Last updated: May 5, 2026
Quick Answer: Trigger finger in children — pediatric stenosing tenosynovitis — is a condition where a child's finger or thumb gets stuck in a bent position due to inflammation and narrowing around the flexor tendon sheath. It's most common in the thumb of children under age 3. Up to 60% of cases in very young children resolve on their own, but the spontaneous resolution rate drops to under 10% after age 2, making early assessment important. Treatment ranges from watchful waiting and splinting to surgery, depending on the child's age and symptom severity.
Trigger finger in children — pediatric stenosing tenosynovitis — is a condition where the flexor tendon that bends a finger or thumb becomes unable to glide smoothly through the fibrous tunnel (called the tendon sheath) that surrounds it. The result is a finger that catches, clicks, or locks in a flexed position.
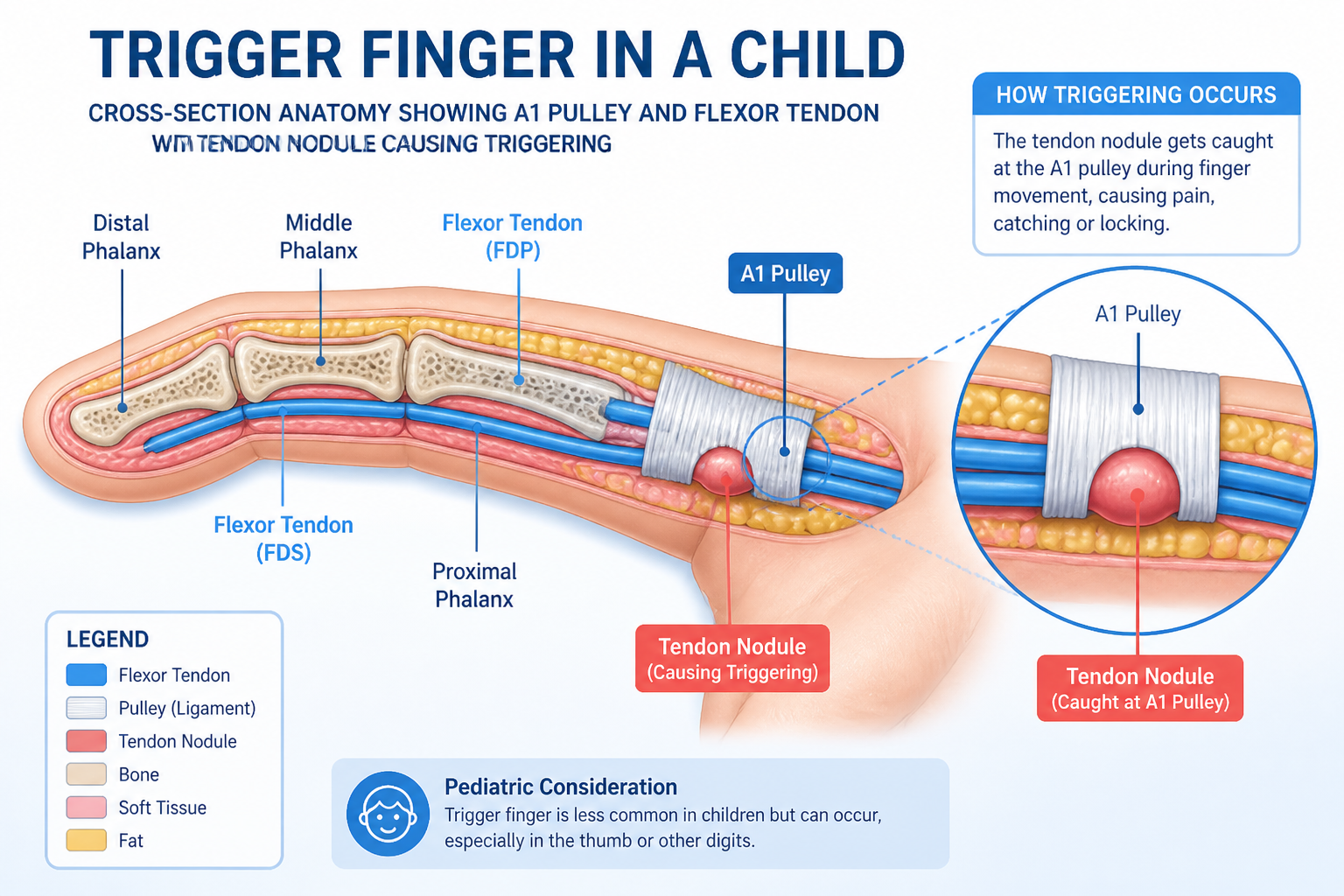
Each finger has a flexor tendon that runs through a series of tight fibrous rings called pulleys. The first of these, the A1 pulley, sits at the base of the finger. In stenosing tenosynovitis, this pulley becomes thickened and narrowed, or a nodule forms on the tendon itself. Either way, the tendon can no longer pass through cleanly.
In children, the problem is slightly different from adults:
Adult trigger finger is typically linked to repetitive gripping, diabetes, or rheumatoid arthritis. In children, the cause is usually structural — a size mismatch between the tendon and the pulley — rather than inflammatory or degenerative. This distinction matters for treatment planning.
For a broader look at trigger finger across age groups, the Trigger Finger Treatment & Surgery resource offers a useful overview of how the condition is managed in different populations.
Pediatric stenosing tenosynovitis most commonly affects children between ages 1 and 3, with trigger thumb being the dominant presentation. It can appear in older children and adolescents, but this is less common.
Key risk factors and associations:
💡 Clinical note: Because severe symptoms in one finger can mask early triggering in adjacent digits, a complete examination of all fingers — not just the symptomatic one — is recommended at every visit [1].
The symptom pattern in pediatric stenosing tenosynovitis follows a predictable course, which helps clinicians and parents recognize the condition early.
Three-stage progression [1]:
StageWhat Parents and Clinicians SeeStage 1 — ClickingA painless snap or click when the finger moves; child may not noticeStage 2 — TriggeringFinger catches or locks during bending or straightening; may be painfulStage 3 — Fixed flexionFinger stays bent and cannot be straightened, even passively
In infants and toddlers, the thumb is often found stuck in a bent position. Parents commonly notice it when dressing the child or during play. Older children may complain of pain or difficulty gripping objects.
What to watch for:
Diagnosis of trigger finger in children — pediatric stenosing tenosynovitis — is based on clinical examination. No blood tests or imaging are required in most cases.
The clinical exam includes:
Ultrasound may be used in complex or atypical cases to visualize the tendon and pulley, and research confirms it can detect changes in tendon and pulley size after treatment [1]. However, it is not part of routine diagnosis.
When to see a specialist: If a child's thumb or finger is locked in flexion and cannot be straightened with gentle pressure, or if symptoms have persisted beyond a few weeks without improvement, a referral to a pediatric hand surgeon or orthopedic specialist is appropriate.
For families dealing with other pediatric hand and wrist conditions, the guide on carpal tunnel syndrome in children and teens covers a related condition that sometimes co-occurs with trigger digit.
Non-surgical treatment is the appropriate first step for most children with trigger finger in children — pediatric stenosing tenosynovitis, especially those under age 2 or with mild-to-moderate symptoms.

For children under age 2, watchful waiting combined with gentle passive extension exercises is often the first recommendation. Parents are taught to gently straighten the affected thumb or finger several times daily.
Choose observation if: The child is under 2, the finger is not completely locked, and there are no signs of rapid progression.
Splinting holds the finger in an extended position to reduce triggering and allow the tendon sheath to recover.
Common mistake: Using the wrong joint level for splinting. PIP-blocking orthoses appear superior to MCP splints for symptom control [1]. A hand therapist should fit and monitor the splint.
Steroid injections into or around the tendon sheath reduce inflammation and can shrink the A1 pulley.
Edge case: In older children or adolescents with trigger finger, corticosteroid injection is a reasonable step before surgery, particularly when splinting has not resolved symptoms.
Overall, non-surgical management (observation plus splinting) resolved symptoms in 57.8% (37 of 64) fingers across studies [6]. This is a meaningful success rate, but it also means roughly 4 in 10 children will eventually need surgery.
Surgery becomes appropriate when conservative treatment fails, when the finger is completely locked, when the child is over age 2 with no sign of spontaneous improvement, or when multiple digits are involved.

The standard surgical procedure for pediatric trigger finger is A1 pulley release — a minor operation in which the surgeon divides the narrowed pulley to give the tendon room to glide freely.
Key outcomes:
Percutaneous release (using a needle rather than an open incision) is an option in some cases, though open release remains the standard in pediatric patients due to the need for precision around small structures.
When multiple fingers are affected, conservative treatment is less likely to succeed. Multiple affected digits and higher symptom severity are both associated with lower odds of resolution without surgery [1]. In these cases, surgical planning should address all involved digits.
If a child has both trigger finger and carpal tunnel syndrome, concurrent surgical release of both conditions is often more appropriate than staged procedures [1]. For context on what carpal tunnel surgery recovery looks like, the article on carpal tunnel surgery recovery provides useful detail for families navigating that process.
The table below summarizes success rates across the main treatment approaches, based on available evidence.
Treatment ApproachResolution RateBest Suited ForObservation alone~52% [6]Children under 2, mild symptomsSplinting~67% [6]Acute onset (<3 months), cooperative childrenCorticosteroid injectionVariable; improves tendon/pulley size [1]Older children, failed splintingSurgical A1 pulley release80–90% [1]Failed conservative care, fixed flexion, age >2
Key insight: Age at diagnosis is one of the strongest predictors of outcome. Children under 2 have a reasonable chance of spontaneous resolution; children over 2 almost certainly need active treatment, and many will eventually require surgery if conservative measures fail.
Leaving trigger finger in children — pediatric stenosing tenosynovitis — untreated carries real risks, particularly for hand development and function.
Potential consequences of delayed treatment:
The good news is that early surgical intervention — even in toddlers — carries a high success rate and does not prevent normal hand development or sports participation [5].
Q: Is trigger finger in children painful?
In the early clicking stage, it is often painless. As the condition progresses to active triggering or locking, children may experience pain or discomfort, particularly when trying to straighten the finger. Young children may not verbalize pain but may avoid using the affected hand.
Q: Can trigger thumb in babies resolve on its own?
Yes — 30–60% of cases in children under age 2 resolve spontaneously [7]. After age 2, spontaneous resolution drops to under 10%, so active treatment is usually recommended if the condition persists.
Q: At what age should surgery be considered?
Most specialists recommend surgical A1 pulley release if the condition has not resolved by age 2–3, or sooner if the finger is completely locked or if the child is older at diagnosis. Waiting beyond age 3–4 increases the risk of permanent joint stiffness.
Q: How long does recovery from A1 pulley release take in children?
Most children recover within a few weeks. The small incision heals quickly, and full hand function typically returns within 4–6 weeks. Children can usually return to normal activities, including sports, after healing is confirmed [5].
Q: Is splinting effective for trigger finger in children?
Splinting resolves symptoms in roughly 67% of patients when used appropriately [6]. PIP joint-blocking orthoses appear more effective than MCP splints [1]. A hand therapist should fit the device and guide the treatment duration (typically 3–12 weeks).
Q: Can trigger finger affect multiple fingers at once in a child?
Yes. Multiple digit involvement is possible, especially in children with underlying conditions like Down syndrome or juvenile arthritis. When multiple fingers are affected, conservative treatment is less likely to succeed, and surgical management is often warranted [1].
Q: Do corticosteroid injections work for pediatric trigger finger?
They can be effective, particularly in older children. Ultrasound evidence confirms improvement in tendon and pulley size after injection [1]. Subcutaneous and intrasheath injections produce equivalent results, making the procedure more accessible in clinical settings.
Q: Is pediatric trigger finger the same as adult trigger finger?
The symptoms are similar, but the underlying cause differs. Children typically have a structural size mismatch between the tendon and pulley, while adults are more likely to have inflammatory or degenerative causes. Treatment approaches overlap but are tailored to the child's age and anatomy.
Q: What other hand conditions should be checked for in a child with trigger finger?
Clinicians should examine all digits carefully, as triggering in one finger can mask early involvement in others [1]. Carpal tunnel syndrome can also co-exist with trigger finger in children and may require concurrent treatment [1].
Q: Will my child's hand develop normally after treatment?
Yes. When treated appropriately, most children achieve full finger extension and normal hand function. Early treatment reduces the risk of permanent contracture, and post-surgical outcomes are excellent in the vast majority of cases [5].
Trigger finger in children — pediatric stenosing tenosynovitis — is a manageable condition with good outcomes when recognized and treated at the right time. Here's what to do based on the child's situation:
For parents:
For clinicians:
For families in the Toronto area seeking expert evaluation of pediatric hand conditions, the Minor Surgery Center's trigger finger treatment page outlines available options. You can also explore recent advances in trigger finger management for a broader view of how treatment approaches are evolving.
If your child has been diagnosed with a related condition, the guide on carpal tunnel syndrome in children and teens and the overview of congenital moles and birthmarks in children may also be useful resources for navigating pediatric surgical decisions.
Early action makes a real difference. A locked finger in a toddler is not something to watch indefinitely — but with the right care at the right time, outcomes are consistently excellent.
[1] Pmc12476290 — https://pmc.ncbi.nlm.nih.gov/articles/PMC12476290/
[2] Trigger Finger Stenosing Tenosynovitis — https://www.massgeneral.org/orthopaedics/hand/conditions-and-treatments/trigger-finger-stenosing-tenosynovitis
[3] Trigger Finger Thumb — https://www.nicklauschildrens.org/conditions/trigger-finger-thumb
[4] Trigger Finger Adult Pediatric Hand Upper Extremity Surgeon New York — https://www.aarondaluiskimd.com/trigger-finger-adult-pediatric-hand-upper-extremity-surgeon-new-york.html
[5] Pediatric Trigger Thumb — https://www.childrenscolorado.org/health-professionals/publications/charting-pediatrics-podcast/pediatric-trigger-thumb/
[6] Pmc6005211 — https://pmc.ncbi.nlm.nih.gov/articles/PMC6005211/
[7] Trigger Finger 2 — https://chortho.com/trigger-finger-2/
[8] Spontaneous Resolution Of Early Onset Pediatric Trigger Thumb A Case Study — https://www.cureus.com/articles/343314-spontaneous-resolution-of-early-onset-pediatric-trigger-thumb-a-case-study
[9] Pediatric Trigger Digits — https://publications.aap.org/pediatricsinreview/article/43/4/191/185596/Pediatric-Trigger-Digits



