Last updated: May 20, 2026
Quick Answer: Skin cancer spots are abnormal growths or lesions on the skin caused by the uncontrolled division of damaged skin cells. They range from pearly or waxy bumps (basal cell carcinoma) to irregular, multi-colored moles (melanoma) to rough, scaly patches (squamous cell carcinoma). Early detection dramatically improves outcomes — most skin cancers are treatable when caught at an early stage.
Skin cancer spots don't follow a single appearance — they vary significantly by cancer type, location, and how long they've been present. The most important visual cues come from understanding the three main cancer types and how each one tends to present on the skin.
Basal cell carcinoma is the most common form and usually appears on sun-exposed areas like the face, neck, and hands. Key visual signs include:
For a deeper look at this specific cancer type, the guide to BCC skin cancer covers its stages and treatment options in detail.
SCC tends to appear as:
Actinic keratosis — rough, scaly patches caused by years of sun exposure — is a well-recognized precursor to SCC. Understanding the progression from actinic keratosis to SCC can help people catch the warning signs before full malignancy develops.
Melanoma is the most serious type and can appear anywhere on the body, including areas rarely exposed to sun. It typically looks like:
💡 Key visual rule: A normal mole is usually round, uniform in color, smaller than 6mm, and stable over time. Any spot that breaks these norms warrants professional evaluation.
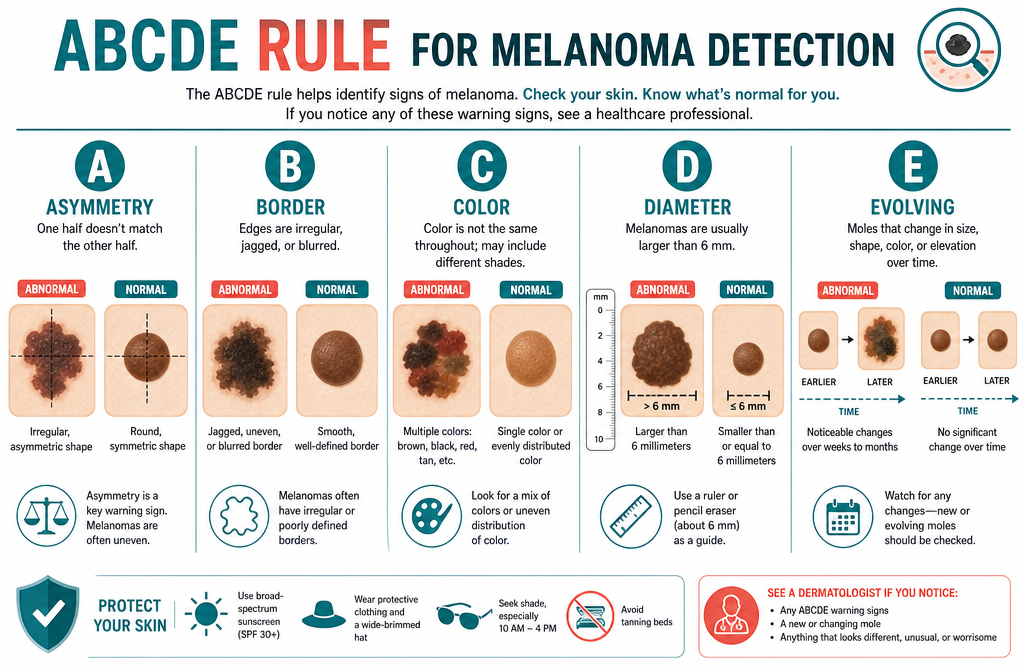
The difference between a harmless mole and melanoma often comes down to the ABCDE criteria, a dermatologist-developed framework used worldwide. A regular mole is symmetrical, has smooth borders, is a single shade of brown, stays under 6mm, and doesn't change. Melanoma typically fails one or more of these criteria.
FeatureBenign MoleMelanomaAsymmetrySymmetrical halvesOne half doesn't match the otherBorderSmooth, well-definedIrregular, ragged, or blurredColorUniform tan or brownMultiple shades, may include red or blackDiameterUsually under 6mmOften larger than 6mmEvolvingStable over yearsChanges in weeks or months
An additional warning sign sometimes called the "ugly duckling" sign: if one mole looks noticeably different from all the others on your body, that outlier deserves closer attention — even if it doesn't clearly fail the ABCDE test.
Common mistake: Many people assume a spot must be dark or raised to be melanoma. Amelanotic melanoma is a rare but dangerous form that appears pink, red, or skin-colored, making it easy to dismiss as a pimple or scar.
For visual comparisons and early-stage examples, the first stages of skin cancer pictures guide provides helpful reference images.
No — most skin spots that change color are not cancerous. Color changes in skin spots are common and can result from sun exposure, hormonal shifts, aging, or minor trauma. That said, color change in a spot is one of the key warning signals that warrants professional review.
Benign reasons a spot might change color:
When color change becomes a red flag:
"A single color change in isolation is rarely alarming. It's the combination of changes — color plus shape plus rapid timeline — that raises clinical concern." — general dermatology consensus
If you're unsure whether a spot qualifies as suspicious, reviewing resources on age spots vs. cancer spots can help clarify the distinction between harmless pigmentation and potentially malignant changes.
Certain people face a significantly higher risk of developing skin cancer spots. Risk is not limited to fair-skinned individuals — though UV sensitivity does play a major role.
Higher-risk groups include:

Edge case: Organ transplant recipients face a dramatically elevated risk of squamous cell carcinoma specifically — studies have estimated their SCC risk to be 65–250 times higher than the general population, due to long-term immunosuppressive medications.
Yes — people with darker skin tones absolutely develop skin cancer spots, and they are often diagnosed at a later, more dangerous stage. The misconception that dark skin provides full protection from skin cancer contributes to delayed diagnosis and worse outcomes.
Melanin does provide some natural UV protection, but it does not eliminate risk. In people with darker skin tones:
The key takeaway: skin cancer screening is important for everyone, regardless of skin tone. Anyone who notices a new, unusual, or changing spot should seek evaluation — not assume it's harmless based on skin color alone.
Early-stage skin cancer spots often cause no pain and can be easy to overlook. The earliest warning signs are almost entirely visual, which is why regular skin self-exams matter.
Early warning signs to watch for:
One common question is whether skin cancer hurts. Early-stage lesions are usually painless — which is part of what makes them easy to ignore. The detailed breakdown of whether skin cancer hurts explains when and why pain may or may not be present at different stages.
Self-skin checks are valuable, but they're frequently done incorrectly — or not done at all. The most common errors reduce the chance of catching a suspicious spot early.
Mistake 1: Checking only sun-exposed areas
Melanoma can develop on the scalp, between the toes, under the nails, on the genitals, and on the soles of the feet. A thorough check requires a full-body examination, ideally with a hand mirror and a well-lit room.
Mistake 2: Checking infrequently
Monthly self-exams are the standard recommendation. Checking once a year — or only when something already looks alarming — misses the window for early detection.
Mistake 3: Not tracking changes over time
A single snapshot of a mole tells you little. What matters is whether it looks different from last month. Taking photos of existing spots and comparing them over time is one of the most practical tracking methods.
Mistake 4: Dismissing spots in hard-to-see areas
The back, back of the scalp, and posterior legs are commonly missed. A partner or friend can help examine these areas.
Mistake 5: Assuming a spot is benign because it doesn't hurt
As noted above, most early skin cancers are painless. Pain is not a reliable indicator of whether a spot is dangerous.
Mistake 6: Waiting too long to seek evaluation
A suspicious spot should be assessed within 2–4 weeks of discovery. Waiting months — or hoping it resolves on its own — allows potential malignancy to progress.
Melanoma is the most serious and potentially life-threatening form of skin cancer. While it accounts for a smaller percentage of skin cancer diagnoses than basal cell or squamous cell carcinoma, it is responsible for the majority of skin cancer deaths because of its tendency to spread (metastasize) to other organs.
Quick comparison of the three main types:
TypeSeriousnessSpread Risk5-Year Survival (localized)Basal Cell CarcinomaLow–ModerateRarely spreadsVery high (near 100% if caught early)Squamous Cell CarcinomaModerateCan spread to lymph nodesHigh if caught earlyMelanomaHighSpreads readily if not caught earlyHigh if localized; drops sharply if metastatic
For a complete breakdown of all four main skin cancer types — including Merkel cell carcinoma — the guide to the 4 main types of skin cancer covers each in detail.
Finding a suspicious spot doesn't mean it's cancer — but it does mean action is needed. The right steps depend on how concerning the spot looks and how quickly it appeared.
Step-by-step response:
Choose a specialist if: The spot is rapidly changing, bleeding, or you have a personal or family history of melanoma. A general practitioner can refer you, but a dermatologist or surgical clinic with skin cancer expertise will provide the most thorough evaluation.
The Minor Surgery Center's skin cancer clinic locations across Toronto, Mississauga, Vaughan, and Oakville offer screening and biopsy services for patients who need prompt evaluation.
Skin cancer screening costs vary depending on location, provider type, and whether a biopsy is required. In Ontario, a basic skin examination by a physician may be covered under OHIP in some circumstances, but dedicated skin cancer screening clinics often operate on a private-pay model.
Estimated costs in Ontario (2026):
Important note: OHIP coverage for skin cancer-related procedures depends on whether the visit is deemed medically necessary. Cosmetic mole removal is not covered; biopsy of a clinically suspicious lesion typically is. Always confirm coverage before your appointment.
For those in the Mississauga area, the skin cancer screening options in Mississauga page outlines available services and what to expect at your first visit.

For most adults with no significant risk factors, an annual full-body skin examination is a reasonable standard. Higher-risk individuals may need more frequent checks — every 3 to 6 months in some cases.
Recommended frequency by risk level:
Between professional checks, monthly self-exams are recommended by most dermatological organizations. The combination of regular self-checks and annual professional exams provides the best chance of catching changes early.
For those in the Toronto area looking for screening options, the guide to skin cancer screening in Toronto lists vetted clinics and what each offers.
Treatment for skin cancer spots depends on the type of cancer, its stage, size, location, and the patient's overall health. Most early-stage skin cancers are treated successfully with outpatient procedures.
Common treatment options:
The skin cancer surgeries and lesion treatment overview at The Minor Surgery Center explains the procedural options available for patients in Ontario.
Skin cancer prevention is genuinely possible — and the evidence strongly supports several practical strategies. No approach eliminates risk entirely, but consistent habits meaningfully reduce the chance of developing skin cancer spots.
Evidence-backed prevention strategies:
Who benefits most from prevention: Prevention is most impactful for fair-skinned individuals with high UV exposure histories, but it benefits everyone. Starting sun protection habits in childhood and adolescence provides the greatest long-term benefit, since cumulative UV damage begins early.
Q: Can a skin cancer spot appear overnight?
A: No. Skin cancer spots develop over weeks, months, or years. A lesion that appears to "appear overnight" is more likely a blood blister, cyst, or inflamed mole. That said, any rapidly changing spot should be evaluated promptly.
Q: Is a bleeding mole always skin cancer?
A: Not always — moles can bleed from minor trauma like catching on clothing. However, a mole that bleeds spontaneously or repeatedly without injury is a red flag that warrants same-week evaluation by a doctor.
Q: Can children get skin cancer spots?
A: Skin cancer in children is rare but not impossible. Certain genetic conditions increase risk. More importantly, UV damage from childhood sunburns accumulates and significantly raises adult skin cancer risk — making sun protection in childhood critically important.
Q: Do skin cancer spots always need to be removed?
A: Most confirmed skin cancers do require removal or treatment. The method depends on the type and stage. Some very superficial lesions may be treated with topical creams rather than surgery.
Q: What does a skin cancer spot feel like?
A: Most early skin cancer spots are painless and have no distinct texture from the outside. Some may feel slightly raised, rough, or firm. Itching or tenderness can occur but is not a reliable indicator on its own.
Q: How long does it take for a biopsy result to come back?
A: Most skin biopsy pathology results return within 5–10 business days, though some clinics may have results in 3–5 days. Your doctor will contact you with results and next steps.
Q: Are skin cancer spots contagious?
A: No. Skin cancer is not contagious and cannot be transmitted from person to person. Some skin cancers are associated with viruses (like HPV-related SCC), but the cancer itself is not transmissible.
Q: What's the difference between a skin cancer spot and an age spot?
A: Age spots (solar lentigines) are flat, evenly pigmented brown spots caused by sun exposure. They have smooth, well-defined borders and don't change rapidly. Cancerous spots typically have irregular borders, multiple colors, or change over time. When in doubt, have a dermatologist evaluate any new or changing pigmented lesion.
Q: Can stress cause skin cancer spots?
A: Stress does not directly cause skin cancer. However, chronic stress may suppress immune function, which could theoretically affect the body's ability to identify and destroy abnormal cells. This link is not well-established in clinical evidence.
Q: Is skin cancer more common in certain parts of the body?
A: Yes. Sun-exposed areas — the face, neck, scalp, ears, forearms, and hands — account for the majority of skin cancer cases. However, melanoma can occur anywhere, including the back, legs, and non-sun-exposed areas.
Q: What should I bring to a skin cancer screening appointment?
A: Bring a list of any spots you've noticed or are concerned about, photos if you've been tracking changes, your personal and family medical history, and a list of any medications you take (some increase photosensitivity).
Q: Can sunscreen fully prevent skin cancer?
A: Sunscreen significantly reduces UV-related skin damage and lowers skin cancer risk, but it does not provide 100% protection. Regular application, protective clothing, shade-seeking behavior, and avoiding tanning beds together offer the most comprehensive protection.
Skin cancer spots are among the most detectable and treatable forms of cancer — but only when caught early. The difference between a routine removal and a complex, life-altering diagnosis often comes down to how quickly a suspicious spot is noticed and acted on.
Actionable next steps:
For residents in Ontario, The Minor Surgery Center offers skin cancer screening, biopsy, and surgical removal services at multiple clinic locations across Toronto, Mississauga, Vaughan, Oakville, and surrounding areas. Their board-certified surgeons specialize in skin lesions and can provide prompt evaluation for suspicious spots.
Early action is the single most powerful tool available. A 15-minute skin check today could make a significant difference tomorrow.



