Last updated: June 24, 2026
Skin cancer on the nose is the most common form of facial skin cancer, primarily because the nose receives more cumulative UV radiation than almost any other part of the face. Basal cell carcinoma accounts for roughly 80 to 90 percent of nasal skin cancers, and when caught early, it is highly treatable with cure rates approaching 99 percent using Mohs micrographic surgery [1]. Early recognition of warning signs and prompt evaluation by a dermatologist or skin cancer specialist are the most critical steps toward a good outcome.
Skin cancer on the nose can appear in several distinct ways depending on the type, and it often looks like a spot that simply will not go away. The most important visual clue is persistence: a sore, bump, or patch that does not heal within three to four weeks should be evaluated.
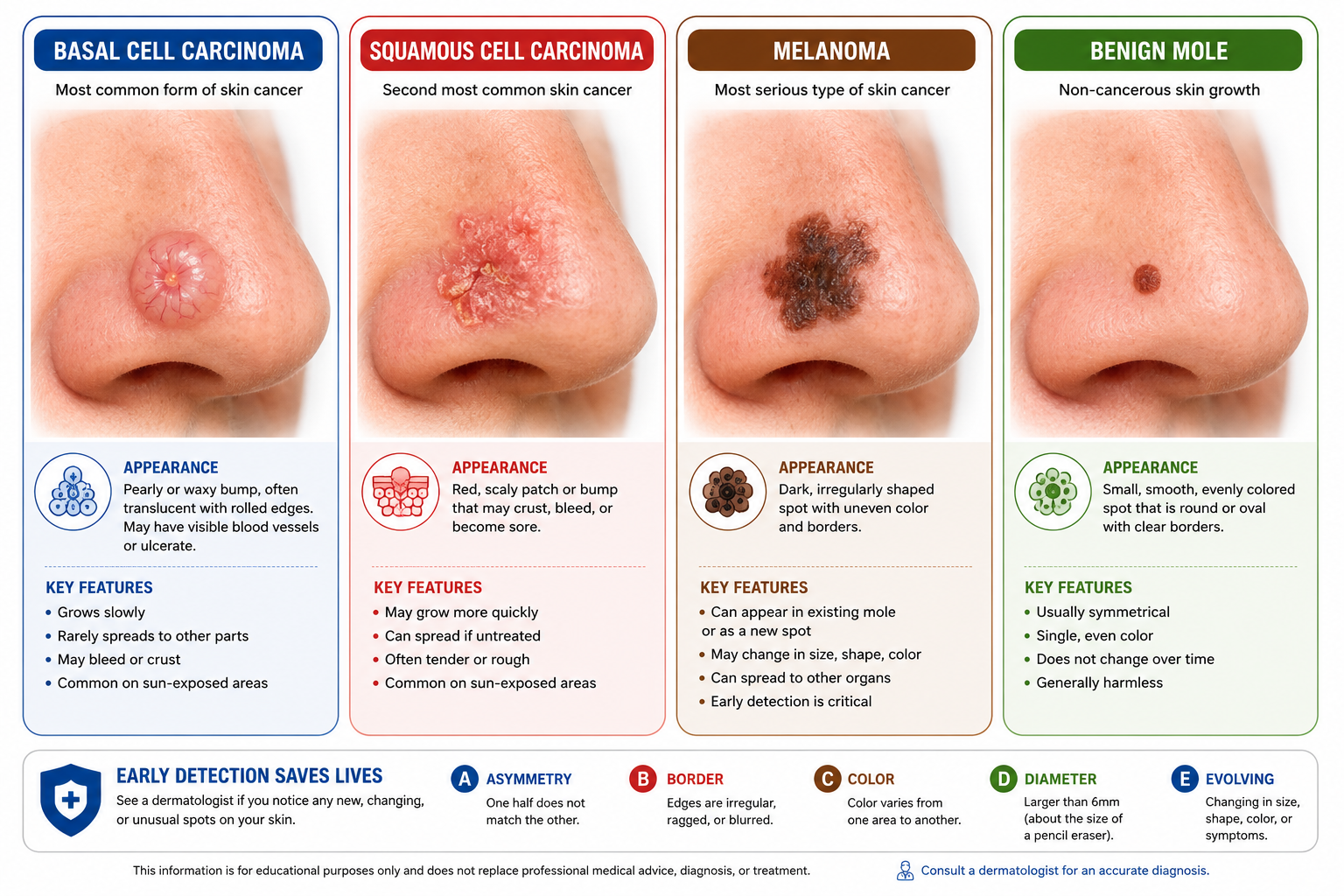
Basal cell carcinoma (BCC) is the most common type and typically appears as:
Squamous cell carcinoma (SCC) on the nose often looks like:
Melanoma on the nose is less common but the most dangerous. It may appear as:
For a visual reference on early presentations, see this guide to first stages of skin cancer pictures.
"Any spot on the nose that bleeds spontaneously, refuses to heal, or changes noticeably over four to eight weeks is a red flag that warrants professional evaluation." [2]
Most spots on the nose are benign, but certain features distinguish a concerning lesion from a harmless one. The ABCDE rule, originally developed for melanoma screening, applies broadly to any suspicious nose growth.
ABCDE warning signs:
Benign moles tend to be:
Key decision rule: Choose to see a dermatologist if a spot on the nose is new and growing, bleeds without trauma, or has been present for more than four weeks without healing. A benign mole that has been stable for years and shows none of the ABCDE features is far less urgent, but any doubt warrants professional assessment.
For more on distinguishing benign from suspicious growths, read benign mole explained.
Skin cancer on the nose is caused primarily by cumulative ultraviolet (UV) radiation damage to skin cells, and the nose's anatomy makes it uniquely vulnerable. Because the nose protrudes from the face, it intercepts UV rays at a more direct angle than surrounding skin, accumulating more damage over a lifetime [5].
Primary causes and risk factors:
Risk FactorDetailsUV radiationThe leading cause; both UVA and UVB damage DNA in skin cellsFair skinLess melanin means less natural UV protectionHistory of sunburnsEven one severe blistering sunburn in childhood raises lifetime riskOutdoor occupationFarmers, construction workers, and athletes face higher cumulative exposurePrevious skin cancerHaving one nasal or facial skin cancer raises the risk of a secondAgeMost cases occur in people over 50, though rates in younger adults are risingImmunosuppressionOrgan transplant recipients and those on immunosuppressive drugs face significantly higher riskIndoor tanningTanning beds emit concentrated UV radiation that damages nasal skinArsenic exposureA less common but established environmental risk factorGenetic syndromesGorlin syndrome (basal cell nevus syndrome) predisposes individuals to multiple BCCs
Common mistake: Many people assume that skin cancer only develops from intentional sun exposure like sunbathing. In reality, cumulative incidental exposure, driving, walking, and working near windows, accounts for a significant portion of total UV damage to the nose [5].
Yes, melanoma can and does develop on the nose, and it is the type of skin cancer on the nose that carries the highest risk of spreading to other parts of the body. While melanoma is less common on the nose than BCC or SCC, it should never be dismissed [1].
Melanoma on the nose may arise from an existing mole or appear as an entirely new dark lesion. It can also appear as a lightly pigmented or even pink growth (known as amelanotic melanoma), which makes it harder to identify visually.
Who is at highest risk for nasal melanoma:
For detailed information on melanoma diagnosis and surgical options, see melanoma surgery and treatment in Toronto.
Nose skin cancer is diagnosed through a combination of visual examination and skin biopsy. No amount of visual inspection alone can confirm a cancer diagnosis; a tissue sample examined under a microscope is required [2].
Diagnostic steps:
Edge case: Some BCCs on the nose are superficial and easy to identify, while others are morpheaform (scar-like) and can be deceptively subtle, spreading under the skin surface without an obvious raised border. These aggressive subtypes are more likely to be underestimated and undertreated if not properly biopsied.
For skin biopsy and screening options in the Greater Toronto Area, see best skin biopsy and skin cancer screening in Mississauga.
Skin cancer on the nose is generally considered higher risk than cancer on the trunk or limbs, for several reasons. The nose has complex anatomy with cartilage, bone, and critical structures for breathing and appearance, all of which can be affected if cancer grows unchecked [3].
Why nasal location increases complexity:
That said, nasal skin cancer caught at an early stage, before it invades deeper structures, carries an excellent prognosis. The key variable is timing of treatment.
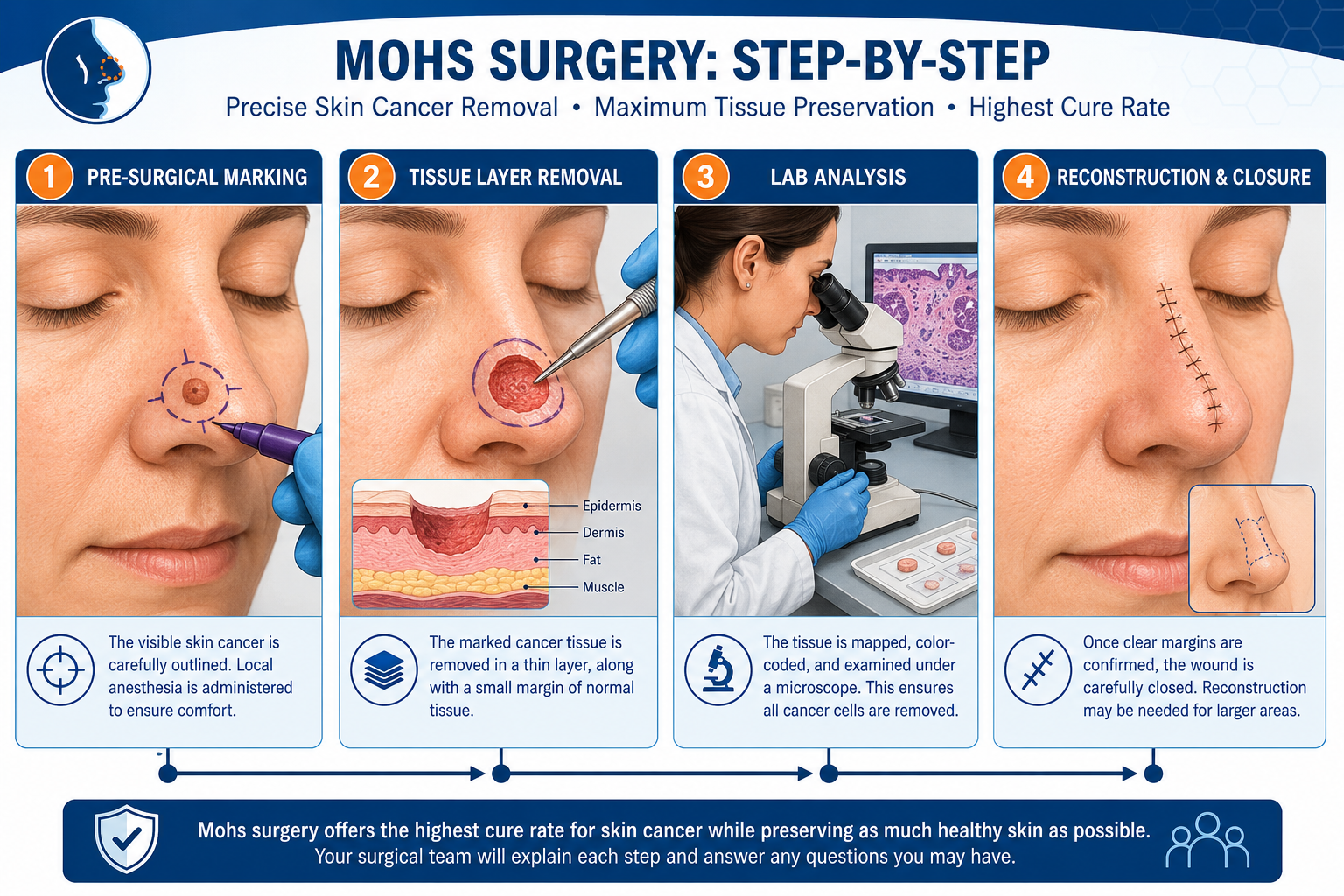
Mohs micrographic surgery is the gold-standard treatment for basal cell carcinoma on the nose, offering the highest cure rate while preserving the maximum amount of healthy tissue [3]. Other treatments exist but are generally reserved for specific situations.
Treatment options compared:
TreatmentBest ForCure Rate (BCC)NotesMohs micrographic surgeryNose, face, high-risk sitesUp to 99% [3]Gold standard; tissue-sparingStandard surgical excisionLower-risk, small lesions90-95%May require wider marginsRadiation therapyPatients who cannot have surgery85-90%Used when surgery is not feasibleTopical therapy (imiquimod, 5-FU)Superficial BCC onlyModerateNot appropriate for nodular or deep BCCCryotherapyVery superficial, low-risk lesionsVariableNot recommended for nasal tip or high-risk zonesHedgehog pathway inhibitors (vismodegib)Advanced or metastatic BCCPalliativeSystemic medication for inoperable cases
For SCC on the nose: Mohs surgery is also preferred for high-risk SCC. For more on squamous cell carcinoma treatment, see squamous cell carcinoma surgery in Toronto.
Decision rule: Choose Mohs surgery for any nasal skin cancer that is larger than 1 cm, located on the nasal tip or alar groove, recurrent, or of an aggressive histological subtype (morpheaform, infiltrative, or poorly differentiated).
Recovery from nose skin cancer surgery varies depending on the extent of the tumor and the type of reconstruction required. Most patients can return to light daily activities within one to two weeks, but full cosmetic recovery takes considerably longer [4].
General recovery timeline:
Factors that extend recovery:
Common mistake: Patients often expect the nose to look fully normal within weeks. In reality, post-surgical swelling and scar maturation are slow processes, and patience is essential for accurate assessment of the final result.
The cost of nose skin cancer removal varies widely based on the treatment type, geographic location, facility, and whether reconstruction is needed. In Canada, medically necessary skin cancer removal is generally covered by provincial health insurance (OHIP in Ontario), though wait times and specific coverage details vary.
Estimated cost ranges (private/uninsured, approximate):
Important note: These are estimates based on general market data and should not be treated as quotes. Actual costs depend on individual clinical circumstances, the number of Mohs stages required, and the complexity of reconstruction. Always confirm coverage with your provincial health plan and the treating clinic.
For patients in the Toronto area seeking accessible skin cancer care, the skin cancer clinic in Toronto with rapid access and no referral needed is one option worth exploring.
Yes, skin cancer on the nose can recur after treatment, and the risk depends heavily on whether surgical margins were clear at the time of removal. When margins are clear, recurrence rates drop to approximately 6 percent; when margins are positive (cancer cells remain at the edge), recurrence rises to around 24 percent [1].
Factors that increase recurrence risk:
Surveillance after treatment:
For more on recurrence risk and cancer progression, see this complete guide to understanding cancer progression.
Untreated skin cancer on the nose does not resolve on its own and will grow over time, often with serious consequences. The progression differs by cancer type, but none of the three main types should be left without treatment.
Consequences by type:
The bottom line: early-stage nasal skin cancer is highly curable. Delayed treatment converts a straightforward procedure into a complex surgical and reconstructive challenge.
See a dermatologist or skin cancer specialist promptly if any spot on the nose meets one or more of the following criteria. Waiting to see if it resolves on its own is appropriate only for spots that are clearly minor (a small pimple or insect bite), not for anything that persists beyond three to four weeks.
See a doctor if the spot:
Who should be seen sooner rather than later:
For those in the Toronto region, finding a skin cancer clinic near you can help reduce delays in diagnosis.
Preventing skin cancer on the nose is achievable through consistent, practical sun protection habits. Because the nose cannot be covered by clothing, it requires specific attention [5].
Evidence-based prevention strategies:
Who benefits most from aggressive prevention: People with Fitzpatrick skin types I and II (very fair, burns easily) and those with a prior skin cancer diagnosis should treat sun protection as a non-negotiable daily habit, not an occasional precaution.
Q: Can skin cancer on the nose be mistaken for acne or rosacea?
Yes. Basal cell carcinoma on the nose is frequently mistaken for a pimple, cyst, or rosacea flare because it can appear as a pink or red bump. The key difference is persistence: acne and rosacea lesions change and resolve, while BCC stays and grows.
Q: How long does Mohs surgery on the nose take?
Mohs surgery for nasal skin cancer typically takes three to six hours, though it can be longer if multiple stages are needed to achieve clear margins. The procedure is done under local anesthetic in an outpatient setting.
Q: Is nasal skin cancer more common in men or women?
BCC and SCC are more common in men, largely due to historically higher rates of outdoor occupational UV exposure. Melanoma rates are more balanced between sexes, though men tend to be diagnosed at later stages.
Q: Can a spot on the nose be skin cancer if it does not hurt?
Yes. Most early-stage skin cancers on the nose are painless. Pain, if it occurs, is usually a sign of more advanced disease involving nerves or deeper structures. The absence of pain should never be used to rule out skin cancer.
Q: What type of doctor removes skin cancer from the nose?
Mohs surgeons (dermatologists with specialized fellowship training), plastic surgeons, and head and neck surgeons all treat nasal skin cancer. For complex cases requiring reconstruction, a plastic and reconstructive surgeon is often involved.
Q: Does skin cancer on the nose always require surgery?
Not always. Superficial BCC may be treated with topical therapies or radiation in select patients. However, surgery (particularly Mohs) is the standard of care for most nasal skin cancers because it provides the highest cure rate and best tissue preservation.
Q: How soon after diagnosis should treatment begin?
For BCC and SCC, treatment within four to eight weeks of diagnosis is generally recommended. Melanoma should be treated as soon as possible, ideally within two to four weeks, due to its higher metastatic potential.
Q: Can children get skin cancer on the nose?
Skin cancer in children is rare but not impossible, particularly in those with genetic conditions like xeroderma pigmentosum or Gorlin syndrome. Any unusual, persistent lesion on a child's nose warrants evaluation.
Q: Will there be a visible scar after nasal skin cancer removal?
Some scarring is inevitable, but skilled reconstruction minimizes cosmetic impact. Mohs surgery's tissue-sparing approach reduces the defect size, and reconstructive techniques are designed to restore both form and function. Scars continue to fade for up to 12 months [4].
Q: Is it safe to use over-the-counter treatments on a suspected nose skin cancer?
No. Over-the-counter products should not be used on a suspected skin cancer. Self-treatment delays diagnosis and can obscure the lesion, making accurate assessment harder. Always seek professional evaluation first.
Skin cancer on the nose is both common and, in most cases, highly treatable when caught early. The nose's constant UV exposure makes it the most frequent site for facial skin cancers, with basal cell carcinoma accounting for the vast majority of cases [1]. Recognizing warning signs, including persistent sores, pearly bumps, scaly patches, and bleeding lesions, and acting on them promptly is the single most important step a person can take [2].
Actionable next steps:
The difference between a simple excision and a major reconstructive surgery often comes down to how quickly a person acts on a warning sign.
[1] Skin Cancer On Nose - https://instalab.com/answers/skin-cancer-on-nose?utm_source=openai
[2] How Is Skin Cancer On The Nose Treated - https://dermgroupar.com/skin-cancer/how-is-skin-cancer-on-the-nose-treated/?utm_source=openai
[3] Mohs Surgery Nose Reconstruction - https://www.kaplanclinic.co.il/en/articles/mohs-surgery-nose-reconstruction?utm_source=openai
[4] 352 Surfer Returns To The Ocean After Near Total Nasal Reconstruction - https://my.clevelandclinic.org/patient-stories/352-surfer-returns-to-the-ocean-after-near-total-nasal-reconstruction?utm_source=openai
[5] Skin Cancer On Nose - https://www.medicalnewstoday.com/articles/skin-cancer-on-nose?utm_source=openai



