When you notice a new dark spot on your skin after years of sun exposure, a critical question arises: is this just a harmless age spot, or could it be something more dangerous? Understanding what do cancerous sun spots look like can literally save your life. Every year, millions of people discover skin lesions that require medical evaluation, and knowing the warning signs makes all the difference between early detection and advanced disease.
The skin tells a story of sun exposure over a lifetime. Those brown spots that appear on hands, face, and arms might seem like innocent markers of aging, but some carry a sinister secret. Cancerous sun spots don't always announce themselves with obvious symptoms, which is why learning to recognize their subtle characteristics becomes essential for everyone, especially those with significant sun exposure history.
The sun's ultraviolet radiation creates various marks on the skin, ranging from completely harmless to potentially life-threatening. Distinguishing between these requires knowledge of specific characteristics that separate innocent age spots from dangerous malignancies.
Benign sun spots, medically known as solar lentigines or age spots, are flat, brown, gray, or black spots that develop on sun-exposed areas. These harmless lesions result from years of UV exposure causing localized melanin production increases. They typically appear on the face, hands, shoulders, and arms of people over 40, though younger individuals with extensive sun exposure can develop them too.
Characteristics of harmless age spots include:
These benign spots pose no health risk and require no treatment unless desired for cosmetic reasons. However, their presence indicates significant cumulative sun damage, which increases overall skin cancer risk [1].
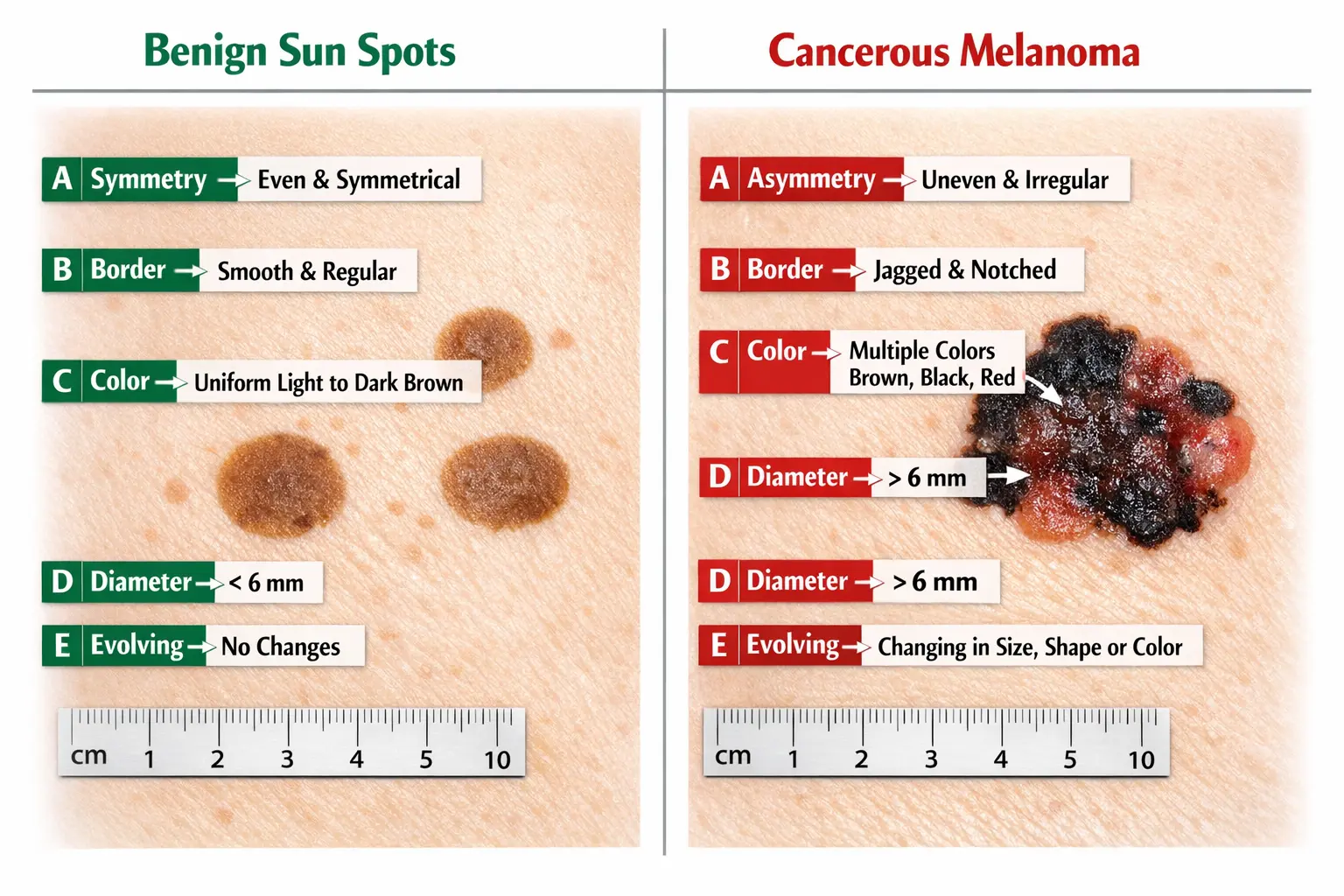
Cancerous sun spots present distinctly different characteristics that should trigger immediate medical evaluation. Understanding what do cancerous sun spots look like involves recognizing patterns that deviate from the benign features described above.
The ABCDE Rule for Identifying Dangerous Lesions:
LetterCriterionWhat to Look ForAAsymmetryOne half doesn't match the other half in shape or appearanceBBorderEdges are irregular, scalloped, notched, or poorly definedCColorMultiple colors present (brown, black, tan, red, white, blue) or uneven color distributionDDiameterLarger than 6mm (pencil eraser size), though melanomas can be smallerEEvolvingChanges in size, shape, color, elevation, or new symptoms like bleeding or itching
"The most important warning sign for melanoma is a new spot on the skin or a spot that is changing in size, shape, or color. Another important sign is a spot that looks different from all of the other spots on your skin." — American Academy of Dermatology [2]
When examining what do cancerous sun spots look like, color variation stands out as particularly concerning. A lesion displaying shades of brown mixed with black, red, white, or blue indicates abnormal cell activity at different skin depths. This multicolored appearance rarely occurs in benign spots.
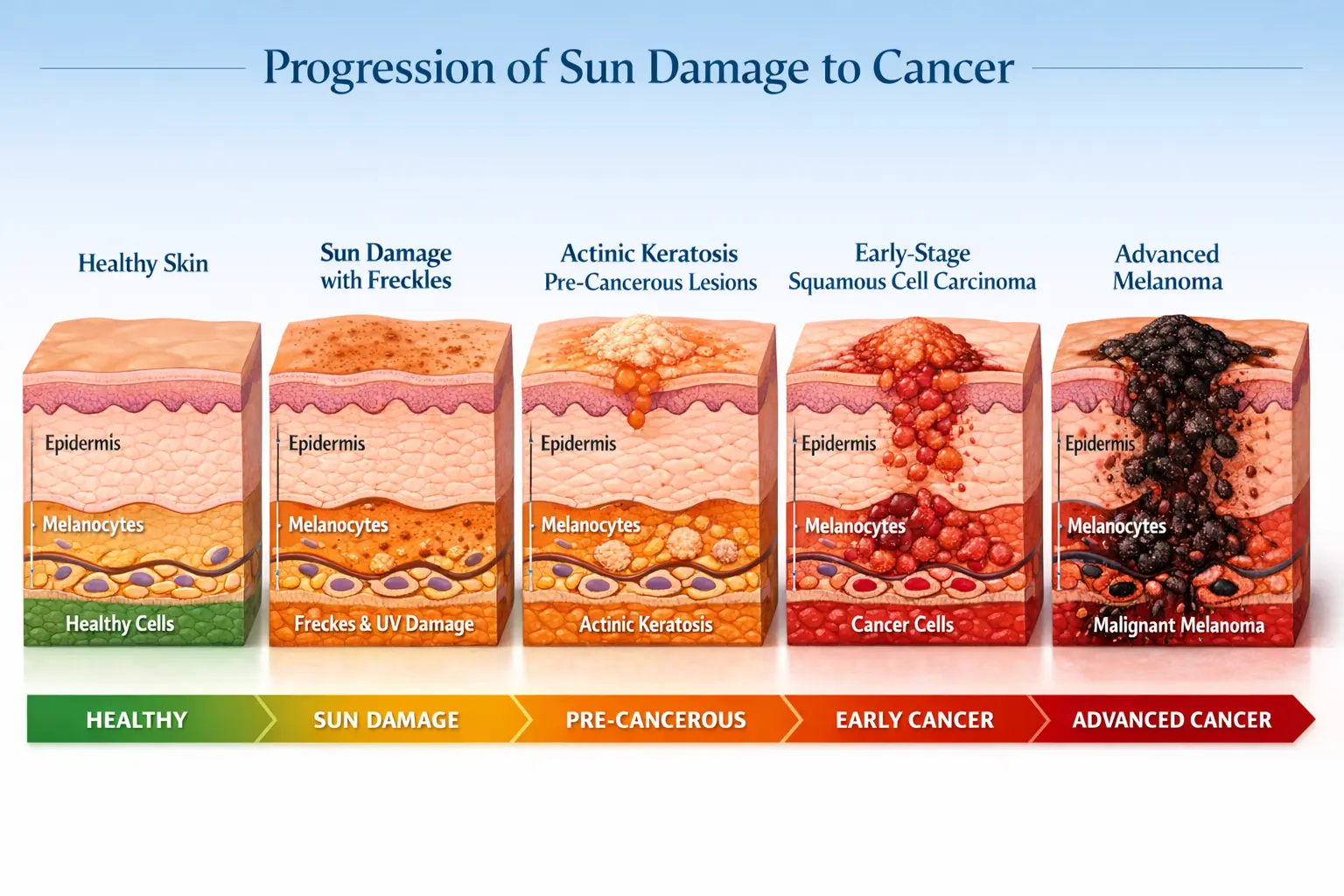
Between completely benign age spots and fully developed skin cancers lies an important middle category: pre-cancerous lesions called actinic keratoses. These rough, scaly patches deserve special attention because they can progress to squamous cell carcinoma if ignored.
Actinic keratosis characteristics:
Studies show that approximately 10% of actinic keratoses progress to squamous cell carcinoma, making early treatment important [3]. Understanding the progression from actinic keratosis to squamous cell carcinoma helps patients appreciate why dermatologists recommend treating these lesions promptly.
Sun damage can lead to three primary types of skin cancer, each with distinct appearances and risk profiles. Knowing what do cancerous sun spots look like requires understanding how each cancer type manifests on the skin.
Basal cell carcinoma represents the most common skin cancer, accounting for approximately 80% of all skin cancer diagnoses. It develops in the basal cells at the bottom of the epidermis and rarely metastasizes, but can cause significant local tissue damage if untreated [4].
What basal cell carcinoma looks like:
BCC typically appears on sun-exposed areas like the face, ears, neck, and hands. The lesions grow slowly over months or years, which sometimes leads people to dismiss them as minor skin irritations. However, early basal cell carcinoma treatment offers the best cosmetic outcomes and prevents extensive tissue destruction.
Squamous cell carcinoma is the second most common skin cancer, arising from squamous cells in the upper layers of the epidermis. While less common than BCC, SCC carries a higher risk of metastasis, particularly when located on ears, lips, or in immunocompromised patients [5].
Squamous cell carcinoma appearance:
SCC often develops in areas with chronic sun exposure or previous burns. The lesions may grow more rapidly than BCC, sometimes doubling in size within weeks or months. People frequently mistake early SCC for warts, age spots, or minor skin irritations, delaying crucial treatment.
Melanoma develops in melanocytes, the pigment-producing cells, and represents the most serious skin cancer type. Though less common than BCC or SCC, melanoma causes the majority of skin cancer deaths due to its aggressive nature and tendency to metastasize [6].
What melanoma looks like:
Melanoma can develop in an existing mole or appear as a new dark spot on previously normal skin. The different types of skin cancer each require specific treatment approaches, but melanoma demands the most urgent attention due to its potential for rapid spread.
Melanoma subtypes with unique appearances:
Understanding advanced melanoma stages emphasizes why early detection matters so critically. Stage I melanoma confined to the skin surface has excellent prognosis, while Stage IV melanoma that has spread to distant organs carries a much poorer outlook.
Regular self-examination combined with professional skin checks creates the most effective strategy for early cancer detection. Knowing what do cancerous sun spots look like provides value only when paired with systematic examination habits.
Dermatologists recommend monthly self-examinations to track changes in existing spots and identify new lesions. This simple practice takes only 10-15 minutes but can detect problems at their most treatable stages.
Step-by-step self-examination process:
What to document during self-exams:
While self-examinations provide valuable monitoring, professional evaluation by a dermatologist offers expertise and technology that home checks cannot match. Certain findings demand immediate professional assessment.
Schedule an appointment immediately if you notice:
Professional skin examinations should occur annually for most adults, or more frequently for high-risk individuals. Those with previous skin cancer, numerous moles, fair skin, significant sun exposure history, or family history of melanoma should see a dermatologist every 6 months [7].
When you visit a specialized skin cancer clinic, dermatologists employ sophisticated tools that reveal details invisible to the naked eye. These technologies dramatically improve diagnostic accuracy.
Professional diagnostic methods:
Dermoscopy – A handheld device with magnification and special lighting that reveals subsurface skin structures. Dermoscopy increases melanoma detection accuracy by approximately 30% compared to visual examination alone [8].
Digital mole mapping – Computerized full-body photography that documents all moles and spots, allowing precise comparison over time. This technology excels at detecting subtle changes that might escape notice during visual examination. Many patients benefit from visiting top mole mapping clinics for this advanced screening.
Confocal microscopy – A non-invasive imaging technique that provides near-histological resolution of skin lesions without requiring a biopsy. This emerging technology helps dermatologists evaluate suspicious lesions with unprecedented detail.
Artificial intelligence analysis – Computer algorithms trained on thousands of skin cancer images can analyze photos and flag concerning features, serving as a decision-support tool for dermatologists.
Skin biopsy – When a lesion appears suspicious, dermatologists remove a sample for microscopic examination by a pathologist. Biopsy remains the gold standard for definitive diagnosis, revealing exact cancer type and depth of invasion.
Understanding personal risk factors helps determine appropriate screening frequency and prevention strategies. Some risk factors can be modified, while others require heightened vigilance.
Certain characteristics increase skin cancer risk regardless of lifestyle choices. Recognizing these factors helps people understand their baseline risk level.
Genetic and inherent factors:
While genetic factors cannot change, lifestyle modifications significantly reduce skin cancer risk. The majority of skin cancers are preventable through sun protection measures.
Controllable risk factors:
UV exposure history – Both chronic sun exposure and severe sunburns contribute to cancer risk. Even one blistering sunburn in childhood or adolescence doubles melanoma risk [9]. Tanning bed use before age 35 increases melanoma risk by 75% [10].
Occupational sun exposure – Outdoor workers (construction, agriculture, fishing, landscaping) accumulate UV damage over decades, increasing both melanoma and non-melanoma skin cancer risk.
Geographic location – Living closer to the equator or at higher altitudes increases UV radiation exposure. However, skin cancer occurs in all geographic regions, including cloudy climates.
Prevention strategies that work:
Sunscreen application tips:
Many benign skin conditions mimic cancerous lesions, causing unnecessary anxiety. Conversely, some dangerous lesions masquerade as harmless conditions, delaying diagnosis. Understanding these look-alikes improves decision-making about when to seek professional evaluation.
Several harmless skin conditions share visual characteristics with skin cancer, leading to confusion during self-examination.
Seborrheic keratoses – These extremely common benign growths appear as brown, black, or tan warty spots that look "stuck on" the skin surface. They often develop after age 40 and can be mistaken for melanoma due to their dark color and irregular appearance. However, seborrheic keratoses have a distinctive waxy, scaly texture and well-defined borders that differ from melanoma [11].
Cherry angiomas – Bright red, dome-shaped bumps caused by dilated blood vessels. These benign growths typically appear after age 30 and increase in number with age. Their bright red color sometimes causes concern, but their uniform color and symmetrical shape distinguish them from melanoma.
Dermatofibromas – Firm, brown nodules that commonly develop on legs after minor skin trauma. These benign fibrous growths feel like a hard button under the skin and dimple inward when squeezed from the sides, unlike skin cancers which don't dimple.
Moles (nevi) – Most moles are completely benign, but distinguishing a benign mole from melanoma requires attention to the ABCDE criteria. Benign moles remain stable over time, maintain symmetry, and display uniform color.
Age spots vs. cancer spots – Understanding the difference between age spots and cancer spots prevents both unnecessary worry and dangerous delays in diagnosis. Age spots remain flat, uniform in color, and stable, while cancerous lesions show irregularity and evolution.
Some skin cancers present with subtle or atypical features that lead people to dismiss them as harmless conditions. These deceptive presentations underscore the importance of professional evaluation for any concerning lesion.
Amelanotic melanoma – This melanoma variant lacks the dark pigmentation typically associated with melanoma, appearing pink, red, or skin-colored instead. Amelanotic melanoma accounts for approximately 2-8% of melanomas and is frequently misdiagnosed as a benign lesion, wart, or scar [12].
Nodular melanoma – This aggressive melanoma subtype grows vertically rather than horizontally, appearing as a rapidly growing bump rather than a flat, spreading lesion. It may not follow traditional ABCDE criteria, making it particularly dangerous.
Superficial basal cell carcinoma – This BCC variant appears as a flat, scaly, reddish patch that resembles eczema or psoriasis. People often treat it with over-the-counter skin creams for months before realizing it requires medical attention.
Skin cancer on unusual locations – Acral melanoma appears on palms, soles, or under nails, locations people don't typically associate with sun damage. These melanomas are often diagnosed late because patients don't think to check these areas or attribute changes to injury or fungal infection.
The ugly duckling sign represents a simple but powerful concept: a lesion that looks different from all your other moles deserves professional evaluation, even if it doesn't clearly meet ABCDE criteria.
Most people's moles share similar characteristics – they tend to be roughly the same size, shape, and color. A spot that stands out as distinctly different from this pattern warrants attention, regardless of whether it displays obvious warning signs. This principle helps identify atypical presentations that might otherwise be dismissed [13].
When a suspicious lesion is identified, a systematic diagnostic process determines whether it's cancerous and, if so, what type and stage. Understanding this process reduces anxiety and helps patients know what to expect.
The diagnostic journey typically begins with a comprehensive skin examination by a dermatologist. This visit includes several components:
Medical history review – The dermatologist asks about:
Full-body skin examination – Even if you've scheduled the appointment for one specific spot, dermatologists typically examine all skin from scalp to toes. This comprehensive approach frequently reveals additional concerning lesions patients hadn't noticed.
Dermoscopic evaluation – The dermatologist uses a dermoscope to examine suspicious lesions at 10-40x magnification, revealing structures invisible to the naked eye. This non-invasive technique helps distinguish benign from malignant lesions.
Photography and documentation – Many practices photograph lesions to track changes over time and document baseline appearance.
When a lesion appears suspicious, biopsy provides definitive diagnosis. Several biopsy techniques exist, with selection depending on lesion size, location, and suspected diagnosis.
Shave biopsy – The dermatologist uses a small blade to shave off the lesion at or slightly below skin level. This technique works well for raised lesions suspected to be basal cell or squamous cell carcinoma. However, shave biopsy is generally avoided for suspected melanoma because it may not capture the full depth needed for accurate staging.
Punch biopsy – A circular blade removes a small cylinder of skin including deeper layers. Punch biopsies provide full-thickness samples useful for diagnosing various skin conditions, including suspected melanoma.
Excisional biopsy – The entire lesion is surgically removed with a margin of normal-appearing skin. This approach is preferred for suspected melanoma because it removes the entire tumor and provides complete information about depth and margins.
Incisional biopsy – Only a portion of a large lesion is removed for diagnosis. This technique is sometimes used for very large lesions when complete removal would require extensive surgery.
Biopsy procedures are typically performed under local anesthesia in the dermatologist's office. The removed tissue is sent to a pathology laboratory where a dermatopathologist examines it under a microscope to determine if cancer is present and, if so, what type and characteristics it displays.
Pathology reports contain crucial information that guides treatment decisions. Key elements include:
Diagnosis – The specific type of lesion (benign, pre-cancerous, or cancerous)
Cancer type – If malignant, whether it's basal cell carcinoma, squamous cell carcinoma, melanoma, or another skin cancer type
Breslow thickness – For melanoma, the depth of invasion measured in millimeters, which is the most important prognostic factor
Margins – Whether the biopsy removed the entire lesion with clear margins or if cancer cells extend to the edge of the specimen
Mitotic rate – The number of dividing cells, indicating how quickly the cancer is growing
Ulceration – Whether the tumor has broken through the skin surface, which affects prognosis
Other features – Including lymphovascular invasion, regression, and specific cellular characteristics
Understanding these pathology details helps patients and physicians determine appropriate next steps, from simple monitoring to aggressive treatment.
Treatment selection depends on cancer type, size, location, depth, and patient factors. Modern dermatology offers multiple effective approaches, with cure rates exceeding 95% for most non-melanoma skin cancers when caught early [14].
Surgery remains the gold standard treatment for most skin cancers, offering the highest cure rates and the ability to examine margins to ensure complete removal.
Excisional surgery – The cancerous lesion is cut out along with a margin of healthy tissue. The wound is then closed with stitches. This straightforward approach works well for most skin cancers and provides tissue for pathological examination to confirm complete removal.
Mohs micrographic surgery – This specialized technique involves removing the cancer in thin layers, examining each layer under a microscope immediately, and continuing until no cancer cells remain. Mohs surgery offers the highest cure rates (up to 99% for primary basal cell carcinoma) while preserving the maximum amount of healthy tissue [15]. This precision makes it ideal for cancers on the face, ears, hands, feet, and genitals where tissue preservation matters most.
Curettage and electrodesiccation – The cancer is scraped away with a curette (a sharp, spoon-shaped instrument), then the area is treated with an electric needle to destroy remaining cancer cells and control bleeding. This technique works well for superficial basal cell and squamous cell carcinomas but doesn't provide tissue for margin examination.
Cryosurgery – Liquid nitrogen freezes and destroys abnormal tissue. This approach treats pre-cancerous actinic keratoses and some superficial skin cancers, though it doesn't allow pathological confirmation of complete removal.
Some skin cancers and pre-cancerous lesions can be treated without surgery, particularly when they're superficial, multiple, or located in areas where surgery would be challenging.
Topical medications – Prescription creams like 5-fluorouracil (5-FU) and imiquimod stimulate the immune system or directly attack cancer cells. These treatments work for actinic keratoses and some superficial basal cell carcinomas, requiring several weeks of application.
Photodynamic therapy (PDT) – A photosensitizing agent is applied to the skin, then activated with specific wavelengths of light, destroying abnormal cells. PDT effectively treats actinic keratoses and some superficial non-melanoma skin cancers.
Radiation therapy – High-energy rays destroy cancer cells. Radiation serves as primary treatment when surgery isn't feasible (due to lesion location or patient health) or as adjuvant therapy after surgery for high-risk cancers.
Targeted therapy and immunotherapy – For advanced melanoma or squamous cell carcinoma that has spread, newer medications target specific genetic mutations (BRAF inhibitors, MEK inhibitors) or boost the immune system's ability to fight cancer (checkpoint inhibitors like pembrolizumab and nivolumab). These treatments have revolutionized outcomes for advanced skin cancer [16].
Skin cancer treatment doesn't end when the lesion is removed. Ongoing surveillance is essential because people who've had one skin cancer face significantly elevated risk of developing additional lesions.
Recommended follow-up schedule:
Follow-up visits include full-body skin examinations to detect new lesions and check the treatment site for recurrence. Patients with melanoma may also undergo lymph node examinations and, in some cases, imaging studies to monitor for metastasis.
Self-examination remains crucial between professional visits. Patients should immediately report any new or changing lesions rather than waiting for scheduled appointments.
Skin cancer can affect people of all skin tones, though presentation and risk patterns vary. Understanding these differences ensures appropriate vigilance across diverse populations.
People with fair skin (Fitzpatrick skin types I and II) face the highest skin cancer risk due to lower melanin levels providing less natural UV protection. In this population:
While less common in people with darker skin (Fitzpatrick types IV-VI), skin cancer in these populations is often diagnosed at later stages, leading to worse outcomes. Important considerations include:
Different presentation patterns – Melanoma in darker skin often appears on non-sun-exposed areas like palms, soles, mucous membranes, and under nails. These acral and mucosal melanomas don't follow typical sun-damage patterns [17].
Color variations – Skin cancers in darker skin may appear as dark brown, black, or even amelanotic (lacking color), making them harder to distinguish from normal skin variations.
Lower awareness – Both patients and healthcare providers may have lower suspicion for skin cancer in darker-skinned individuals, contributing to delayed diagnosis.
Subungual melanoma – Melanoma under the nail (often appearing as a dark streak in the nail) is more common in people with darker skin and is frequently misdiagnosed as a bruise or fungal infection.
"Skin cancer can affect anyone, regardless of skin color. While it's less common in people of color, when it does occur, it's often diagnosed at a later stage when it's more difficult to treat." — Skin Cancer Foundation [18]
All individuals, regardless of skin tone, should perform monthly self-examinations and seek professional evaluation for any new, changing, or unusual skin lesions. The comprehensive guide to skin lesions helps people recognize various skin changes that warrant attention.

A skin cancer diagnosis or identification of significant risk factors requires lifelong vigilance and lifestyle adjustments. These strategies reduce future cancer risk and ensure early detection if new lesions develop.
After skin cancer diagnosis or identification of pre-cancerous lesions, sun protection becomes non-negotiable. Consistent UV protection significantly reduces the risk of additional skin cancers.
Daily sun protection habits:
Vitamin D considerations – Some people worry that sun avoidance will cause vitamin D deficiency. However, vitamin D can be obtained through diet (fatty fish, fortified foods) and supplements without UV exposure. The skin cancer risk from unprotected sun exposure far outweighs any vitamin D benefits.
Early detection remains the most powerful tool for managing skin cancer risk. Establishing systematic surveillance habits ensures problems are caught at their most treatable stages.
Monthly self-examination checklist:
✅ Examine skin in a well-lit room with full-length and hand mirrors
✅ Check all body areas, including scalp, ears, between toes, soles, and genital area
✅ Document any new spots or changes in existing lesions
✅ Take photos of concerning areas to track changes over time
✅ Note any spots that itch, bleed, or feel different
✅ Use the ABCDE criteria to evaluate suspicious lesions
✅ Schedule a dermatology appointment if anything concerns you
Professional screening schedule:
A skin cancer diagnosis, even of a highly curable type, can cause significant anxiety. Fear of recurrence, worry about appearance after treatment, and hypervigilance about new spots are common reactions.
Coping strategies:
Remember that most skin cancers are highly treatable, especially when caught early. The vast majority of people diagnosed with skin cancer are cured and live normal lifespans.
While some skin cancers develop relatively quickly, most evolve over months or years. Melanoma can appear as a new spot or develop in an existing mole, sometimes growing noticeably over weeks to months. Basal cell and squamous cell carcinomas typically develop more slowly. Any new spot that appears and continues to grow, change, or look different from your other moles deserves professional evaluation.
No. The majority of dark spots on sun-exposed skin are benign age spots (solar lentigines), freckles, or moles. However, some dark spots are cancerous, which is why evaluation using ABCDE criteria is important. When in doubt, have a dermatologist examine any concerning spot.
Most skin cancers don't cause pain in early stages. However, some people experience tenderness, itching, or burning sensations. Squamous cell carcinoma and advanced basal cell carcinoma may become painful as they grow. Pain or tenderness in a skin lesion warrants medical evaluation but isn't required for a cancer diagnosis.
Schedule an appointment within 2-4 weeks for any spot that meets ABCDE criteria, bleeds without trauma, doesn't heal, or otherwise concerns you. While most skin cancers grow slowly enough that a few weeks won't significantly impact outcomes, don't delay for months. If a lesion is rapidly growing, bleeding profusely, or causing severe symptoms, seek evaluation sooner.
Sunscreen significantly reduces skin cancer risk but doesn't provide 100% protection. Studies show regular sunscreen use reduces melanoma risk by approximately 50% and squamous cell carcinoma risk by about 40% [19]. Sunscreen should be part of a comprehensive sun protection strategy that includes protective clothing, shade-seeking, and avoiding peak UV hours.
While most skin cancers develop on sun-exposed skin, melanoma can appear anywhere on the body, including areas that rarely see sun (soles, palms, genital area, under nails). This is why full-body skin examinations are important, not just checking sun-exposed areas.
Understanding what do cancerous sun spots look like empowers you to take control of your skin health. The ability to distinguish between benign age spots and dangerous lesions can literally save your life, given that early-stage skin cancer has cure rates exceeding 95%.
The key warning signs bear repeating: asymmetry, irregular borders, multiple or uneven colors, diameter larger than a pencil eraser, and evolution over time. Any spot displaying these characteristics deserves professional evaluation, as does any lesion that bleeds, doesn't heal, or looks different from your other moles.
Your action plan starting today:
Remember that skin cancer is one of the most preventable and, when caught early, most treatable cancers. The few minutes spent on monthly self-examinations and daily sun protection can prevent years of treatment and worry. Your skin tells the story of your life's sun exposure – learn to read that story carefully, and don't hesitate to seek expert interpretation when something doesn't look right.
The difference between a harmless age spot and a dangerous melanoma may seem subtle, but with the knowledge you've gained from this guide, you're now equipped to recognize warning signs and take appropriate action. Your vigilance today could save your life tomorrow.
[1] American Academy of Dermatology. (2026). Age spots and your skin. Retrieved from AAD.org
[2] American Academy of Dermatology. (2026). Melanoma warning signs and images. Retrieved from AAD.org
[3] Werner, R. N., et al. (2023). Evidence- and consensus-based (S3) Guidelines for the Treatment of Actinic Keratosis. Journal of the European Academy of Dermatology and Venereology, 37(8), 1483-1504.
[4] American Cancer Society. (2026). Basal and Squamous Cell Skin Cancer Statistics. Retrieved from cancer.org
[5] Karia, P. S., et al. (2013). Cutaneous squamous cell carcinoma: Estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. Journal of the American Academy of Dermatology, 68(6), 957-966.
[6] Siegel, R. L., et al. (2026). Cancer statistics, 2026. CA: A Cancer Journal for Clinicians, 76(1), 12-49.
[7] Skin Cancer Foundation. (2026). Skin Cancer Screening Guidelines. Retrieved from skincancer.org
[8] Vestergaard, M. E., et al. (2008). Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: A meta-analysis of studies performed in a clinical setting. British Journal of Dermatology, 159(3), 669-676.
[9] Dennis, L. K., et al. (2008). Sunburns and risk of cutaneous melanoma: Does age matter? Annals of Epidemiology, 18(8), 614-621.
[10] Boniol, M., et al. (2012). Cutaneous melanoma attributable to sunbed use: Systematic review and meta-analysis. BMJ, 345, e4757.
[11] Jackson, J. M., et al. (2015). Seborrheic keratosis: A review. Journal of Drugs in Dermatology, 14(10), 1119-1123.
[12] Pizzichetta, M. A., et al. (2004). Amelanotic/hypomelanotic melanoma: Clinical and dermoscopic features. British Journal of Dermatology, 150(6), 1117-1124.
[13] Grob, J. J., & Bonerandi, J. J. (1998). The 'ugly duckling' sign: Identification of the common characteristics of nevi in an individual as a basis for melanoma screening. Archives of Dermatology, 134(1), 103-104.
[14] Rogers, H. W., et al. (2015). Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the US population, 2012. JAMA Dermatology, 151(10), 1081-1086.
[15] Rowe, D. E., et al. (1989). Mohs surgery is the treatment of choice for recurrent (previously treated) basal cell carcinoma. Journal of Dermatologic Surgery and Oncology, 15(4), 424-431.
[16] Larkin, J., et al. (2019). Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. New England Journal of Medicine, 381(16), 1535-1546.
[17] Bradford, P. T., et al. (2009). Acral lentiginous melanoma: Incidence and survival patterns in the United States, 1986-2005. Archives of Dermatology, 145(4), 427-434.
[18] Skin Cancer Foundation. (2026). Skin Cancer in People of Color. Retrieved from skincancer.org
[19] Green, A. C., et al. (2011). Daily sunscreen application and betacarotene supplementation in prevention of basal-cell and squamous-cell carcinomas of the skin: A randomised controlled trial. The Lancet, 354(9180), 723-729.



