
No. A provider can identify concerning features, but visual assessment alone cannot confirm whether a mole is cancerous.
Dermoscopy can provide more information when used by a trained provider, but pathology is still required for confirmation.
If a mole is removed and sent to pathology, the lab report provides the diagnosis and helps guide next steps.
For patients trying to understand different types of skin cancer, TMSC also has resources on skin cancer treatment, basal cell carcinoma removal, squamous cell carcinoma surgery, and melanoma surgery.
A pathology report may describe:
The next step depends on the pathology result, margins, lesion type, and clinical situation.
Some patients may need no further treatment. Others may need additional excision, follow-up, or referral to another specialist.
You may want to book a mole check with a GP Dermatologist if:
A GP Dermatologist can assess whether the lesion needs monitoring, removal, biopsy, or referral.
Book with a plastic surgeon if:
If you are unsure which appointment to book, TMSC can help route you to the appropriate provider.
In Toronto and the GTA, patients may access mole checks, skin assessments, biopsy, and mole removal through different types of providers.
Common options include:
A family doctor can perform an initial assessment and refer to a dermatologist or specialist when needed.
A dermatologist specializes in skin conditions and may provide mole checks, dermoscopy, diagnosis, and treatment planning.
At TMSC, GP Dermatologists provide mole checks, full-body skin checks, and dermoscopy-based assessments when clinically appropriate.
At TMSC, plastic surgeons perform biopsy, mole removal, excision, surgical closure, pathology coordination, and treatment when appropriate.
Mole mapping clinics use photography or imaging to track moles over time. This may be helpful for patients with many moles or higher skin cancer risk.
For patients comparing options, TMSC also has a guide to mole mapping vs. full-body mole checks.
You may also find these pages helpful:
Doctors review the mole’s history, examine its size, shape, colour, border, surface, and symptoms, and look for warning signs. A GP Dermatologist may use a dermatoscope when clinically appropriate. If tissue analysis is needed, biopsy or excision may be recommended.
No. Visual assessment and dermoscopy can identify concerning features, but pathology is needed to confirm whether tissue is benign, atypical, precancerous, or cancerous.
At TMSC, a mole check is performed by a GP Dermatologist. The provider reviews your concern, examines the mole or skin, may use a dermatoscope when appropriate, and recommends the next step.
Yes, GP Dermatologists at TMSC may use dermatoscopes during mole checks when clinically appropriate.
Plastic surgeons at TMSC do not perform dermoscopy-based mole checks. Their role is biopsy, removal, excision, and surgical treatment when needed.
A biopsy may be recommended when a mole has concerning features, has changed, is symptomatic, or needs tissue analysis to confirm what it is.
The area is cleaned and numbed with local anaesthetic. A plastic surgeon removes tissue using the appropriate technique, such as shave, punch, or excisional biopsy. The tissue may then be sent to pathology.
Yes. In some cases, a mole can be removed and sent to pathology during the same procedure.
Timing can vary by lab and clinical situation. The clinic will contact the patient when results are available and explain any recommended next steps.
This depends on your risk factors, mole count, personal history, family history, and whether any lesions are changing. A GP Dermatologist, family doctor, or dermatologist can advise on an appropriate schedule.
The ugly duckling sign refers to a mole or spot that looks noticeably different from your other moles. A lesion that stands out, changes, bleeds, hurts, or looks unusual should be assessed by an appropriate medical provider.
Doctors check moles by reviewing history, examining the skin, looking for warning signs, and deciding whether monitoring, biopsy, removal, or referral is needed.
At The Minor Surgery Center, mole checks are performed by GP Dermatologists, who may use dermatoscopes when clinically appropriate.
If biopsy, removal, excision, or surgical treatment is needed, the patient may be referred or directed to one of TMSC’s plastic surgeons.
If you are worried about a mole and need assessment, book a mole check with a GP Dermatologist.
If a mole has already been assessed and removal or biopsy has been recommended, book for mole removal or surgical treatment.
[1] Screening - https://www.moffitt.org/cancers/melanoma/diagnosis/screening/
[2] Mole Mapping - https://www.aimatmelanoma.org/melanoma-101/early-detection-of-melanoma/mole-mapping/
[4] Skin Cancer Screening: What to Expect During a Dermatology Exam - https://www.dcsionline.com/blog/1431987-skin-cancer-screening-what-to-expect-during-a-dermatology-exam/
[5] Skin Cancer Screening - https://medlineplus.gov/lab-tests/skin-cancer-screening/
[6] SquareMind robotic mole scanning announcement - https://www.instagram.com/p/DXxW19_E8B1/
[7] Melanoma 2026 Cutting Edge Research and Predictions - https://www.theminorsurgerycenter.com/blog/melanoma-2026-cutting-edge-research-and-predictions
[8] ScienceDaily: AI melanoma risk prediction study - https://www.sciencedaily.com/releases/2026/04/260415043612.htm
[9] Screening Moles Cancer - https://www.webmd.com/melanoma-skin-cancer/screening-moles-cancer
[10] PMC review on dermoscopy and AI in melanoma detection - https://pmc.ncbi.nlm.nih.gov/articles/PMC12856975/
Last updated: May 12, 2026



