Last updated: April 7, 2026
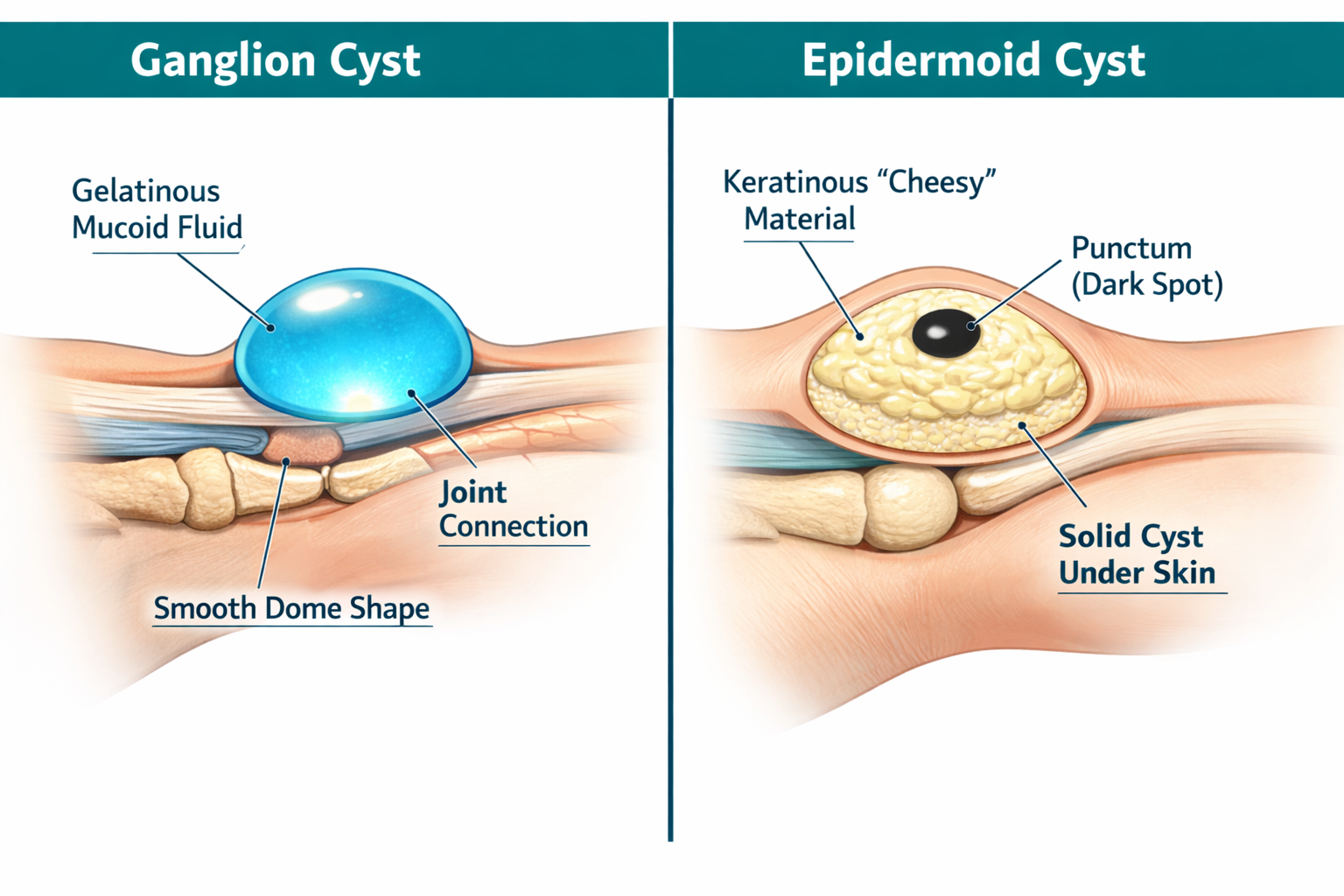
A cyst on the wrist is most likely a ganglion cyst, which accounts for roughly 70% of all hand and wrist lumps and is filled with thick, gel-like fluid [3]. An epidermoid cyst, by contrast, is a solid, skin-derived lump filled with keratin — a cheesy, white material — and is far less common on the wrist specifically. The two look similar on the surface but differ in origin, texture, behavior, and treatment approach.
A ganglion cyst is a benign, fluid-filled sac that forms directly from a joint capsule or tendon sheath. It is the single most common soft-tissue tumor of the hand and wrist, representing approximately 70% of all lesions in that region, with a higher prevalence in women than men [3].
Key characteristics:
Common mistake: Many people assume any wrist lump that fluctuates in size is "just a ganglion." While ganglions do change size with wrist activity and rest, fluctuating size alone does not confirm the diagnosis. A proper clinical exam — or ultrasound — is needed.
An epidermoid cyst (sometimes called an epidermal inclusion cyst) is a benign, slow-growing sac lined with true skin cells. It fills with keratin — the same protein that makes up skin and nails — which accumulates over time into a thick, cheesy material.
Key characteristics:
Epidermoid cysts on the wrist are less common than ganglions but can occur after hand injuries, repeated friction, or previous wrist surgery. For a broader look at how epidermoid cysts compare to other cyst types, see this detailed guide on epidermoid vs. sebaceous vs. pilar cysts.
Pull quote: "A ganglion glows. An epidermoid doesn't. That single transillumination test is often the fastest way to separate the two at the bedside."
The table below summarizes the most clinically useful differences between the two types of wrist cysts.
FeatureGanglion CystEpidermoid CystContentsGelatinous mucoid fluidCheesy keratinous materialTransillumination✅ Positive (glows)❌ Negative (solid)Central punctumAbsentOften presentSkin surfaceNormalNormal; punctum may be visibleConnectionJoint capsule or tendon sheathSkin only (no joint connection)Texture on palpationTense, fluctuantFirm, doughySpontaneous resolution~58% resolve on their own [2]Rarely resolves; tends to growInfection riskLowModerate (can rupture and inflame)Recurrence after aspiration58.1% [1]Not applicable (aspiration not standard)Recurrence after excision20.8% [1]Low with complete wall removal [2]
Choose "watch and wait" if: The lump is painless, small, and consistent with a ganglion on clinical exam — up to 58% resolve without any intervention [2].
Choose surgical excision if: The cyst is painful, growing, interfering with wrist function, cosmetically bothersome, or is an epidermoid cyst (which will not resolve on its own).
Clinical examination alone is adequate for classic presentations of a cyst on the wrist — ganglion vs. epidermoid distinction is usually possible at the bedside using transillumination as the key test [2].
Diagnostic steps, in order:
Edge case: An occult ganglion is a ganglion too small to see or feel but large enough to cause wrist pain. MRI is the best tool to find these. If wrist pain has no obvious cause, an occult ganglion should be on the differential.
For concerns about whether a wrist or finger lump could be something more serious, this resource on cancerous cysts on the finger provides useful context.
Treatment depends on the cyst type, size, symptoms, and patient preference. The right approach differs significantly between ganglion and epidermoid cysts.
Option 1 — Observation (watchful waiting)
First-line management for asymptomatic or mildly symptomatic ganglions. Approximately 58% resolve spontaneously over time [2]. No treatment is needed if the cyst is not painful and not limiting wrist use.
Option 2 — Needle aspiration (with or without steroid injection)
A needle drains the fluid. Quick, done in-office, no incision. However, the recurrence rate is high: 58.1% at 12 months [1]. Patient satisfaction after aspiration is 77.4%, with a mean pain reduction of 3.5 points on a visual analog scale [1]. Best suited for patients who want temporary relief or are not candidates for surgery.
Option 3 — Surgical excision
The most durable option. Recurrence rate drops to 20.8% at 12 months [1]. Patient satisfaction reaches 94.3%, with a mean pain reduction of 5.6 points [1]. Complications occurred in only 5.7% of surgical cases in one study of 84 patients, and the difference in complication rates between excision and aspiration was not statistically significant [1]. Minimally invasive arthroscopic approaches are gaining ground, showing decreased postoperative complications and recurrence rates compared to open excision [4].
Surgical excision under local anesthesia is the definitive treatment. The entire cyst wall must be removed intact; leaving any wall behind almost guarantees recurrence [2]. Aspiration is not a standard option because the solid keratin content cannot be drained. For a detailed walkthrough of what the procedure involves, see this guide on epidermoid cyst removal surgery.
Important: Attempting to drain a ganglion cyst at home — including the old "Bible book" method of striking it — is not recommended. It can cause injury, infection, and incomplete treatment. Read more about why draining a ganglion cyst yourself is risky.
Most wrist cysts are benign, but certain signs warrant prompt medical evaluation rather than watchful waiting.

See a doctor promptly if:
Reassuring signs (lower urgency):
For patients across the Greater Toronto Area, clinics offering professional assessment and removal include locations in Mississauga, North York, Markham, and Whitby.
For ganglion cysts, leaving it alone is often the right call. About 58% resolve without treatment [2], and watchful waiting carries no medical risk as long as the diagnosis is clear and symptoms are absent or mild.
For epidermoid cysts, the situation is different. These cysts do not resolve on their own. Over time, they tend to:
Bottom line: A confirmed, asymptomatic ganglion cyst can reasonably be observed. A confirmed epidermoid cyst on the wrist should be removed electively before it causes problems. To understand recurrence risk across different removal methods, this comparison of cyst drainage vs. full excision is worth reading.
Yes. Not every wrist lump is a ganglion or epidermoid cyst. Several other conditions can produce similar lumps, and getting the diagnosis right matters for treatment.
Other wrist lumps to consider:
Ultrasound quickly separates most of these. If ultrasound findings are atypical, MRI provides the next level of detail [2].
Q: Can a ganglion cyst on the wrist go away on its own?
Yes. Approximately 58% of ganglion cysts resolve spontaneously over time without any treatment [2]. Watchful waiting is a legitimate first option for asymptomatic cysts.
Q: Does a ganglion cyst hurt?
Not always. Many ganglion cysts are painless. When pain occurs, it is usually with extreme wrist positions or repetitive activity. A cyst pressing on a nearby nerve can cause aching, weakness, or tingling.
Q: How can I tell at home if my wrist lump is a ganglion or an epidermoid cyst?
Press a small flashlight firmly against the lump in a dark room. If it glows, it is likely a ganglion (fluid-filled). If it stays dark and solid-feeling, it is more likely an epidermoid cyst. This test is a useful guide but not a substitute for a clinical exam.
Q: Is surgery always necessary for a wrist cyst?
No. For ganglion cysts, surgery is one of three options — the others being observation and aspiration. For epidermoid cysts, surgical excision is the standard recommendation because they do not resolve and aspiration is not effective [2].
Q: What is the recurrence rate after ganglion cyst surgery?
About 20.8% at 12 months after surgical excision, compared to 58.1% after needle aspiration [1]. Arthroscopic techniques may reduce recurrence further [4].
Q: Can an epidermoid cyst on the wrist become cancerous?
Malignant transformation of an epidermoid cyst is extremely rare. However, any rapidly growing, painful, or fixed wrist lump should be evaluated promptly to rule out malignancy.
Q: How long does recovery take after wrist cyst removal?
Most patients return to light daily activities within a few days. Full wrist function typically returns within 2 to 6 weeks depending on cyst size, location, and surgical approach. For more detail, see this overview of cyst removal recovery time.
Q: Will a wrist cyst removal leave a scar?
A small scar is expected at the incision site. Skilled surgical technique and proper aftercare minimize scarring. The scar typically fades significantly over 6 to 12 months. More information is available on whether cyst removal leaves a scar.
Q: Is aspiration painful?
The skin is numbed with local anesthetic before the needle is inserted, so the procedure itself is minimally painful. Some discomfort may follow for a day or two.
Q: Can children get ganglion cysts on the wrist?
Yes. Ganglion cysts occur across all age groups, including children and adolescents. Management principles are similar, though observation is preferred even more strongly in younger patients given the high spontaneous resolution rate.
A cyst on the wrist — ganglion vs. epidermoid — is a distinction that directly shapes what happens next. Here is a simple decision path:
For a broader understanding of the many types of cysts and how they differ, the 20+ types of cysts guide is a useful reference. Patients in the Toronto area can find experienced surgical teams for assessment and removal at The Minor Surgery Center.
[1] ijoro - https://www.ijoro.org/index.php/ijoro/article/view/4071
[2] What Is The Diagnosis And Treatment For A Patient - https://www.droracle.ai/articles/732201/what-is-the-diagnosis-and-treatment-for-a-patient
[3] Gmj.2026 - https://gazimedj.com/articles/evaluation-of-the-characteristics-of-hand-and-wrist-ganglion-cysts-and-their-relationship-with-ligamentous-injury/gmj.2026.4359
[4] Pmc11632804 - https://pmc.ncbi.nlm.nih.gov/articles/PMC11632804/
[8] A Rare Case Of Giant Cell Tumor Of The Extensor Hallucis Longus Tendon - https://auctoresonline.org/article/a-rare-case-of-giant-cell-tumor-of-the-extensor-hallucis-longus-tendon



