Last updated: March 5, 2026
Waking up with numb, tingling fingers isn't just annoying—it's often the first sign of carpal tunnel syndrome. But not all cases are the same. Carpal Tunnel Severity: Mild vs Moderate vs Severe represents distinct stages of median nerve compression, each with different symptoms, functional impacts, and treatment approaches. Understanding where you fall on this spectrum determines whether you need a simple wrist splint, corticosteroid injections, or surgical intervention.
The difference between mild and severe carpal tunnel syndrome isn't just about pain intensity. Mild cases involve occasional sensory symptoms like tingling without motor weakness, while severe cases feature muscle atrophy, loss of grip strength, and inability to perform basic hand functions. Moderate severity sits in between, with noticeable functional limitations but without permanent muscle damage. Each stage requires a specific treatment strategy, and choosing the wrong approach can lead to permanent nerve damage or unnecessary surgery.
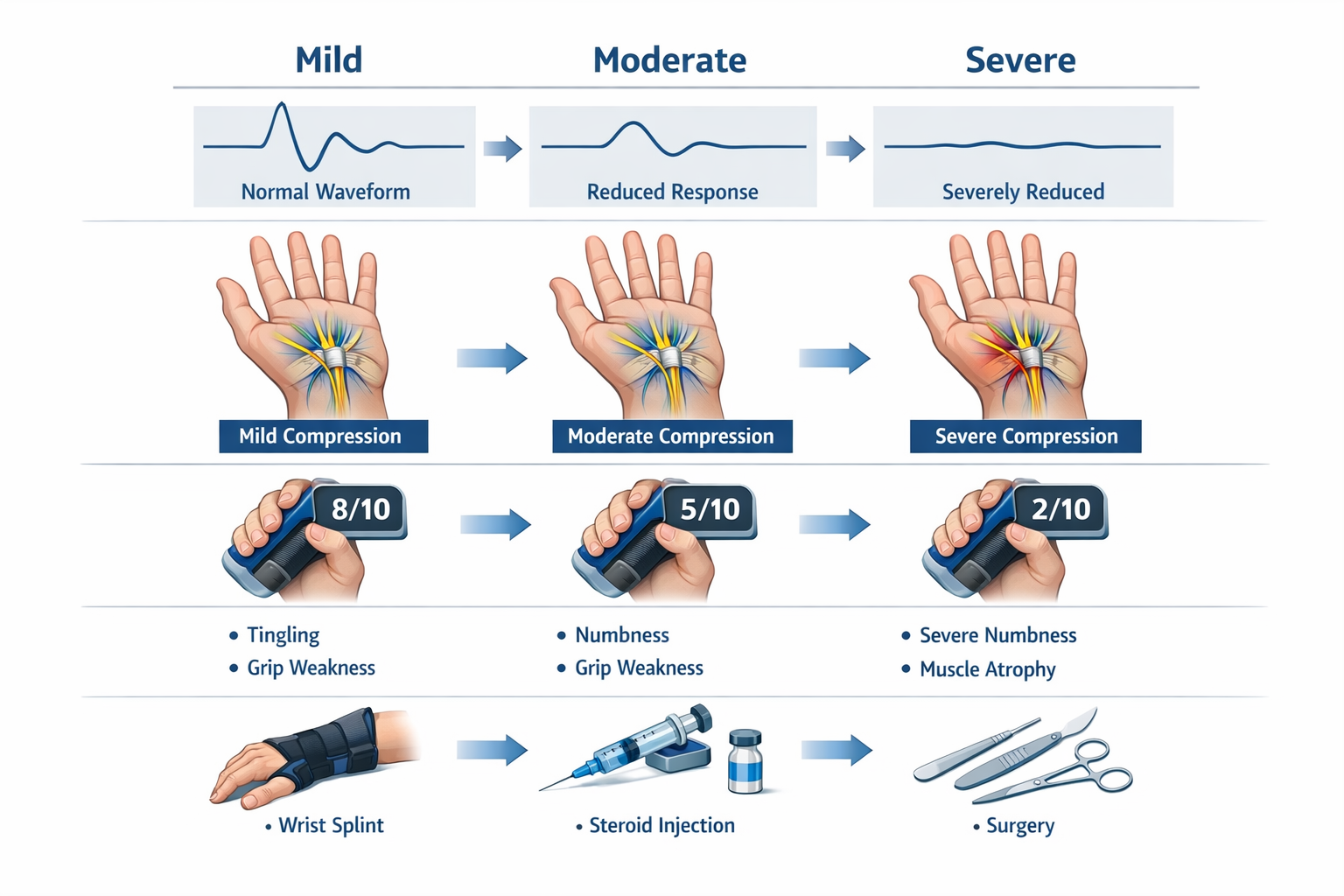
Carpal tunnel syndrome severity is classified into three main stages based on symptom intensity, functional impairment, and nerve conduction study findings. Mild cases feature occasional tingling and numbness without weakness, treated with splinting and ergonomic modifications. Moderate cases show persistent symptoms with noticeable grip weakness and functional limitations, typically managed with corticosteroid injections and physical therapy. Severe cases involve constant numbness, muscle atrophy, significant functional loss, and usually require surgical carpal tunnel release for recovery.
Carpal tunnel syndrome progresses through three distinct severity stages: mild, moderate, and severe. Each stage is defined by specific symptom patterns, functional limitations, and objective findings on nerve conduction studies.[1]
Mild carpal tunnel syndrome presents with:
Moderate carpal tunnel syndrome is characterized by:
Severe carpal tunnel syndrome involves:
The progression between stages isn't always linear. Some patients remain at mild severity for years, while others progress rapidly from moderate to severe within months, particularly if the underlying cause (repetitive strain, pregnancy, diabetes) isn't addressed.
Choose conservative treatment if: You have mild symptoms that started recently (within 3-6 months), symptoms occur mainly at night, and you have no muscle weakness or atrophy.
Consider injections or advanced therapy if: You have moderate symptoms lasting more than 3 months, noticeable functional limitations, or mild symptoms that haven't improved with 6 weeks of splinting.
Discuss surgery if: You have severe symptoms with muscle atrophy, constant numbness, significant functional loss, or moderate symptoms that haven't responded to 3-6 months of conservative treatment including injections.[2]
Physicians use a combination of clinical examination findings, validated scoring tools, and electrodiagnostic studies to objectively measure carpal tunnel severity. The CTS-6 Evaluation Tool is a validated clinical scoring instrument that assigns points based on six key factors.[2]
FactorPointsDescriptionSymptom diagram2Classic pattern: numbness/tingling in thumb, index, middle, and radial half of ring fingerSymptom duration1Symptoms present for more than 4 monthsNocturnal symptoms1Numbness or tingling that wakes patient from sleepSensory deficit1Reduced sensation to light touch in median nerve distributionThenar atrophy1Visible or palpable wasting of thumb base musclesPositive Tinel sign4Tingling sensation when tapping over carpal tunnel
A total score greater than 12 indicates an 80% probability of carpal tunnel syndrome diagnosis.[2] However, this tool focuses on diagnosis rather than severity grading.
Phalen test (wrist flexion test) is the most sensitive diagnostic test. The patient holds both wrists in full flexion (bent downward) for 30-60 seconds. Symptom onset within 30 seconds indicates a positive result and suggests moderate to severe nerve compression.[2]
Tinel sign involves tapping or pressing over the median nerve at the wrist crease for 30 seconds. A positive test produces tingling or electric shock sensations radiating into the fingers.[2]
Durkan test (carpal compression test) applies direct pressure over the carpal tunnel for 30 seconds. This test has high specificity for carpal tunnel syndrome when positive.
Thenar muscle strength testing assesses thumb opposition strength (pressing thumb tip to pinky tip against resistance). Weakness indicates motor nerve involvement and at least moderate severity.
Nerve conduction velocity (NCV) and electromyography (EMG) provide objective measurements of nerve function and are the gold standard for severity grading:
Common mistake: Relying solely on symptom severity without objective testing. Some patients with severe nerve damage have minimal symptoms because the nerve is so damaged it no longer transmits pain signals effectively. Conversely, some patients with mild objective findings report severe symptoms due to low pain tolerance or anxiety.
Edge case: Patients with diabetes or other neuropathies may have abnormal baseline nerve conduction, making severity assessment more complex. In these cases, comparing the affected hand to the unaffected side helps determine carpal tunnel-specific changes.
For more information on distinguishing carpal tunnel from similar conditions, see our guide on carpal tunnel vs tendonitis vs arthritis.
Mild carpal tunnel syndrome presents with intermittent sensory symptoms without motor weakness or functional impairment. Patients typically experience numbness, tingling, or burning sensations in the thumb, index, middle, and radial half of the ring finger—the distribution of the median nerve.[1]
Nocturnal symptoms are the hallmark of mild carpal tunnel syndrome. Patients wake up with numb or tingling hands, often shaking their hands to "wake them up" or restore sensation. This occurs because most people sleep with wrists flexed, which increases pressure in the carpal tunnel.[2]
Intermittent daytime symptoms occur during or after activities involving repetitive wrist movements or sustained gripping:
Symptom relief happens quickly with activity modification. Shaking the hand, changing position, or resting provides immediate improvement.
No functional limitations exist in mild cases. Patients can perform all normal activities, including:
Normal physical examination findings include:
Mild symptoms typically last seconds to minutes and resolve spontaneously or with simple interventions like hand shaking. Symptoms may occur daily but don't persist continuously throughout the day.
Choose conservative management if: Your symptoms started within the past 3-6 months, occur mainly at night or with specific activities, resolve with rest, and don't interfere with work or daily tasks.
Common mistake: Ignoring mild symptoms because they're "not that bad." Early intervention with ergonomic modifications and nighttime splinting can prevent progression to moderate or severe stages.
Many patients with mild carpal tunnel syndrome experience flare-ups triggered by increased hand use, making symptom patterns variable over time.
Moderate carpal tunnel syndrome represents a significant progression from mild disease, with persistent symptoms, noticeable functional limitations, and early motor involvement. Patients at this stage experience symptoms that interfere with daily activities and work performance.[1]
Persistent sensory symptoms occur throughout the day and night, not just with specific activities:
Functional impairment becomes noticeable:
Motor weakness begins to appear:
Pain patterns expand beyond the hand:
Physical examination findings:
Moderate carpal tunnel syndrome affects work productivity and quality of life. Patients report:
Treatment responsiveness becomes more limited at this stage. Research shows that patients with greater baseline symptom severity and those who have failed one nonsurgical intervention are less likely to respond to continued conservative management.[3]
Choose escalated treatment if: You have moderate symptoms lasting more than 6-8 weeks despite splinting and activity modification, symptoms that interfere with work or sleep, or measurable weakness on examination.
For patients experiencing severe nighttime symptoms, our guide on carpal tunnel night pain provides specific management strategies.
Severe carpal tunnel syndrome involves significant motor and sensory dysfunction with permanent structural changes to the median nerve and muscles. This stage represents advanced disease requiring urgent treatment to prevent irreversible damage.[1]
Constant sensory loss replaces intermittent symptoms:
Visible muscle atrophy is the defining feature:
Significant motor weakness impairs hand function:
Functional disability affects most hand activities:
Pain patterns may paradoxically decrease:
Nerve conduction studies in severe carpal tunnel syndrome show:
Surgical outcomes are less predictable in severe cases. Patients with severe EMG/NCV findings demonstrate less improvement after surgery compared to those with moderate findings, because permanent nerve and muscle damage may not fully recover even after pressure is relieved.[2]
Urgent surgical consultation is needed if: You have visible thenar atrophy, constant numbness, inability to oppose your thumb, or significant functional disability. Delaying surgery in severe cases risks permanent nerve damage and incomplete recovery.
Edge case: Some patients develop severe carpal tunnel syndrome rapidly (over weeks to months) due to acute causes like wrist fracture, pregnancy, or inflammatory conditions. These cases may have better surgical outcomes than chronic severe cases because permanent structural changes haven't yet occurred.
For information on returning to work after treatment, see our guide on desk job vs manual labor return to work after carpal tunnel syndrome.

Mild carpal tunnel syndrome responds well to conservative, nonsurgical treatments. The primary goals are reducing median nerve pressure, preventing symptom progression, and avoiding the need for injections or surgery.[2][3]
Nighttime wrist splinting is the cornerstone of mild carpal tunnel treatment:
Choose a splint that keeps the wrist in neutral position without forcing extension. For guidance, see our article on choosing the right carpal tunnel brace or splint.
Activity modification reduces repetitive strain:
Ergonomic workplace adjustments:
For specific product recommendations, see our guide on best ergonomic gadgets for preventing carpal tunnel.
Hand and wrist exercises improve flexibility and reduce stiffness:
Our carpal tunnel exercises and stretches guide provides detailed instructions, or try our 10-minute daily carpal tunnel exercise routine.
Anti-inflammatory measures:
Improvement timeline for conservative treatment:
Success indicators that conservative treatment is working:
Treatment failure is indicated by:
When to escalate treatment: If conservative measures don't provide significant improvement within 6-8 weeks, or if symptoms progress despite treatment, consider advancing to corticosteroid injections or physical and occupational therapy techniques.
Common mistake: Inconsistent splint use. Wearing the splint only occasionally or stopping after a few nights of improvement leads to symptom recurrence. Splints must be worn nightly for the full 6-12 week course.
Moderate carpal tunnel syndrome typically requires more aggressive intervention than splinting alone. The standard approach combines conservative measures with corticosteroid injections and may include occupational therapy.[2][3]
Mechanism: Corticosteroid injections reduce inflammation and swelling within the carpal tunnel, decreasing pressure on the median nerve.
Technique: A healthcare provider injects a mixture of corticosteroid (typically methylprednisolone or triamcinolone) and local anesthetic into the carpal tunnel using ultrasound guidance or anatomical landmarks.
Expected outcomes:
Repeat injections: If symptoms recur after initial relief, a second injection may be given after 6 weeks to 3 months. More than 2-3 injections are generally not recommended due to risk of tendon weakening.
Predictors of poor response:
Splinting remains important even with injections:
Occupational therapy is recommended as part of comprehensive nonsurgical management for moderate carpal tunnel syndrome.[2][3]
Components include:
Duration: Typically 4-8 sessions over 6-12 weeks, with a home exercise program continued long-term.
After 3-6 months of conservative treatment (splinting, injections, therapy), reassessment determines next steps:
Continue conservative treatment if:
Consider surgery if:
Research shows that patients with greater symptom severity at baseline and previous failure of one nonsurgical intervention are less likely to respond to continued conservative management, making surgery a more appropriate option.[3]
For more information on treatment options in specific locations, see our guides on carpal tunnel treatment in Mississauga and best carpal tunnel treatment in Vaughan.
Carpal tunnel release surgery becomes necessary when conservative treatments fail to provide adequate relief or when patients present with severe disease. Surgery is the definitive treatment that reliably decompresses the median nerve by cutting the transverse carpal ligament.[2]
Absolute indications:
Relative indications:
Open carpal tunnel release:
Endoscopic carpal tunnel release:
Both techniques have success rates exceeding 90% for appropriate candidates.[2]
Symptom relief timeline:
Factors affecting outcomes:
Success rates by severity:
Immediate postoperative period (0-2 weeks):
Early recovery (2-6 weeks):
Full recovery (6-12 weeks):
For detailed recovery information, see our comprehensive guide on carpal tunnel surgery recovery: what to expect.
Common mistake: Delaying surgery too long in severe cases. Waiting until severe muscle atrophy develops reduces the likelihood of complete recovery, as prolonged nerve compression causes permanent damage.
Edge case: Some patients with severe EMG findings but minimal symptoms may not need immediate surgery. However, these cases require close monitoring, as the discrepancy suggests the nerve is so damaged it's not transmitting signals effectively, which can worsen without intervention.
For information about surgical options, see our page on carpal tunnel syndrome surgery in Toronto.
Yes, mild carpal tunnel syndrome can progress to moderate and eventually severe disease if left untreated or if underlying causes aren't addressed. However, progression isn't inevitable, and many patients remain at mild severity for years with appropriate management.
Modifiable risk factors:
Non-modifiable risk factors:
Medical conditions that accelerate progression:
For pregnancy-specific information, see our article on carpal tunnel syndrome and pregnancy.
Typical progression patterns:
Warning signs of progression:
Early intervention is the most effective strategy:
Monitoring strategy:
When progression occurs despite treatment:
Edge case: Some patients experience temporary severe symptoms during pregnancy or after wrist injury that resolve completely once the precipitating factor resolves. These cases don't represent true progression of chronic carpal tunnel syndrome.
For information on whether symptoms can resolve without intervention, see our article on can carpal tunnel go away on its own.
Determining your carpal tunnel severity requires a combination of self-assessment, clinical evaluation, and objective testing. While you can estimate severity based on symptoms, definitive classification requires medical evaluation.
You likely have MILD carpal tunnel syndrome if:
You likely have MODERATE carpal tunnel syndrome if:
You likely have SEVERE carpal tunnel syndrome if:
Phalen test (self-administered):
Tinel test (self-administered):
Grip strength comparison:
For more detailed self-testing instructions, see our guide on home tests for carpal tunnel.
Immediate evaluation needed if:
Routine evaluation recommended if:
Clinical examination includes:
Electrodiagnostic testing (when indicated):
Imaging studies (rarely needed):
Common mistake: Assuming you have mild disease because pain isn't severe. Severe carpal tunnel syndrome sometimes causes less pain than moderate disease because the nerve is so damaged it doesn't transmit pain signals effectively. Numbness pattern, weakness, and muscle atrophy are more reliable severity indicators than pain intensity.
For information on conditions that can be confused with carpal tunnel syndrome, see our article on carpal tunnel syndrome misdiagnosis.
How long does it take for mild carpal tunnel to become severe?
Progression from mild to severe carpal tunnel syndrome varies widely, ranging from 6 months to several years or never. Most patients with mild disease who receive early treatment and modify aggravating activities remain stable or improve. Those with untreated mild disease and continued exposure to risk factors (repetitive work, obesity, diabetes) may progress to moderate severity within 1-2 years and severe within 2-5 years. Rapid progression (within 6-12 months) occurs in 10-20% of cases, typically with underlying medical conditions or high-intensity occupational exposure.
Can you have severe carpal tunnel without pain?
Yes, severe carpal tunnel syndrome can present with minimal or no pain. Paradoxically, some patients with the most severe nerve damage report less pain because the nerve is so compressed it no longer effectively transmits pain signals. These patients typically have constant numbness, significant weakness, and visible muscle atrophy despite minimal pain. Relying on pain intensity alone to assess severity can be misleading—numbness pattern, motor weakness, and muscle wasting are more reliable indicators of severe disease.
Is surgery always needed for severe carpal tunnel syndrome?
Surgery is almost always recommended for severe carpal tunnel syndrome, particularly when thenar muscle atrophy is present. Conservative treatments rarely provide adequate relief in severe cases, and delaying surgery risks permanent nerve damage and incomplete recovery. However, some patients with severe disease who are poor surgical candidates due to medical comorbidities may continue conservative management with realistic expectations of symptom control rather than cure. The decision should be made in consultation with a hand surgeon after discussing risks, benefits, and expected outcomes.
How accurate are nerve conduction studies for determining severity?
Nerve conduction studies are highly accurate for objectively measuring carpal tunnel severity and have become the gold standard for severity classification. They provide quantitative data on nerve function that correlates well with clinical severity in most cases. However, 10-15% of patients with clinical carpal tunnel syndrome have normal or minimally abnormal nerve studies, particularly in early or mild disease. Conversely, some patients with abnormal studies report minimal symptoms. Severity assessment should combine clinical findings, functional impact, and electrodiagnostic results rather than relying on any single measure.
What percentage of mild carpal tunnel cases need surgery eventually?
Approximately 20-30% of patients with mild carpal tunnel syndrome eventually require surgery, typically after progression to moderate or severe disease or failure of conservative treatments. The remaining 70-80% achieve adequate symptom control with conservative measures (splinting, activity modification, ergonomic changes) or have symptoms that resolve spontaneously. Early intervention with appropriate conservative treatment significantly reduces the likelihood of progression and need for surgery. Patients who address underlying risk factors and consistently use conservative treatments have the lowest surgery rates.
Can moderate carpal tunnel syndrome be reversed without surgery?
Moderate carpal tunnel syndrome can improve significantly with nonsurgical treatment, though "reversal" implies complete resolution which is less common at this stage. Approximately 50-70% of moderate cases achieve meaningful symptom improvement with corticosteroid injections combined with splinting and occupational therapy. However, many patients experience symptom recurrence within 6-12 months and eventually require surgery for definitive treatment. True reversal (complete resolution without recurrence) is more likely in cases with identifiable temporary causes like pregnancy or acute wrist injury that resolve on their own.
How do you distinguish between moderate and severe carpal tunnel syndrome?
The key distinguishing feature is thenar muscle atrophy—visible or palpable wasting of the thumb base muscles indicates severe disease. Other differences include: moderate cases have intermittent or partial numbness while severe cases have constant numbness; moderate cases have measurable but functional grip strength (typically 10-25% weaker) while severe cases have significant weakness (50%+ reduction); moderate cases can perform most activities with difficulty while severe cases have major functional disability. Nerve conduction studies show moderate slowing in moderate cases versus marked slowing or absent signals in severe cases. When in doubt, medical evaluation with electrodiagnostic testing provides objective classification.
What happens if you don't treat mild carpal tunnel syndrome?
Untreated mild carpal tunnel syndrome follows one of three paths: spontaneous improvement (20-30% of cases), stable symptoms that remain mild (30-40%), or progression to moderate or severe disease (30-50%). The outcome depends on whether underlying causes persist or resolve. Patients who continue repetitive hand activities, have obesity, diabetes, or other risk factors are more likely to progress. Those with temporary causes (pregnancy, acute injury) often improve spontaneously. The safest approach is early conservative treatment (splinting, ergonomic modifications) which has minimal risk and can prevent progression in most cases.
Are there any warning signs that carpal tunnel is getting worse?
Yes, several warning signs indicate progression: increasing frequency of symptoms (from occasional to daily to constant), development of daytime symptoms when you previously had only nighttime symptoms, new onset of weakness or dropping objects, symptoms that no longer respond to measures that previously helped (shaking hands, changing position), difficulty with tasks you could previously perform easily (buttoning, writing, gripping), and constant numbness replacing intermittent tingling. Any of these changes warrant medical evaluation and potential treatment escalation.
Can carpal tunnel severity be different in each hand?
Yes, carpal tunnel severity commonly differs between hands. Most people have one dominant hand that performs more repetitive activities and develops more severe disease first. Bilateral carpal tunnel syndrome (affecting both hands) occurs in 50-60% of patients, but severity is usually asymmetric. The dominant hand typically has more severe symptoms and progresses faster. Some patients have symptomatic disease in one hand and subclinical (no symptoms but abnormal nerve studies) disease in the other. Each hand should be evaluated and treated based on its individual severity rather than assuming both hands require the same treatment.
How long should you try conservative treatment before considering surgery?
For mild carpal tunnel syndrome, try conservative treatment (splinting, activity modification, ergonomics) for at least 6-12 weeks before considering injections or surgery. For moderate severity, attempt conservative treatment plus corticosteroid injection for 3-6 months before surgery. For severe carpal tunnel with muscle atrophy, surgery should be considered promptly rather than prolonging conservative treatment, as delays risk permanent nerve damage. These timelines assume consistent adherence to treatment—if you're not improving after appropriate conservative treatment duration, continuing the same approach is unlikely to help.
Does carpal tunnel severity affect surgical success rates?
Yes, severity significantly impacts surgical outcomes. Mild to moderate cases have 95%+ excellent to good outcomes with complete or near-complete symptom resolution. Severe cases without muscle atrophy achieve 85-90% good outcomes. Severe cases with thenar atrophy have 70-80% improvement rates, but often retain some residual numbness and weakness because prolonged nerve compression causes permanent damage. Patients with the most severe nerve conduction study findings show less improvement after surgery than those with moderate findings. This is why early surgical intervention for appropriate candidates produces better outcomes than delaying until severe atrophy develops.
Understanding Carpal Tunnel Severity: Mild vs Moderate vs Severe is essential for choosing the right treatment approach and preventing permanent nerve damage. Mild carpal tunnel syndrome, characterized by intermittent tingling and numbness without weakness, responds well to conservative measures like nighttime splinting and ergonomic modifications. Moderate severity, with persistent symptoms and noticeable functional limitations, typically requires corticosteroid injections combined with occupational therapy. Severe carpal tunnel syndrome, marked by constant numbness, muscle atrophy, and significant weakness, usually necessitates surgical release for optimal outcomes.
The key to successful management is early recognition and appropriate intervention for your severity stage. Mild cases treated promptly rarely progress to severe disease, while delayed treatment of severe cases risks incomplete recovery even after surgery. Electrodiagnostic studies provide objective severity measurement when clinical assessment is uncertain, helping guide treatment decisions and predict outcomes.
If you have mild symptoms:
If you have moderate symptoms:
If you have severe symptoms:
For all severity levels:
Remember that carpal tunnel syndrome is a treatable condition with excellent outcomes when managed appropriately for severity stage. Whether you need simple splinting, injections, or surgical release, early intervention prevents progression and preserves hand function for years to come.
For comprehensive information about carpal tunnel syndrome, visit our main carpal tunnel syndrome page.
[1] Va Disability Rating For Carpal Tunnel - https://www.hillandponton.com/va-disability-rating-for-carpal-tunnel/
[2] Carpal Tunnel Syndrome - https://www.orthobullets.com/hand/6018/carpal-tunnel-syndrome
[3] Hand Pain And Sensory Deficits Carpal Tunnel Syndrome Clinical Practice Guidelines - https://www.apta.org/patient-care/evidence-based-practice-resources/cpgs/hand-pain-and-sensory-deficits-carpal-tunnel-syndrome-clinical-practice-guidelines



