Quick Answer: A corticosteroid injection into the flexor tendon sheath is the standard first-line treatment for trigger finger. Most patients receive one or two injections. A single shot relieves symptoms in roughly half of all patients, and a second injection raises that figure considerably. Symptoms often improve within one week. The injections work well for mild-to-moderate cases, but recurrence is possible, and surgery tends to produce better long-term results for severe or recurring cases.
Trigger finger (stenosing tenosynovitis) happens when the A1 pulley — a small band of tissue at the base of the finger — becomes thickened and inflamed. The flexor tendon that runs through it can no longer glide smoothly, causing the finger to catch, lock, or snap when bending or straightening.
Corticosteroids reduce local inflammation and swelling around the tendon sheath. When injected directly into or near the sheath, they can shrink the irritated tissue enough to let the tendon move freely again. The injection does not fix any structural narrowing permanently, but it gives the tissue a chance to calm down — and for many patients, that window of relief becomes permanent.
Why this matters for treatment decisions:
For a broader overview of treatment options, see the Trigger Finger Treatment & Surgery guide from The Minor Surgery Center.
The short answer: one or two injections, and yes, they work — but not for everyone.
Clinical guidelines and research consistently support one to two corticosteroid injections as first-line treatment for trigger finger [3]. Here is what the evidence shows:
MetricFindingSourceSuccess rate — single injection~54%[1]Overall success rate (1–2 injections)~68%[1]Time to symptom reliefUsually within 1 week[3]Maximum duration of reliefUp to 10 years in some patients[1]Average pain score (dorsal approach)3.8 / 10[1]Neurovascular injury risk (dorsal)2 out of 112 injections[1]
A 2018 study of 126 patients using the dorsal webspace approach found a 54% success rate after a single injection and a 68% overall success rate across the cohort [1]. Those are meaningful numbers for a non-surgical, office-based procedure.
What "success" means here: In most studies, success means the finger moves freely without triggering, locking, or significant pain — without the patient needing further treatment (a second injection or surgery).
Common mistake: Patients sometimes assume that if the first injection works initially but symptoms return, the treatment "failed." In reality, a second injection is still appropriate and often effective. Recurrence after the first shot does not automatically mean surgery is next.
Most clinicians recommend a maximum of two to three corticosteroid injections per finger over a lifetime. Beyond that, the risk-to-benefit ratio shifts.
Why the limit exists:
Typical injection schedule:
Choose injections if:
Choose surgery sooner if:
For patients in the Greater Toronto Area exploring both options, advances in trigger finger management covers newer techniques alongside traditional approaches.
The procedure is straightforward and typically takes under 10 minutes in a clinic setting.
Step-by-step process:
Palmar vs. dorsal approach:
Both approaches are safe and effective [1]. The dorsal webspace approach — entering from the back of the hand between the fingers — may cause less procedural pain. Research found the dorsal approach averaged a pain score of 3.8/10 and had a mean needle-to-neurovascular-bundle distance of 1.77mm, with only 2 neurovascular complications in 112 injections studied [1]. A 2024 clinical trial is actively comparing both approaches to further define which is preferable [1].
What you'll feel: A brief sting from the needle, possible pressure as the solution enters the sheath, and sometimes a temporary burning sensation from the anesthetic. Most patients tolerate it well without sedation.

It works well in the short to medium term for most patients — but it is not a guaranteed permanent fix.
Short-term (within 1 week): The majority of patients who respond to the injection notice improved finger movement and reduced pain within the first week [3]. The local anesthetic provides immediate (though temporary) relief, and the steroid effect builds over several days.
Medium-term (weeks to months): Many patients remain symptom-free for months after a successful injection. Some achieve lasting relief from a single shot.
Long-term (years): Studies have shown that steroid injections can ease symptoms for up to 10 years in some patients [1]. However, this is not universal. Recurrence is the main limitation.
Factors that reduce long-term success:
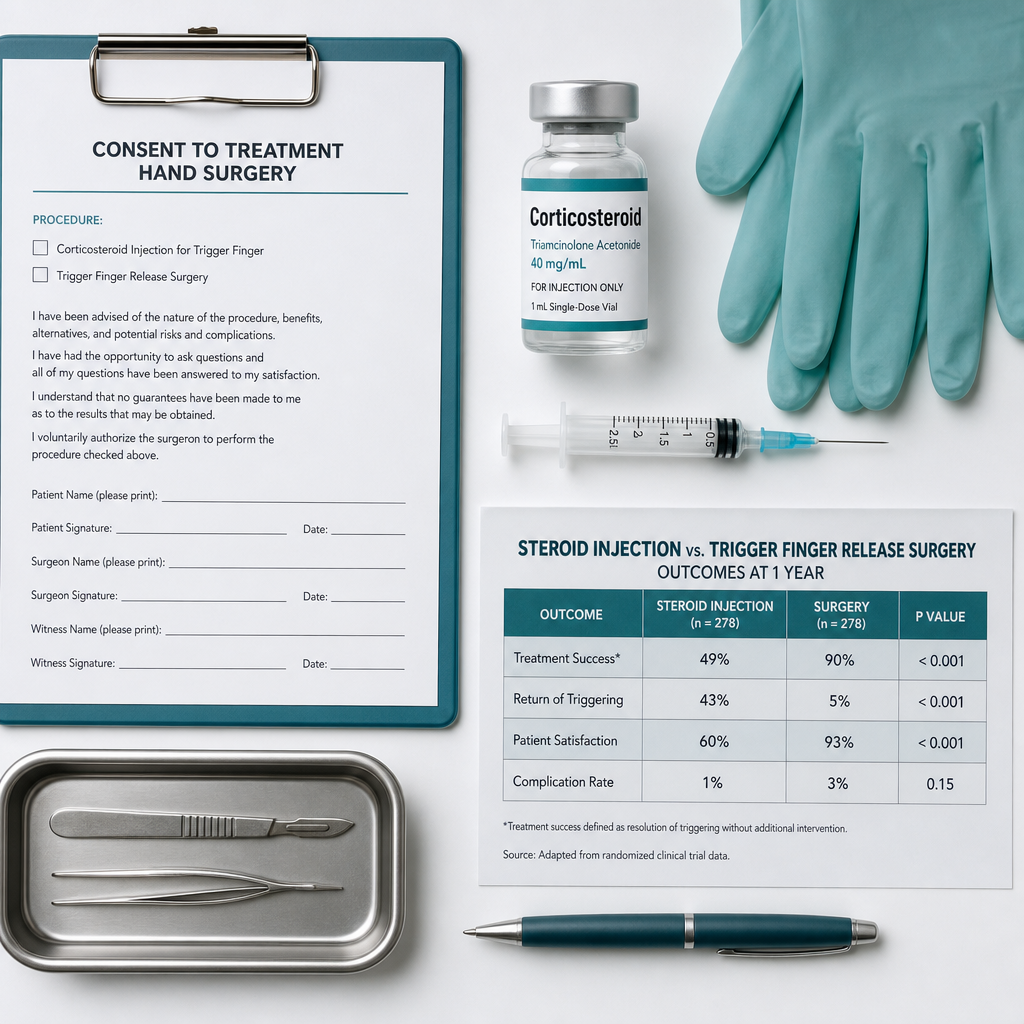
Injection vs. surgery at one year: Surgical trigger finger release provides better outcomes than a single steroid injection at the one-year mark and is generally considered a permanent cure [3]. That said, surgery carries its own recovery period and risks, so injections remain a reasonable first step for most patients.
A systematic review and meta-analysis currently underway through NCBI aims to more precisely quantify how steroid injections compare to other non-surgical and surgical treatments [2] — results from that work should help refine future guidelines.
Most adults with symptomatic trigger finger are reasonable candidates for a corticosteroid injection as a first step.
Good candidates:
Less ideal candidates or situations requiring extra caution:
Edge case — pregnancy: Corticosteroid injections are generally used with caution during pregnancy. The decision should involve the treating physician and, if relevant, an obstetrician.
Corticosteroid injections for trigger finger are generally safe, but side effects do occur.
Common, usually temporary:
Less common:
What to watch for after the injection:
Understanding where injections fit in the treatment ladder helps patients make informed decisions.
Treatment comparison overview:
TreatmentHow It WorksSuccess RateRecoveryBest ForSplinting / restImmobilizes finger to reduce inflammationModerate (mild cases)WeeksVery mild, early-stageCorticosteroid injectionReduces tendon sheath inflammation~54–68% per course [1]DaysMild to moderateUltrasound-guided injectionSame as above, with imagingPotentially higher accuracyDaysDifficult anatomy, recurrenceTrigger finger release (surgery)Cuts the A1 pulley to free the tendon>90% permanent cure [3]2–6 weeksFailed injections, severe casesPercutaneous needle releaseNeedle used to cut pulley without open incisionHigh, less evidence than open surgeryDays to 1 weekSelected patients
Key decision rule:
Patients dealing with related hand conditions may also find it useful to read about Dupuytren's contracture, which can co-exist with trigger finger and affects treatment planning.
For those in the Toronto region considering surgical options, the Trigger Finger Treatment & Surgery page outlines what the procedure involves and what to expect.
Recovery is usually quick. Most patients return to normal daily activities within a day or two.
First 24–48 hours:
Days 3–7:
Weeks 2–6:
Longer term:
Practical tips for recovery:
For patients whose hand problems relate to workplace ergonomics, the guide on desk job vs. manual labour return to work after carpal tunnel syndrome offers practical return-to-work advice that applies to trigger finger recovery as well.
Surgery becomes the better option in several clear situations.
Surgical trigger finger release involves cutting the A1 pulley under local anesthesia, freeing the tendon permanently. It is performed as a minor day procedure and has a success rate exceeding 90% with low complication rates [3].
Consider surgery if:
What surgery involves:
The surgical approach is well-established and has been refined over decades. For patients in the Toronto area, board-certified surgeons at The Minor Surgery Center perform trigger finger release — see the full team of expert surgeons to find the right specialist.
Q: How quickly does a trigger finger steroid injection work?
Most patients notice improvement within 3–7 days. The local anesthetic provides immediate (short-lived) relief, and the corticosteroid effect builds over several days. Full benefit is usually apparent by the end of the first week [3].
Q: How many steroid injections can you have in a trigger finger?
The general limit is two to three injections per finger over a lifetime. Most clinicians offer a second injection if the first provides partial or temporary relief, but recommend surgery if two injections fail. Beyond three injections, the risk of tendon damage increases without meaningful additional benefit.
Q: Does a trigger finger injection hurt?
The injection involves a brief needle sting and some pressure as the solution enters the sheath. Using the dorsal webspace approach, patients reported an average pain score of 3.8 out of 10 — uncomfortable but well-tolerated without sedation [1].
Q: Can trigger finger come back after a steroid injection?
Yes. Recurrence is the main limitation of injection therapy. The injection reduces inflammation but does not permanently widen the A1 pulley. Diabetic patients are at particularly higher risk of recurrence [3].
Q: Is a steroid injection better than surgery for trigger finger?
For mild-to-moderate cases, injections are a reasonable first step with fewer risks and faster recovery. However, surgery provides better outcomes at one year and is generally considered a permanent cure [3]. The right choice depends on severity, patient health, and personal preference.
Q: What steroid is used for trigger finger injections?
Triamcinolone acetonide and methylprednisolone are the most commonly used corticosteroids. They are typically mixed with a local anesthetic such as lidocaine to provide immediate pain relief alongside the longer-acting steroid effect.
Q: Can I have a trigger finger injection if I have diabetes?
Yes, but with caution. Corticosteroids can temporarily raise blood sugar for 1–3 days. Diabetic patients should monitor their glucose closely after the injection. They also face a higher recurrence risk, so earlier surgical referral may be appropriate [3].
Q: What is the success rate of a trigger finger steroid injection?
A single injection has approximately a 54% success rate. Overall success across one or two injections reaches approximately 68%, based on a study of 126 patients using the dorsal webspace approach [1].
Q: How long does relief from a trigger finger injection last?
Relief duration varies. Some patients remain symptom-free for years — studies show relief lasting up to 10 years in some cases [1]. Others experience recurrence within months. Severity, diabetes status, and how many fingers are affected all influence duration.
Q: Is ultrasound guidance necessary for trigger finger injections?
Not always. Experienced clinicians can perform accurate injections using anatomical landmarks. Ultrasound guidance can improve accuracy in difficult cases, obese patients, or when previous injections have failed — but it is not routinely required for straightforward cases.
Q: What happens if I do nothing about trigger finger?
Mild trigger finger sometimes improves on its own with rest. However, without treatment, moderate-to-severe cases tend to worsen. A finger that catches can progress to one that locks, and prolonged locking can lead to permanent stiffness or contracture.
Q: Can I drive after a trigger finger steroid injection?
Most patients can drive immediately after the injection, though it is advisable to wait until the local anesthetic has worn off (usually 1–2 hours) so normal hand sensation has returned. Check with the treating clinician based on which hand was injected.
Trigger finger steroid injection — how many shots, does it work? — is one of the most common questions patients ask when diagnosed with stenosing tenosynovitis. The evidence is clear: one to two corticosteroid injections are the appropriate first-line approach for most patients with mild-to-moderate trigger finger. A single injection resolves symptoms in roughly half of patients, and a second injection raises overall success to approximately 68% [1]. Relief typically appears within one week [3] and can last years for many patients [1].
Injections are not a permanent structural fix, and recurrence is real — especially for diabetic patients [3]. When two injections fail, or when the finger is severely locked, surgical trigger finger release is the more reliable long-term solution, with better outcomes at one year [3].
Actionable next steps:
[1] Phase Trigger Finger Disorder 6 2024 0b475 - https://www.withpower.com/trial/phase-trigger-finger-disorder-6-2024-0b475
[2] Pmc12666073 - https://pmc.ncbi.nlm.nih.gov/articles/PMC12666073/
[3] Trigger Finger Release In Adults - https://www.hweclinicalguidance.nhs.uk/clinical-policies/trigger-finger-release-in-adults/
[4] What Is The Recommended Treatment For Trigger Finger - https://www.droracle.ai/articles/959369/what-is-the-recommended-treatment-for-trigger-finger
[5] thepermanentejournal - https://www.thepermanentejournal.org/doi/10.7812/TPP/24.151
[6] meeting.handsurgery - https://meeting.handsurgery.org/program/2026/HS2.cgi
[7] Nct01886157 - https://www.patlynk.com/trial/NCT01886157
Last updated: May 5, 2026



