Tinea Cruris, Tinea Versicolor, Tinea Corporis Explained: A Comprehensive Guide for 2025
Skin conditions can be perplexing, often presenting with similar symptoms yet stemming from vastly different causes. Among the most common dermatological challenges are fungal infections, which can manifest in various forms across the body. Understanding these conditions is crucial for effective treatment and prevention. This comprehensive guide for 2025 delves into three prevalent superficial fungal infections: tinea cruris, tinea versicolor, and tinea corporis explained, offering insights into their causes, symptoms, diagnosis, and treatment options. Whether you're experiencing an itchy rash or simply seeking to expand your knowledge of skin health, this article provides authoritative, easy-to-understand information to help navigate these common fungal concerns.
Key Takeaways
Tinea Infections are Fungal: Tinea cruris, tinea versicolor, and tinea corporis are all caused by fungi, either dermatophytes or yeasts, thriving in specific environments on the skin.
Distinct Locations & Appearances: Each condition has a typical presentation and location: tinea corporis (ringworm) often appears as ring-shaped lesions on the body, tinea cruris (jock itch) affects the groin, and tinea versicolor causes discolored patches on the chest and back.
Contagious Nature: Tinea corporis and tinea cruris are highly contagious and can spread through direct contact or shared items, while tinea versicolor is caused by an overgrowth of yeast naturally present on the skin.
Effective Treatment Available: Most tinea infections respond well to topical antifungal medications, though persistent or widespread cases may require oral antifungals.
Prevention is Key: Maintaining good hygiene, wearing breathable clothing, and avoiding prolonged moisture are essential preventive measures against these fungal infections.
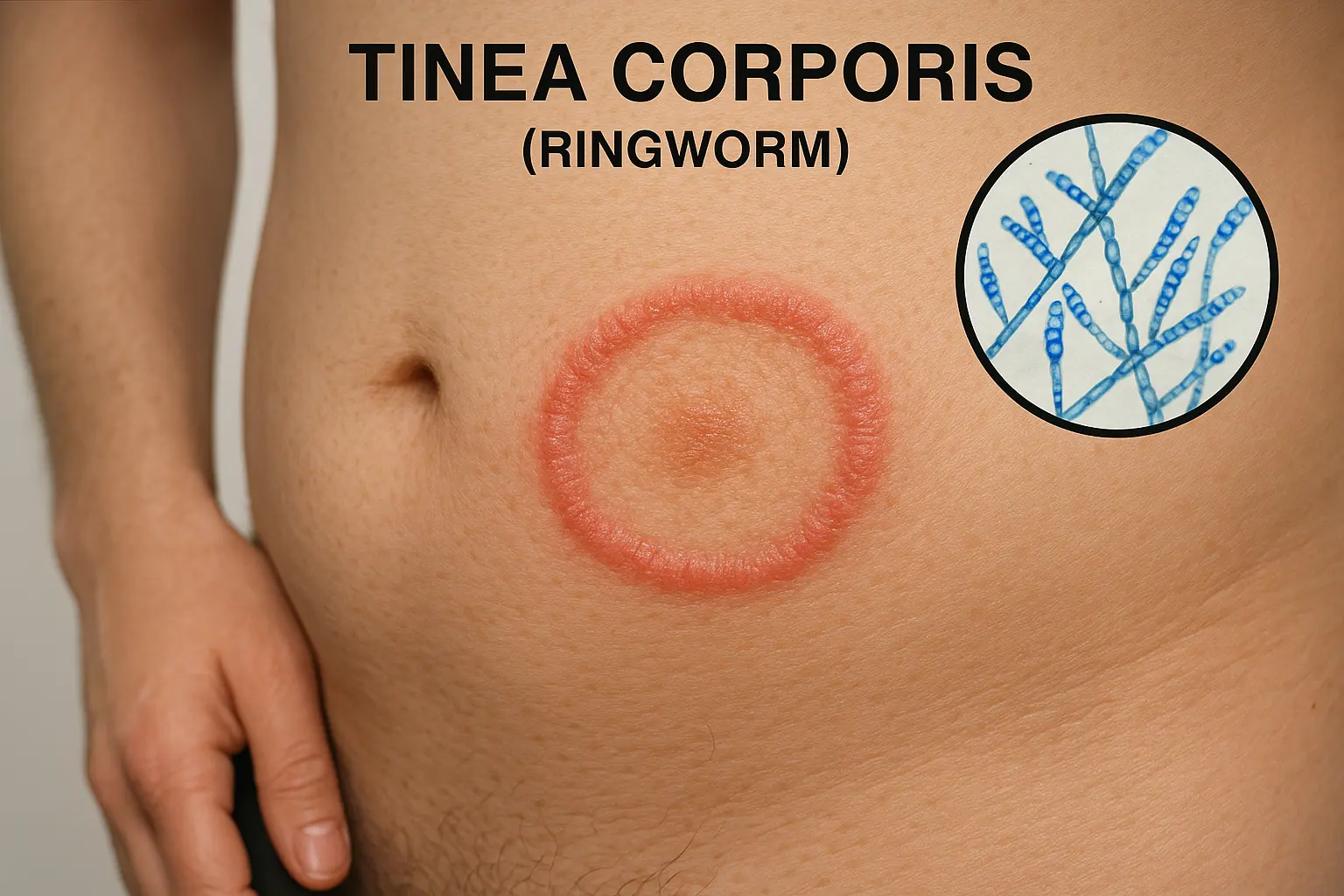
Tinea corporis, commonly known as ringworm, is a superficial fungal infection that can affect various parts of the body, excluding the scalp, groin, hands, and feet (which have their own specific tinea designations). Despite its misleading name, ringworm has nothing to do with worms; rather, it's caused by dermatophytes, a group of fungi that thrive on keratin, a protein found in skin, hair, and nails. These fungi belong primarily to the genera Trichophyton, Epidermophyton, and Microsporum [4].
What Causes Tinea Corporis?
The primary culprits behind tinea corporis are dermatophytic fungi. These microscopic organisms are highly adaptable and seek out warm, moist environments to grow and spread. Several factors contribute to their proliferation:
Warm and Humid Climates: Fungi flourish in environments with high heat and humidity, making these conditions ideal for tinea corporis development.
Sweating: Excessive sweating creates a damp environment on the skin, providing a breeding ground for fungi.
Skin-to-Skin Contact: Direct contact with an infected person is a common mode of transmission. This can occur through activities like wrestling or close living quarters.
Contact with Contaminated Objects: Sharing personal items such as towels, clothing, sports equipment, or bedding with an infected individual can lead to transmission [1].
Infected Pets: Animals, particularly cats and dogs, can carry dermatophytes and transmit the infection to humans. This is especially common in children.
Weakened Immune System: Individuals with compromised immune systems are more susceptible to fungal infections and may experience more severe or widespread cases.
Symptoms and Appearance of Tinea Corporis
The hallmark of tinea corporis is its characteristic ring-shaped rash, which is where the "ringworm" moniker originates. Understanding these symptoms is key to recognizing the infection early:
Annular (Ring-Shaped) Lesions: Tinea corporis typically presents as circular or oval, reddish, scaly patches on the skin. The most distinctive feature is the raised, active border that expands outwards, while the center of the lesion often appears clearer or less inflamed [4].
Itchiness (Pruritus): The affected areas are almost always intensely itchy, which can lead to scratching and further skin irritation or secondary bacterial infections.
Scaling and Redness: The skin within and around the ring may be scaly, flaky, and red (erythematous).
Location: While it can appear anywhere on the body, common sites include the arms, legs, trunk, and face.
Expanding Lesions: The lesions tend to grow centrifugally, meaning they expand from the outer edges inward. This outward spread contributes to the characteristic ring appearance [4].
Confluent or Widespread Cases: In individuals with weakened immune systems, the lesions may not have the typical ring shape and can become confluent (merging together) or spread over larger areas of the body [4].
Table: Key Features of Tinea Corporis
FeatureDescriptionAppearanceAnnular (ring-shaped) scaly plaques, often with central clearing and a raised, red border.Primary CauseDermatophyte fungi (Trichophyton, Epidermophysum, Microsporum).SymptomsIntense itching (pruritus), redness, scaling.TransmissionDirect contact (person-to-person, animal-to-person), contact with contaminated objects (fomites) [1].Common SitesArms, legs, trunk, face.
Diagnosis and Treatment of Tinea Corporis
Diagnosing tinea corporis typically involves a physical examination by a healthcare professional, who will assess the characteristic appearance of the rash. Sometimes, a skin scraping (KOH prep) is performed to confirm the presence of fungal elements under a microscope. This involves gently scraping a small sample of skin from the affected area and examining it with a potassium hydroxide (KOH) solution, which dissolves skin cells but leaves fungal elements intact, making them visible.
Treatment for tinea corporis is generally straightforward and highly effective.
Topical Antifungal Creams: For most cases, over-the-counter or prescription-strength topical antifungal creams are the first line of treatment. These include active ingredients such as terbinafine (Lamisil), butenafine (Lotrimin Ultra), clotrimazole, miconazole, and ketoconazole [5]. These creams should be applied to the affected area and a small margin of healthy skin around it, usually twice daily for 2-4 weeks, even if the rash appears to clear sooner. Consistent application is crucial to prevent recurrence.
Oral Antifungal Medications: In more severe, widespread, or persistent cases, or in individuals with compromised immune systems, oral antifungal medications may be prescribed. Common oral options include terbinafine, itraconazole, and fluconazole. These medications work systemically to eliminate the fungus from within the body but carry a higher risk of side effects and require monitoring by a doctor.
Hygiene and Prevention:
Keep the affected area clean and dry.
Avoid sharing personal items like towels, clothing, and combs.
Wash clothes, bedding, and towels regularly in hot water.
Wear loose-fitting, breathable clothing, especially in warm weather.
If a pet is suspected to be the source, have it examined and treated by a veterinarian.
Avoid scratching, as this can spread the infection or lead to secondary bacterial infections.
"Tinea corporis, tinea cruris, and tinea pedis generally respond to inexpensive topical antifungal agents such as terbinafine cream or butenafine cream." — Expert Consensus [5]
Early and consistent treatment is vital for resolving tinea corporis and preventing its spread. If the rash does not improve with over-the-counter treatments or if it worsens, consulting a healthcare professional is recommended. For more information on general skin lesions and when to seek professional medical advice, you can explore resources like 25 Types of Skin Lesions Explained.
Delving into Tinea Cruris: "Jock Itch" Explained
Tinea cruris, widely known as jock itch, is another common superficial fungal infection that specifically targets the groin area. While the name suggests an affliction primarily for athletes, it can affect anyone, though it is indeed more prevalent in men than women [1]. This condition is characterized by an intensely itchy rash in the inner thighs, groin, and sometimes the buttocks. Understanding tinea cruris, tinea versicolor, tinea corporis explained in full detail means recognizing the unique features of each.
Causes and Risk Factors for Tinea Cruris
Like tinea corporis, tinea cruris is caused by dermatophyte fungi that thrive in specific conditions. The warm, dark, and moist environment of the groin makes it an ideal breeding ground for these organisms.
Specific Fungi: The most common culprits include Trichophyton rubrum, Trichophyton mentagrophytes, and Epidermophyton floccosum. Candida albicans, a yeast, can also cause similar symptoms, often referred to as candidal intertrigo [1].
Warm, Dark, and Moist Environments: The groin area naturally provides these conditions, especially during physical activity or in humid climates.
Excessive Sweating: Perspiration creates moisture, which contributes to fungal growth. Tight-fitting clothing traps this moisture, exacerbating the problem.
Obesity: Skin folds in obese individuals can trap moisture and create friction, increasing the risk of infection.
Sharing Personal Items: Towels, clothing, and unwashed sports equipment can transmit the fungi from person to person.
Compromised Immune System: Individuals with conditions like diabetes or a weakened immune system are more susceptible to fungal infections.
Associated Fungal Infections: Often, tinea cruris can occur alongside tinea pedis (athlete's foot), as the fungi can be transferred from the feet to the groin, for instance, by pulling up underwear.
Identifying Symptoms of Tinea Cruris
The symptoms of tinea cruris are usually quite distinctive, making it relatively easy to identify.
Red, Scaly Rash: The rash typically appears as a red, brownish-red, or reddish-brown patch with a well-defined, often raised and scaly border. The color can vary based on skin tone.
Intense Itching (Pruritus): This is one of the most prominent symptoms, leading to significant discomfort and a strong urge to scratch.
Location: The rash primarily affects the groin area, inner thighs, and sometimes extends to the buttocks or perineum. Crucially, it usually spares the penile shaft and scrotum, differentiating it from other conditions like candidal infections which might involve these areas [2].
Burning Sensation: A burning or stinging sensation is common, especially with increased moisture or friction.
Peeling and Flaking Skin: The affected skin may peel, crack, or flake, particularly at the edges of the rash.
Annular or Crescent-Shaped: The rash can be somewhat ring-shaped, similar to tinea corporis, but often appears as a crescent or half-moon shape in the groin folds.
Quick Comparison: Tinea Cruris vs. Other Conditions
FeatureTinea CrurisIntertrigo (non-fungal)Candidal Intertrigo (yeast)CauseDermatophyte fungi [1].Skin-on-skin friction, moisture.Candida albicans yeast.AppearanceRed, scaly, distinct, often raised border; usually spares penis/scrotum [2].Red, raw, sometimes moist; less distinct border.Red, moist, satellite lesions (small spots outside main rash); involves folds.Itch/BurnIntense itching, burning.Burning, soreness.Intense itching, burning.Treatment TypeAntifungal creams (e.g., terbinafine) [5].Barrier creams, moisture control, friction reduction.Antifungal creams (e.g., nystatin) or oral antifungals.
Diagnosis and Effective Treatment of Tinea Cruris
Diagnosis of tinea cruris is usually made clinically based on the characteristic appearance of the rash. A healthcare provider might also perform a KOH preparation of a skin scraping to confirm the fungal infection.
Treatment for jock itch is highly effective when approached correctly:
Topical Antifungal Creams: The cornerstone of treatment is topical antifungal creams, similar to those used for tinea corporis. Products containing terbinafine, butenafine, clotrimazole, miconazole, or ketoconazole are highly effective [5]. These should be applied thinly to the affected area and the surrounding skin for at least 2-4 weeks, even after symptoms resolve, to eradicate the fungus completely.
Oral Antifungal Medications: For severe, widespread, or recurrent cases, or in individuals who don't respond to topical treatments, oral antifungal medications like terbinafine or fluconazole may be necessary. These require a prescription and medical supervision due to potential side effects.
Hygiene Practices for Relief and Prevention:
Keep Dry: After showering or sweating, thoroughly dry the groin area. Consider using an antifungal powder or cornstarch to absorb moisture.
Loose Clothing: Wear loose-fitting, breathable cotton underwear and clothing to reduce moisture and friction. Avoid synthetic materials that trap heat and sweat.
Shower Regularly: Especially after exercise or heavy sweating.
Avoid Sharing: Do not share towels, clothing, or other personal items.
Treat Concurrent Infections: If you have athlete's foot, treat it simultaneously to prevent reinfection of the groin.
Change Clothes: Change underwear and sweaty clothes daily, or more frequently if sweating heavily.
If symptoms persist or worsen despite appropriate self-care and over-the-counter treatments, or if the rash appears unusually severe, consulting a medical professional is advised. For persistent skin issues that don't seem to be fungal, it's always wise to get a professional opinion, as certain conditions can mimic fungal infections. You can find more information about distinguishing various skin concerns at The Minor Surgery Center.
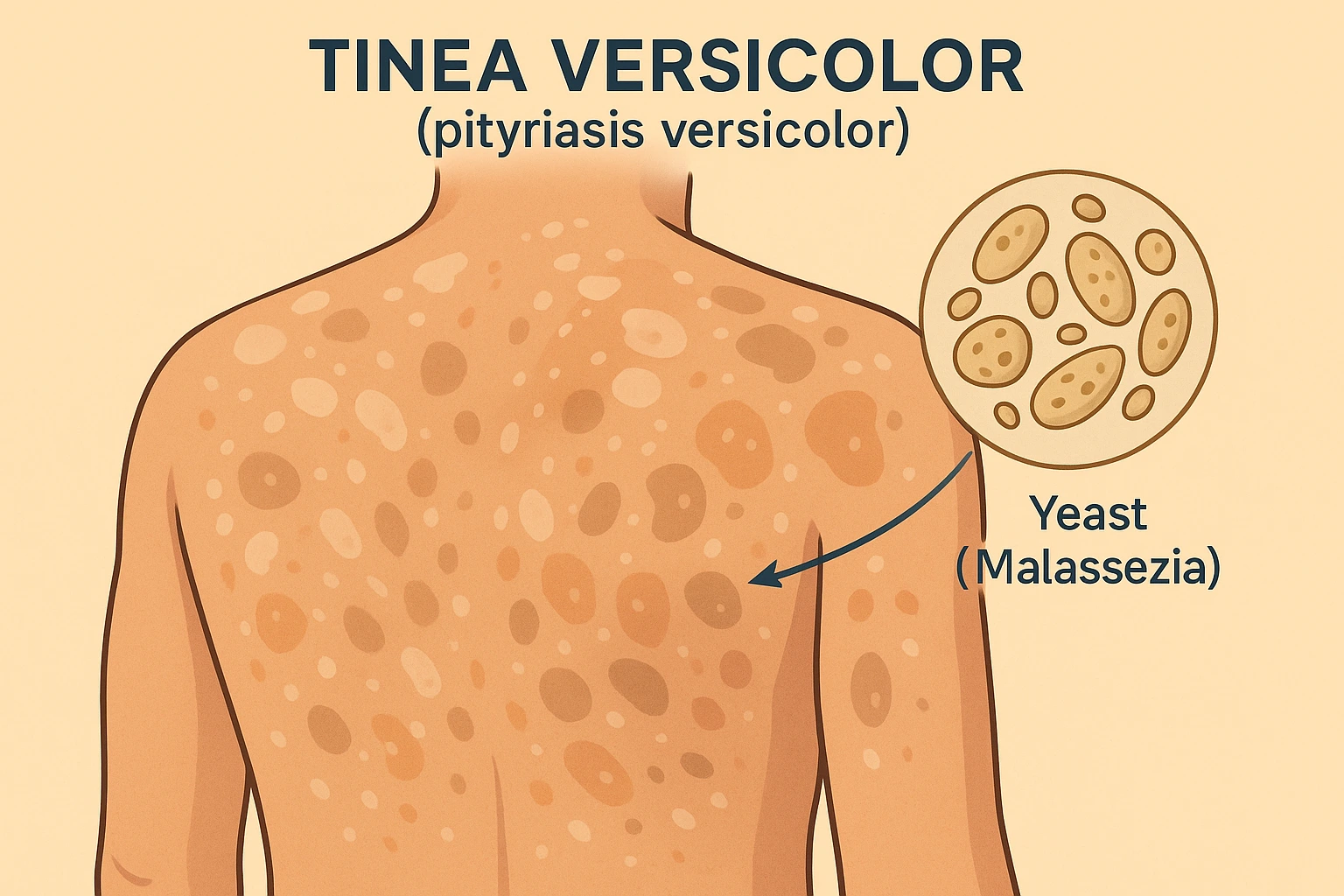
Tinea versicolor, more accurately termed pityriasis versicolor, stands apart from tinea corporis and tinea cruris in its causative agent and typical presentation. While the other tineas are caused by dermatophyte fungi, tinea versicolor is a chronic, superficial fungal infection caused by yeasts of the genus Malassezia, specifically Pityrosporum ovale [1][5]. This yeast is a normal inhabitant of human skin but can overgrow under certain conditions, leading to the characteristic skin discoloration.
What Triggers Tinea Versicolor?
Malassezia yeasts are lipophilic, meaning they thrive in oily environments. This explains why tinea versicolor often appears in areas with a high density of sebaceous (oil) glands.
Yeast Overgrowth: The primary cause is an overgrowth of Malassezia yeast, which is naturally present on the skin. It's not typically spread person-to-person in the same way as dermatophyte infections.
Warm and Humid Climates: This is a significant contributing factor. The yeast flourishes in hot, humid weather, which is why the condition is common in tropical and subtropical regions and often recurs during summer months [1].
Excessive Sweating: Increased sweating creates a moist and warm environment that encourages yeast proliferation.
Oily Skin: Individuals with naturally oily skin are more prone to tinea versicolor due to the yeast's lipophilic nature.
Hormonal Changes: Puberty, pregnancy, and other hormonal fluctuations can sometimes trigger or worsen the condition.
Weakened Immune System: Like other fungal infections, a suppressed immune system can make individuals more susceptible.
Recognizing the Symptoms of Tinea Versicolor
Tinea versicolor is characterized by patches of discolored skin, which can vary in appearance. The term "versicolor" highlights this variability.
Discolored Patches: The most noticeable symptom is the appearance of small, round to oval patches of skin that are either lighter (hypopigmented) or darker (hyperpigmented) than the surrounding skin.
Hypopigmentation: After sun exposure, the affected areas fail to tan, making them appear significantly lighter than the tanned surrounding skin. This is due to a chemical produced by the Malassezia yeast that interferes with melanin production [2].
Hyperpigmentation: The patches can also appear reddish-brown, pink, or light brown, especially on untanned skin.
Scaly Appearance: The patches often have a fine, powdery, or flaky scale, which may become more apparent when the skin is scraped or stretched.
Location: Common sites include the chest, upper back, neck, and sometimes the arms and abdomen [2]. These are areas rich in sebaceous glands.
Mild Itching: While itching can occur, it is generally mild compared to tinea corporis or tinea cruris. Some individuals may experience no itching at all.
Recurrence: Tinea versicolor is known for its tendency to recur, especially in warm or humid weather, even after successful treatment [1].
Pull Quote: "Tinea versicolor, more accurately called pityriasis versicolor, is a chronic superficial fungal infection caused by yeasts of the genus Malassezia, specifically Pityrosporum ovale." [1][5]
Diagnosis and Management of Tinea Versicolor
Diagnosis of tinea versicolor is often made clinically based on the characteristic appearance and distribution of the lesions. A dermatologist may use a Wood's lamp (UV light) examination, under which the affected areas may fluoresce a yellowish-green color. A KOH preparation of skin scrapings can also confirm the presence of yeast cells and characteristic short hyphae (often described as "spaghetti and meatballs" appearance).
Treatment for tinea versicolor focuses on eliminating the yeast overgrowth:
Topical Antifungal Shampoos/Creams:
Selenium Sulfide Shampoo: This is a common and effective over-the-counter treatment. It's typically applied to the affected areas for 10-15 minutes before rinsing, daily for a week, and then once a week for maintenance.
Ketoconazole Shampoo/Cream: Prescription-strength ketoconazole cream or shampoo can also be very effective. The shampoo is used similarly to selenium sulfide.
Other Azole Creams: Clotrimazole or miconazole creams can be used for smaller, localized patches.
Zinc Pyrithione: Shampoos containing zinc pyrithione can also be helpful.
Oral Antifungal Medications: For extensive, stubborn, or frequently recurring cases, oral antifungal medications such as fluconazole or itraconazole may be prescribed. These are typically taken as a single dose or a short course but carry potential side effects and require medical supervision.
Preventive Measures and Maintenance:
Antifungal Washes: Regular use of antifungal shampoos (selenium sulfide or ketoconazole) as a body wash once or twice a week, especially in warm months, can help prevent recurrence.
Loose Clothing: Wear breathable fabrics to minimize sweating and moisture buildup.
Sun Protection: While sun exposure highlights the discolored patches, it doesn't cause the infection. However, sun protection is good practice for overall skin health.
Patience with Pigmentation: It's important to note that even after the yeast is successfully treated, the skin discoloration (especially hypopigmentation) may take several weeks or months to return to normal, as the skin needs time to repigment. Sun exposure after treatment can help even out skin tone.
If you suspect you have tinea versicolor or if your skin condition is not improving with over-the-counter treatments, consult a healthcare provider. They can confirm the diagnosis and recommend the most appropriate course of action. Sometimes, what looks like a fungal infection might be something else entirely, like a cyst or even a skin cancer, highlighting the importance of professional evaluation. Learn more about When It's Not a Fungus (Cyst/Skin Cancer).
Distinguishing Tinea Cruris, Tinea Versicolor, and Tinea Corporis Explained
While all three conditions fall under the umbrella of fungal or yeast infections, it's important to understand their key differences to ensure proper identification and treatment. Here's a comparative overview of tinea cruris, tinea versicolor, and tinea corporis explained in an easy-to-understand format:
Table: Comparative Analysis of Tinea Conditions (2025)
FeatureTinea Corporis (Ringworm)Tinea Cruris (Jock Itch)Tinea Versicolor (Pityriasis Versicolor)Causative AgentDermatophyte fungi (Trichophyton, Epidermophyton, Microsporum) [4].Dermatophyte fungi (Trichophyton rubrum, E. floccosum) or Candida albicans [1].Yeasts of the genus Malassezia (Pityrosporum ovale) [1][5].Typical LocationArms, legs, trunk, face (anywhere on the body except scalp, groin, hands, feet) [4].Groin, inner thighs, buttocks; usually spares penis/scrotum [2].Chest, upper back, neck, sometimes arms and abdomen [2].AppearanceAnnular (ring-shaped) scaly plaques with central clearing and raised, red border [4].Red, scaly, often confluent rash with well-defined, raised border; crescent-shaped [2].Patches of discolored skin (hypo- or hyperpigmented), fine powdery scale [2].ItchinessOften intensely pruritic (itchy) [4].Intense pruritus (itching) [2].Mild itching or no itching [2].Spread/ContagionHighly contagious; spread via person-to-person, animal-to-person, fomites [1].Highly contagious; spread via person-to-person, shared items, tinea pedis [1].Not typically contagious in the same way; caused by overgrowth of normal skin flora [1].Predisposing FactorsWarm/humid climates, sweating, direct contact, immunocompromise.Warm/moist environments, sweating, tight clothing, obesity, associated tinea pedis [1].Warm/humid climates, oily skin, sweating, hormonal changes, immunocompromise [1].Common TreatmentTopical antifungals (terbinafine, butenafine); oral antifungals for severe cases [5].Topical antifungals (terbinafine, butenafine); oral antifungals for severe cases [5].Topical antifungal shampoos/creams (selenium sulfide, ketoconazole); oral for severe [5].RecurrencePossible if treatment is incomplete or re-exposure occurs.Possible if risk factors persist or reinfection from other tinea sites.Common, especially in warm/humid weather; requires maintenance treatment [1].
This comparison makes it clear that while all three are superficial skin infections, their specific characteristics guide proper diagnosis and treatment strategies. For instance, the ring-like shape of tinea corporis is distinct from the groin-confined rash of tinea cruris, and both differ significantly from the patchy discoloration of tinea versicolor.
When to Seek Professional Medical Advice
While many cases of tinea infections can be managed with over-the-counter treatments and good hygiene, there are situations where professional medical attention is crucial:
No Improvement or Worsening: If the rash does not improve after 2-4 weeks of consistent over-the-counter antifungal treatment, or if it appears to be spreading or worsening.
Severe Symptoms: If you experience extreme pain, extensive blistering, weeping, or signs of a secondary bacterial infection (e.g., pus, increased redness, fever).
Widespread Infection: If the infection covers a large area of the body or affects multiple sites.
Scalp or Nail Involvement: Tinea capitis (scalp ringworm) and tinea unguium (nail fungus) require specific oral antifungal treatments and often cannot be resolved with topical creams alone.
Compromised Immune System: Individuals with diabetes, HIV/AIDS, or those on immunosuppressive medications should seek medical advice promptly for any skin infection.
Uncertain Diagnosis: If you are unsure whether your rash is indeed a fungal infection, or if it has unusual characteristics. Many other skin conditions can mimic tinea, including eczema, psoriasis, or even more serious issues like skin cancer. For example, identifying the nature of a lesion is critical, and resources like Barrie Mole Cyst Removal can help understand surgical options for non-fungal growths.
A healthcare provider can accurately diagnose the condition through a physical examination and, if necessary, laboratory tests like a KOH preparation or fungal culture. This ensures you receive the most effective treatment and rules out other potential underlying conditions. The Minor Surgery Center, for instance, offers expertise in diagnosing and treating various skin conditions, linking directly to a range of services on https://www.theminorsurgerycenter.com.
The Importance of Fungal Hub and Differential Diagnosis
Understanding tinea cruris, tinea versicolor, tinea corporis explained is crucial, but it's equally important to know that not every skin lesion is a fungus. The skin is a complex organ, susceptible to a myriad of conditions that can often look similar. This section emphasizes the critical role of differential diagnosis and introduces the concept of a "fungal hub" – a centralized understanding of fungal infections contrasted with other dermatological issues.
The "Fungal Hub" Concept
Think of this article as a key component of a "fungal hub" – a comprehensive resource dedicated to educating individuals about common fungal skin infections. This hub consolidates information on various tinea conditions (corporis, cruris, versicolor, pedis, capitis, manuum, unguium) and other fungal or yeast-related dermatoses. The goal is to provide a clear, reliable source for identifying, treating, and preventing these prevalent conditions.
A robust fungal hub empowers individuals to:
Self-Assess Initial Symptoms: Understand typical presentations to determine if a professional consultation is warranted.
Practice Effective Self-Care: Implement appropriate hygiene and over-the-counter treatments for mild cases.
Know When to Seek Help: Recognize red flags that indicate a need for medical intervention.
Prevent Recurrence: Learn best practices to avoid future infections.
This article, "tinea cruris , tinea versicolor, tinea corporis explained," serves as a cornerstone of such a hub, offering detailed insights into three common manifestations of fungal skin infections.
When It's Not a Fungus: Differential Diagnosis
One of the most vital aspects of skin health is recognizing that not every rash or bump is a fungal infection. Many conditions can mimic tinea, leading to misdiagnosis and ineffective treatment if not properly identified. This is where differential diagnosis becomes critical.
Key Conditions That Can Mimic Tinea:
Eczema (Dermatitis):
Appearance: Red, itchy, inflamed patches, often with dry, scaly skin. Can sometimes be ring-like.
Distinction from Tinea: Eczema often has less defined borders, is typically very itchy, and may appear in skin folds or on flexural surfaces. It doesn't show fungal elements on KOH prep.
Psoriasis:
Appearance: Thick, red patches covered with silvery scales, well-defined borders.
Distinction from Tinea: Psoriasis lesions are usually symmetrically distributed, commonly found on elbows, knees, and scalp. The scales are typically thicker and more adherent than tinea.
Contact Dermatitis:
Appearance: Red, itchy rash, often with blistering or oozing, occurring after contact with an allergen or irritant.
Distinction from Tinea: The rash often corresponds to the area of contact with the offending substance and resolves once exposure ceases.
Seborrheic Dermatitis:
Appearance: Red, scaly, greasy patches, particularly on the scalp, face (eyebrows, sides of nose), and chest.
Distinction from Tinea: Primarily affects oily areas; the scales are often yellowish and greasy.
Pityriasis Rosea:
Appearance: Starts with a "herald patch" (larger, oval, scaly lesion), followed by smaller oval patches on the trunk in a "Christmas tree" pattern.
Distinction from Tinea: The pattern and progression are highly characteristic.
Erythema Annulare Centrifugum:
Appearance: Slow-growing, ring-shaped lesions with a trailing scale inside the border.
Distinction from Tinea: The scale is trailing (inside the ring), whereas in tinea, it's typically leading (on the outer, active border).
Bacterial Infections (e.g., Impetigo):
Appearance: Red sores that quickly rupture, ooze, and form a honey-colored crust.
Distinction from Tinea: Presence of pus, crusting, and often more rapid onset; bacterial cultures would be positive.
The Serious Look-Alikes: Cysts and Skin Cancer
Perhaps the most critical reason for professional evaluation when a rash or lesion is atypical or persistent is to rule out more serious conditions, specifically cysts and skin cancer.
Cysts
Cysts are sacs or pockets of tissue that contain fluid, air, or other substances. They can occur anywhere on the body and can sometimes be mistaken for other skin issues, including infections if they become inflamed.
Types of Cysts: There are numerous types, such as epidermal cysts, pilar cysts, ganglion cysts, and sebaceous cysts. Some can grow quite large, become painful, or get infected. For a comprehensive overview, see 17 Types of Cysts.
Why They Matter: While benign, cysts can cause discomfort, cosmetic concerns, and can sometimes mimic more serious conditions. A professional evaluation can determine if a cyst needs removal. For options, refer to Barrie Mole Cyst Removal or general information at AJAX Mole Cyst Skin Tag Removal.
Skin Cancer
This is perhaps the most crucial differential diagnosis. Early detection of skin cancer dramatically improves prognosis. Some forms of skin cancer can present as red, scaly patches, mimicking fungal infections.
Basal Cell Carcinoma (BCC): Can appear as a red, scaly patch, often with a raised, pearly border. It may bleed easily or fail to heal. Learn more about BCC Skin Cancer.
Squamous Cell Carcinoma (SCC): Often presents as a red, scaly, crusty patch or an open sore, which may be tender. It can grow into a firm lump. Understanding Actinic Keratosis to SCC: Understanding Pre-Cancerous Lesions is vital for early detection.
Melanoma: Though typically appearing as dark, irregularly shaped moles, some rare forms of melanoma can be red or amelanotic (lacking pigment), making them harder to distinguish. For advanced cases, see Advanced Melanoma Stages.
Bowen's Disease (Squamous Cell Carcinoma in Situ): Presents as a persistent, red, scaly patch that slowly enlarges, often mistaken for eczema or tinea. Learn more about Bowen's Disease Explained.
When in doubt, get it checked out. If you have a persistent skin lesion that doesn't respond to conventional treatments, changes in appearance, or raises any suspicion, consult a dermatologist or a skin cancer specialist. Clinics like Best Skin Cancer Clinic Toronto are equipped to provide expert diagnosis and treatment. Prompt professional evaluation is the best course of action to rule out serious conditions and ensure appropriate care for "when it's not a fungus (cyst/skin cancer)."
Advanced Insights into Tinea Management and Prevention for 2025
As we move further into 2025, the principles of managing and preventing tinea infections remain rooted in good hygiene and effective antifungal agents. However, advancements in medical understanding and lifestyle changes continually refine our approach. This section offers advanced insights and emphasizes proactive strategies for maintaining skin health.
Comprehensive Prevention Strategies
Preventing tinea cruris, tinea versicolor, and tinea corporis explained goes beyond simply using antifungal creams. It involves a holistic approach to skin care and environmental management:
Strict Personal Hygiene:
Daily Showering: Shower daily, and immediately after intense physical activity or heavy sweating. Use a mild soap.
Thorough Drying: Crucially, thoroughly dry all skin folds, especially the groin, armpits, and between toes, after showering. A towel specifically for these areas, changed frequently, can be beneficial.
Antifungal Powders: In areas prone to excessive moisture (like the groin or feet), consider using antifungal powders containing miconazole or cornstarch-based powders to keep skin dry.
Appropriate Clothing and Footwear:
Breathable Fabrics: Opt for loose-fitting clothing made from natural, breathable fibers like cotton, especially for underwear, socks, and everyday wear. These materials allow air circulation and wick away moisture.
Avoid Tight Synthetics: Tight synthetic clothing (nylon, polyester) traps heat and moisture, creating an ideal environment for fungal growth.
Change Clothes Regularly: Change underwear, socks, and sweaty workout clothes daily, or more often if damp.
Proper Footwear: If prone to athlete's foot (tinea pedis), wear well-ventilated shoes, alternate shoes daily to allow them to dry out, and wear cotton or moisture-wicking socks. Treating tinea pedis prevents spread to other areas like the groin (tinea cruris).
Environmental Control:
Humidity Management: In humid climates, using dehumidifiers indoors can help reduce ambient moisture that contributes to fungal growth.
Clean Living Spaces: Regularly clean and disinfect showers, gym equipment, and communal areas, especially if you share living spaces.
Pet Care: If you have pets, ensure they are regularly checked for skin conditions, particularly if family members have recurrent tinea corporis.
Avoid Sharing Personal Items:
Towels, Clothing, Razors: Never share these items. Fungi can easily transfer from one person to another via contaminated objects.
Sports Equipment: Clean and disinfect sports equipment (helmets, pads) regularly.
Immune System Support:
A healthy diet, regular exercise, adequate sleep, and stress management contribute to a robust immune system, which can help the body resist infections.
If you have a compromised immune system due to medical conditions or medications, discuss specific preventive strategies with your healthcare provider.
Emerging Treatments and Research (2025 Outlook)
While conventional topical and oral antifungals remain the gold standard for tinea infections, research continues to explore new avenues for treatment, particularly for resistant or recurrent cases.
Novel Antifungal Agents: Pharmaceutical research is always seeking new compounds with enhanced efficacy and reduced side effects. New classes of antifungals or improved formulations of existing ones may emerge in the coming years.
Biologic and Immunomodulatory Therapies: For very severe or recalcitrant fungal infections, especially in immunocompromised individuals, there's ongoing research into therapies that modulate the immune system to better combat fungal pathogens.
Adjunctive Therapies: Exploring the role of adjunctive therapies, such as specific skin barrier repair agents or microbiome-balancing products, could enhance treatment outcomes and prevent recurrence. The skin microbiome plays a crucial role in skin health, and understanding its balance is an area of active research.
Diagnostic Advancements: Faster and more accurate diagnostic tools, such as advanced molecular tests for identifying fungal species, can lead to more targeted and effective treatments.
For the vast majority of people, the classic understanding of tinea cruris, tinea versicolor, and tinea corporis explained, combined with readily available treatments, will be sufficient. However, staying informed about ongoing research helps improve overall dermatological care.
The Role of a Dermatologist or Healthcare Provider
For any persistent, spreading, painful, or unusual skin condition, a consultation with a healthcare provider, ideally a dermatologist, is paramount. They possess the expertise to:
Accurately Diagnose: Distinguish between various skin conditions that might look alike, including different types of fungal infections, eczema, psoriasis, and more serious conditions like skin cancer or cysts. A diagnostic tool like a skin biopsy might be necessary for definitive diagnosis, as described in Best Skin Biopsy Skin Cancer Screening in Mississauga.
Prescribe Appropriate Treatment: Recommend the most effective topical or oral antifungal medications based on the specific type of infection, its severity, and the patient's overall health.
Monitor for Side Effects: Oversee treatment with oral antifungals, which can have systemic side effects, and adjust as necessary.
Provide Preventive Advice: Offer personalized advice on how to prevent recurrence, especially for chronic or recurrent infections like tinea versicolor.
Refer to Specialists: If the condition is complex or requires surgical intervention (e.g., cyst removal), they can refer to appropriate specialists. The Minor Surgery Center, for example, is equipped for various minor surgical procedures.
Remember, self-diagnosis and self-treatment have limitations. While over-the-counter options are effective for many mild cases, professional guidance ensures safety and efficacy. When faced with a perplexing skin issue, leveraging the knowledge of a professional is always the best course of action.
Conclusion
Understanding tinea cruris, tinea versicolor, and tinea corporis explained is a crucial step towards maintaining optimal skin health. These common fungal and yeast infections, while distinct in their causes and presentations, share a common thread: they thrive in specific environmental conditions and are treatable with appropriate antifungal agents. Tinea corporis, the classic "ringworm," manifests as ring-shaped, itchy lesions. Tinea cruris, or "jock itch," targets the groin with intense itching and a well-defined rash. Tinea versicolor, caused by yeast, presents as discolored patches that may or may not itch.
While many cases respond well to accessible topical treatments and diligent hygiene, recognizing when to seek professional medical advice is paramount. Persistent symptoms, widespread infection, or any skin lesion that raises concern warrant a visit to a healthcare provider. This ensures accurate diagnosis, rules out conditions that mimic fungal infections—including cysts or skin cancer—and leads to the most effective treatment plan.
By embracing good hygiene practices, wearing appropriate clothing, and acting promptly on suspicious skin changes, individuals can effectively prevent and manage these common tinea infections, safeguarding their skin health for 2025 and beyond.
Actionable Next Steps:
Assess Your Symptoms: If you suspect a tinea infection, compare your symptoms with the descriptions provided in this article.
Try Over-the-Counter Treatment (for mild cases): For non-severe cases of tinea corporis or tinea cruris, consider an over-the-counter antifungal cream containing terbinafine or butenafine for 2-4 weeks. For tinea versicolor, selenium sulfide or ketoconazole shampoo can be effective.
Prioritize Hygiene: Implement rigorous hygiene practices, including thorough drying of skin, wearing breathable fabrics, and avoiding sharing personal items.
Monitor Progress: Keep an eye on the affected area. If there's no improvement after a few weeks, or if the condition worsens, spreads, or causes significant discomfort, proceed to step 5.
Consult a Healthcare Professional: Schedule an appointment with your doctor or a dermatologist for an accurate diagnosis and personalized treatment plan. Early professional intervention is key, especially if you have an atypical rash or any concerns about cysts or skin cancer. You can find comprehensive care for various skin conditions, including potential skin cancer screenings, at The Minor Surgery Center.
Remember, your skin is your body's largest organ – treat it with the care and attention it deserves.
References
[1] Tinea Infections. American Academy of Dermatology Association. Accessed [Current Date]. [2] Jock Itch (Tinea Cruris). Mayo Clinic. Accessed [Current Date]. [3] Pityriasis Versicolor. National Organization for Rare Disorders. Accessed [Current Date]. [4] Elgash, M., et al. (2019). Tinea Corporis. StatPearls Publishing. [5] Gupta, A. K., & Summerbell, R. C. (2000). Tinea corporis, tinea cruris, tinea pedis and tinea manuum: a review. Medical Mycology, 38(4), 251-287.