Last updated: July 7, 2026
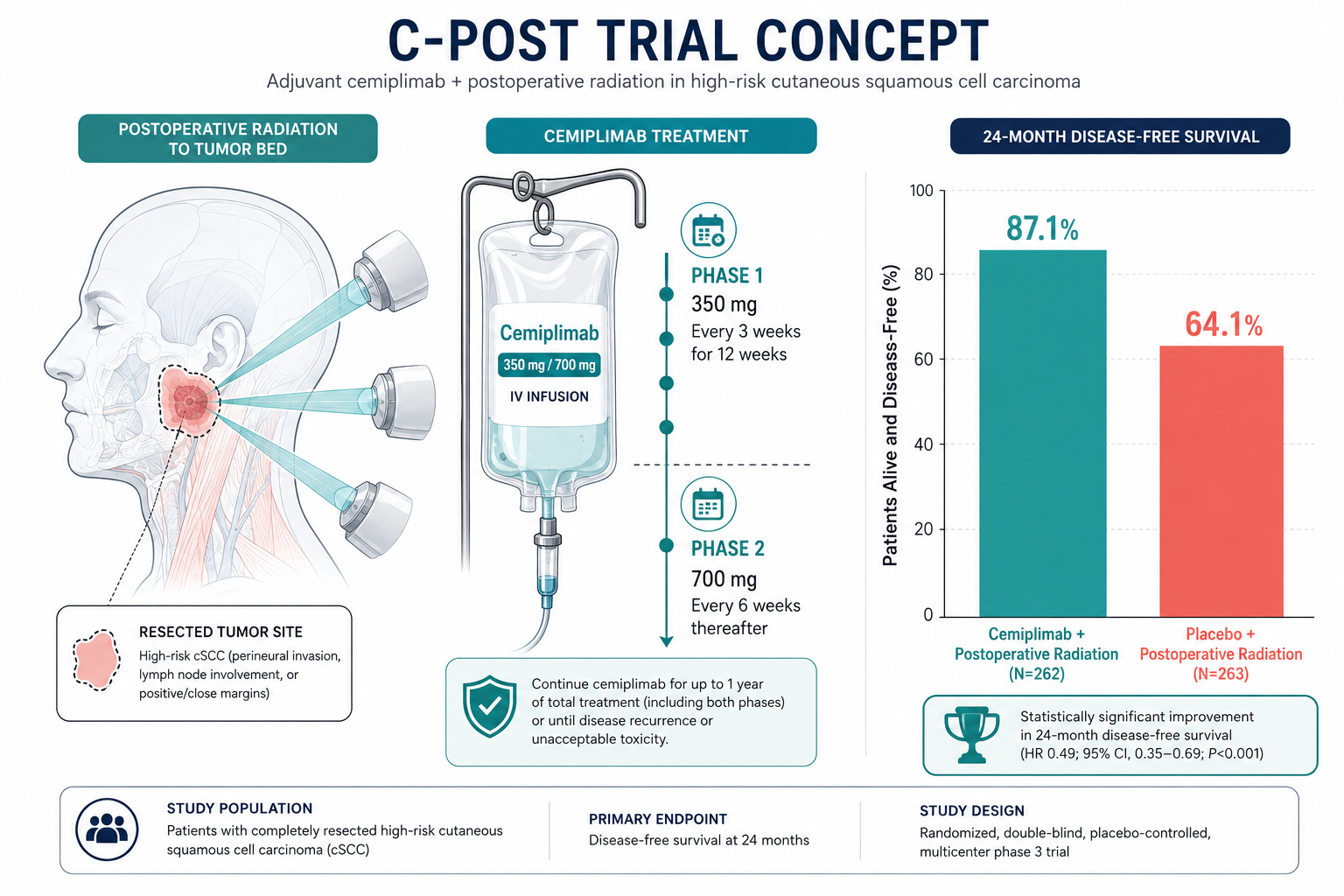
Yes, for a narrow group of very high-risk patients. A 2025 phase 3 trial called C-POST, published in the New England Journal of Medicine, showed that adjuvant cemiplimab given after surgery and radiation cut the risk of recurrence or death by 68% compared with placebo in adults with high-risk cutaneous squamous cell carcinoma (cSCC). The U.S. FDA approved this use in October 2025. It does not apply to routine SCC removed in a minor surgery setting, only to specific post-operative cases with features like major nodal involvement, extracapsular spread, or named-nerve invasion.
Squamous cell carcinoma (SCC) is the second most common skin cancer, growing from the flat squamous cells in the outer layer of skin. Most cases are cured with a straightforward surgical removal, sometimes with radiation added for higher-risk lesions.
Cutaneous SCC usually shows up as a scaly red patch, a firm bump, a sore that won't heal, or a wart-like growth, often on sun-exposed skin like the face, ears, scalp, neck, or backs of the hands. For a visual reference, see our guide to squamous cell carcinoma stages with pictures.
Standard treatment ladder:
For most people, that's where the story ends. But for a small subset of patients whose pathology shows aggressive features, the risk of recurrence stays high even after "successful" surgery. That's the group this new research is aimed at.
Yes, but only for a specific high-risk group. The 2025 C-POST phase 3 trial showed a large recurrence reduction with adjuvant cemiplimab after surgery and radiation. This is now the first proven post-surgery systemic drug option for high-risk cutaneous SCC.
Here's what makes C-POST different from earlier attempts:
Locoregional recurrence dropped by 80% and distant recurrence dropped by 65% versus placebo [3]. Those are unusually strong numbers for an adjuvant oncology trial.
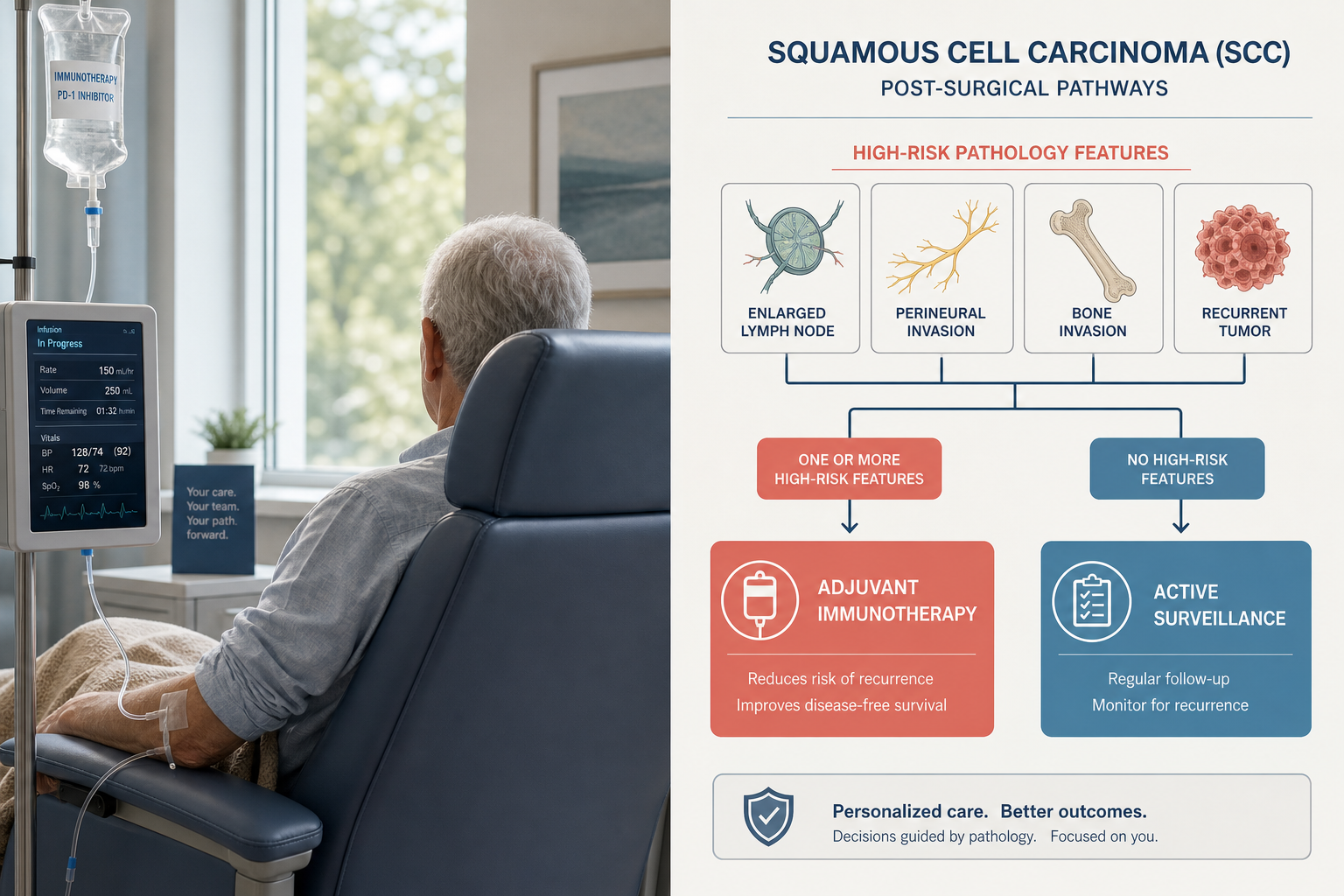
Decision rule: If pathology after your SCC surgery shows only "standard" features (clear margins, thin tumor, no perineural or lymphovascular invasion), you almost certainly won't need immunotherapy. If it shows nodal disease with extracapsular extension, three or more positive nodes, T4 bone invasion, named-nerve perineural invasion, or locally recurrent disease with extra risk features, that's when a medical oncology conversation about adjuvant cemiplimab becomes appropriate.
The two big adjuvant trials for high-risk cSCC, C-POST (cemiplimab) and KEYNOTE-630 (pembrolizumab), landed very differently in 2024-2025. C-POST was positive; KEYNOTE-630 was stopped for futility on its primary endpoint but still showed a signal of benefit.
C-POST (cemiplimab):
KEYNOTE-630 (pembrolizumab):
Why the different results? The two trials used different eligibility definitions, different dosing, and different endpoint hierarchies. C-POST enriched more aggressively for very-high-risk features. That's a lesson in cSCC research: how you define "high risk" changes everything.
There's also active work moving immunotherapy earlier, before surgery instead of after. The ongoing NRG-HN014 phase 3 trial is testing neoadjuvant cemiplimab followed by response-adapted surgery for locally advanced cutaneous head-and-neck SCC. That trial is specifically stratified to include immunosuppressed patients and advanced nodal disease, populations C-POST excluded.
Decisions come from your pathology report plus multidisciplinary review. Adjuvant cemiplimab is generally considered only if surgery + planned or completed radiation are already part of the plan AND the pathology shows one of the C-POST high-risk features.
The C-POST eligibility features are a practical starting checklist:
Nodal high-risk features (either one qualifies):
Non-nodal high-risk features (any one qualifies):
Beyond those, doctors also weigh:
Your pathology report is the anchor document for this whole conversation. If you're not sure how to read yours, our walk-through of a pathology report after mole or lesion removal can help you understand which findings matter.
Cemiplimab is expensive, U.S. list price is roughly USD $10,000,$12,000 per dose, and a full adjuvant course involves multiple infusions over 48 weeks, easily exceeding USD $250,000 without coverage. In Canada, cost is generally borne by provincial cancer programs or private insurance rather than the patient directly, but coverage timing after the 2025 approval varies by province.
Practical cost realities in 2026:
For context on more routine skin surgery pricing that patients often pay out of pocket, see our minor surgery pricing page.
Immunotherapy trains your immune system to attack cancer cells; chemotherapy directly kills fast-dividing cells (both cancerous and healthy). For advanced or high-risk cSCC, immunotherapy has largely replaced chemotherapy as the systemic treatment of choice.
FeatureImmunotherapy (PD-1 inhibitors)Traditional ChemotherapyMechanismBlocks PD-1 so T-cells attack tumorDirectly damages dividing cellsTypical scheduleEvery 3-6 weeks for up to 12 monthsMulti-day cycles, more frequentHair lossRareCommonKey side effectsImmune-related: thyroid, skin, colitis, lungsNausea, low blood counts, infection riskAdjuvant use in cSCCFDA-approved (cemiplimab, 2025)Not standardDurability of responseOften long-lasting when it worksUsually shorter
The bigger picture: chemotherapy was never a great fit for cSCC. Cetuximab (an EGFR-targeted drug) had modest activity, and platinum-based chemo had significant toxicity for often modest benefit. Immunotherapy has changed that entire landscape [8].
The best candidates are adults with completely resected cutaneous SCC, at least one C-POST high-risk feature on pathology, planned or completed postoperative radiation, good performance status, and no significant autoimmune or transplant history.
Good candidate profile:
Poor candidate profile:
Edge case: Immunosuppressed patients (transplant recipients, chronic lymphocytic leukemia, long-term steroid users) are the highest-risk group for cSCC in the real world but were excluded from C-POST. For these patients, decisions are made case-by-case with transplant medicine, dermatology, and medical oncology together.
Cemiplimab's main side effects are immune-related, the same immune system that's attacking tumor cells can also mistakenly attack healthy tissues. In C-POST, 23.9% of patients had grade 3 or higher adverse events vs 14.2% on placebo, and 9.8% stopped treatment because of side effects vs 1.5% on placebo.
Common (≥10% of patients):
Serious but less common:
The FDA label carries warnings for immune-mediated adverse reactions, infusion-related reactions, complications of allogeneic stem-cell transplantation, and embryo-fetal toxicity [1].
What patients often don't realize: Immune side effects can appear weeks or even months after a dose. Your oncology team monitors thyroid, liver, kidney, and blood counts throughout treatment, and any new symptom (persistent diarrhea, shortness of breath, unusual fatigue) needs to be reported promptly.
Reassuringly, patient-reported outcomes in C-POST showed that overall quality-of-life changes from baseline in global health, functioning, fatigue, and pain were small and similar between the cemiplimab and placebo arms, meaning most patients tolerated the treatment reasonably well from a day-to-day standpoint.
For high-risk patients who fit C-POST criteria, yes, the trial showed a 68% reduction in the risk of recurrence or death at 24 months. But immunotherapy doesn't eliminate recurrence risk entirely, and it hasn't yet proven to extend overall survival.
The numbers from C-POST [3]:
Important caveats:
The honest framing: adjuvant cemiplimab meaningfully reduces recurrence, but whether it saves more lives overall than treating recurrences when they happen is still being sorted out. For high-risk patients, most oncologists now favor the adjuvant approach because a recurrence, especially a distant one, can be far harder to control [4].
Recurrence after surgery ranges from a small local re-growth (usually re-excised or treated with radiation) to regional nodal spread or distant metastasis (which typically now involves systemic immunotherapy). The prognosis depends heavily on how early it's caught and where it comes back.
Local recurrence (at or near the original surgical site):
Regional recurrence (lymph nodes):
Distant metastasis (lung, liver, bone, other sites):
Follow-up is why this matters. Standard surveillance for high-risk cSCC includes clinical skin and lymph node exams every 3-6 months for the first 2 years, then less frequently. Any new skin lesion, lump, or symptom in a previously treated area deserves prompt evaluation. Understanding what normal healing looks like vs warning signs is useful for anyone recovering from skin surgery.
They aren't alternatives, they're used together. Radiation is a well-established local treatment that kills residual cancer cells at the surgical site or in nearby lymph nodes. Immunotherapy is a systemic treatment that targets microscopic disease anywhere in the body. In the C-POST trial, every patient received radiation first, then immunotherapy on top.
Radiation therapy after surgery:
Immunotherapy after surgery:
Decision rule: For high-risk cSCC after surgery, radiation is the first adjuvant step. If additional high-risk features are present, cemiplimab is added on top, not instead of. Skipping indicated radiation and substituting immunotherapy is not supported by the trial data.
The C-POST protocol runs up to 48 weeks, roughly 12 months of scheduled infusions. That's cemiplimab 350 mg IV every 3 weeks for the first 12 weeks (4 doses), then 700 mg every 6 weeks for another 36 weeks (6 more doses).
Total time commitment:
Each infusion visit takes about 30 minutes of drug administration plus check-in, labs, and monitoring, so plan on 2-3 hours per visit. Most patients continue normal work and daily life around the schedule.
The most common mistakes are skipping recommended follow-up, assuming a "clean margins" report means the risk is zero, ignoring new symptoms, and confusing routine SCC with the high-risk subset that needs multidisciplinary care.
Frequent pitfalls:
For very high-risk cSCC after surgery and radiation, there is currently no other systemic treatment with proven adjuvant benefit. Alternatives are mostly about optimizing surgery, radiation, and surveillance, or, in some cases, choosing active observation with prompt treatment of recurrence.
Non-immunotherapy options for reducing recurrence risk:
Emerging biology: Research into tumor biology, including work on ferroptosis resistance pathways like ALDH3A1 in squamous cell carcinoma, points toward future targets beyond checkpoint inhibitors. For now, though, cemiplimab is the only adjuvant systemic option with phase 3 evidence.
Active surveillance option: Some patients, especially those with significant comorbidities, transplant status, or personal preference against systemic treatment, reasonably choose surgery + radiation + close follow-up without adjuvant immunotherapy. This is a legitimate choice, particularly because cemiplimab remains an option if recurrence develops.
Is cemiplimab (Libtayo) the same as pembrolizumab (Keytruda)?
Both are PD-1 checkpoint inhibitors and work similarly, but they're different drugs made by different companies. In cutaneous SCC specifically, cemiplimab has a positive phase 3 adjuvant trial (C-POST) and FDA approval; pembrolizumab's adjuvant trial (KEYNOTE-630) did not meet its primary endpoint.
Does adjuvant cemiplimab cure squamous cell carcinoma?
It substantially reduces the risk of recurrence at 24 months but doesn't guarantee cure. Some patients still recur despite treatment, and overall survival benefit has not yet been definitively proven.
Can I get immunotherapy if I've had an organ transplant?
Solid organ transplant recipients were excluded from the C-POST trial because PD-1 inhibitors can trigger organ rejection. These decisions require careful multidisciplinary discussion between transplant medicine and oncology.
How soon after surgery does immunotherapy start?
In C-POST, cemiplimab began 2 to 10 weeks after completion of postoperative radiation therapy, so typically 2-4 months after the original surgery.
Will I lose my hair on immunotherapy?
Hair loss is uncommon with cemiplimab. It's a chemotherapy side effect, not a typical immunotherapy one. Skin rash and itching are more common.
Is this treatment available in Canada?
Cemiplimab is Health Canada, approved for advanced cSCC. Adjuvant coverage under provincial cancer agencies typically follows FDA/EMA approval; ask your oncologist about current provincial funding status.
What if my SCC is small and on my arm, do I need immunotherapy?
Almost certainly not. Small, low-risk SCCs excised with clear margins are cured by surgery in the overwhelming majority of cases. Adjuvant immunotherapy is only for the specific high-risk features identified in C-POST.
How is high-risk cSCC different from ordinary skin cancer?
"High-risk" in the C-POST sense means specific pathology findings: major nodal involvement, extracapsular extension, T4 bone invasion, named-nerve perineural invasion, in-transit metastases, or locally recurrent disease with added risk features. Most SCCs don't have these.
What's the biggest risk of adjuvant cemiplimab?
Immune-related adverse events, inflammation of organs like the colon, lungs, liver, thyroid, or endocrine glands. Most are manageable if caught early, but some can be serious.
Should I get a second opinion before starting adjuvant immunotherapy?
Given the cost, duration, and toxicity profile, a second opinion at a comprehensive cancer center is very reasonable, especially if you're on the borderline of eligibility criteria.
Can I still get sun after finishing treatment?
You'll need lifelong strict sun protection. A history of one SCC, especially a high-risk one, dramatically raises your risk of another skin cancer.
Are there any dietary or lifestyle changes that help recovery?
Standard post-surgical healing advice applies: protein-rich diet, avoid smoking, manage other health conditions well. See our guide to foods that speed healing after minor skin surgery for practical basics.
The C-POST trial is the clearest evidence yet that immunotherapy after surgery can meaningfully reduce recurrence in cutaneous squamous cell carcinoma, but only for a narrowly defined high-risk group. For the vast majority of people who have a routine SCC removed in an outpatient or minor surgery setting, this research doesn't change anything. Surgery, sometimes with radiation, remains the definitive treatment.
The people this actually matters to are those whose post-operative pathology shows aggressive features: significant nodal disease, extracapsular extension, T4 bone invasion, named-nerve perineural invasion, in-transit metastases, or locally recurrent tumors with additional risk factors. If that's you, a conversation with a medical oncologist, after radiation is planned or completed, is now the standard step.
Practical next steps:
If you're in the Greater Toronto Area and dealing with a new or suspicious skin lesion, the team at The Minor Surgery Center handles biopsies and small excisions across multiple clinics and can help ensure any suspicious lesion is evaluated and, if needed, referred appropriately. Understanding whether a skin change warrants professional evaluation is one of the most useful skills any patient can develop.
[1] FDA Approves Cemiplimab-rwlc for Adjuvant Treatment of Cutaneous Squamous Cell Carcinoma - https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-cemiplimab-rwlc-adjuvant-treatment-cutaneous-squamous-cell-carcinoma
[2] Libtayo (cemiplimab-rwlc) Approved in the U.S. as First and Only Immunotherapy for Adjuvant Treatment of Cutaneous Squamous Cell Carcinoma (CSCC) With a High Risk of Recurrence After Surgery and Radiation - https://www.globenewswire.com/news-release/2025/10/08/3163679/0/en/libtayo-cemiplimab-rwlc-approved-in-the-u-s-as-first-and-only-immunotherapy-for-adjuvant-treatment-of-cutaneous-squamous-cell-carcinoma-cscc-with-a-high-risk-of-recurrence-after-su.html
[3] Libtayo (cemiplimab) Phase 3 Data in Adjuvant Treatment Post Surgery and Radiation - https://newsroom.regeneron.com/news-releases/news-release-details/libtayor-cemiplimab-phase-3-data-adjuvant-treatment-post/
[4] Regeneron Announces Approval of Cemiplimab-rwlc for Adjuvant Treatment of Cutaneous Squamous Cell Carcinoma With a High Risk of Recurrence After Surgery and Radiation - https://aimwithimmunotherapy.org/press-releases/regeneron-announces-approval-of-cemiplimab-rwlc-for-adjuvant-treatment-of-cutaneous-squamous-cell-carcinoma-with-a-high-risk-of-recurrence-after-surgery-and-radiation/
[5] Adjuvant Immunotherapy in High-Risk Cutaneous Squamous Cell Carcinoma - https://consultqd.clevelandclinic.org/adjuvant-immunotherapy-in-high-risk-cutaneous-squamous-cell-carcinoma
[6] Recurrent Head and Neck Cutaneous Squamous Cell Carcinoma After Surgery and Radiotherapy - https://pubmed.ncbi.nlm.nih.gov/32627359/
[7] European Guidelines for Cutaneous Squamous Cell Carcinoma - https://pmc.ncbi.nlm.nih.gov/articles/PMC8427439/
[8] American Cancer Society: Treating Squamous Cell Skin Cancer - https://www.cancer.org/cancer/types/basal-and-squamous-cell-skin-cancer/treating/squamousl-cell-carcinoma.html



