Imagine receiving a call from your doctor after a routine CT scan. "We found something on your kidney," they say. Your heart races. Is it cancer? Should you be worried? For millions of people each year, this scenario becomes reality when imaging tests reveal kidney cysts—fluid-filled sacs that appear on approximately 40% of people over age 50. Understanding Kidney (Renal) Cysts vs Kidney Cancer: When a 'Simple Cyst' Needs Follow-Up can transform anxiety into informed action, helping patients and their families navigate the critical distinction between harmless findings and potentially serious conditions requiring immediate attention.
Kidney cysts are round or oval pouches filled with fluid that develop within the kidney tissue. These structures form when the kidney's tiny filtering tubes become blocked or dilated, allowing fluid to accumulate. While the exact cause remains unclear in many cases, age appears to be the strongest risk factor.
Simple cysts represent the most benign form of kidney cysts. These structures have several defining characteristics:
Simple cysts typically cause no symptoms and require no treatment. They grow slowly over years, rarely interfering with kidney function. Medical professionals consider them a normal part of aging, similar to how skin changes occur over time. For more information about different types of cysts throughout the body, visit our comprehensive guide on 17 types of cysts.
Unlike their simple counterparts, complex cysts display features that raise concern for malignancy:
The presence of these features doesn't automatically mean cancer, but it does warrant closer evaluation and monitoring.
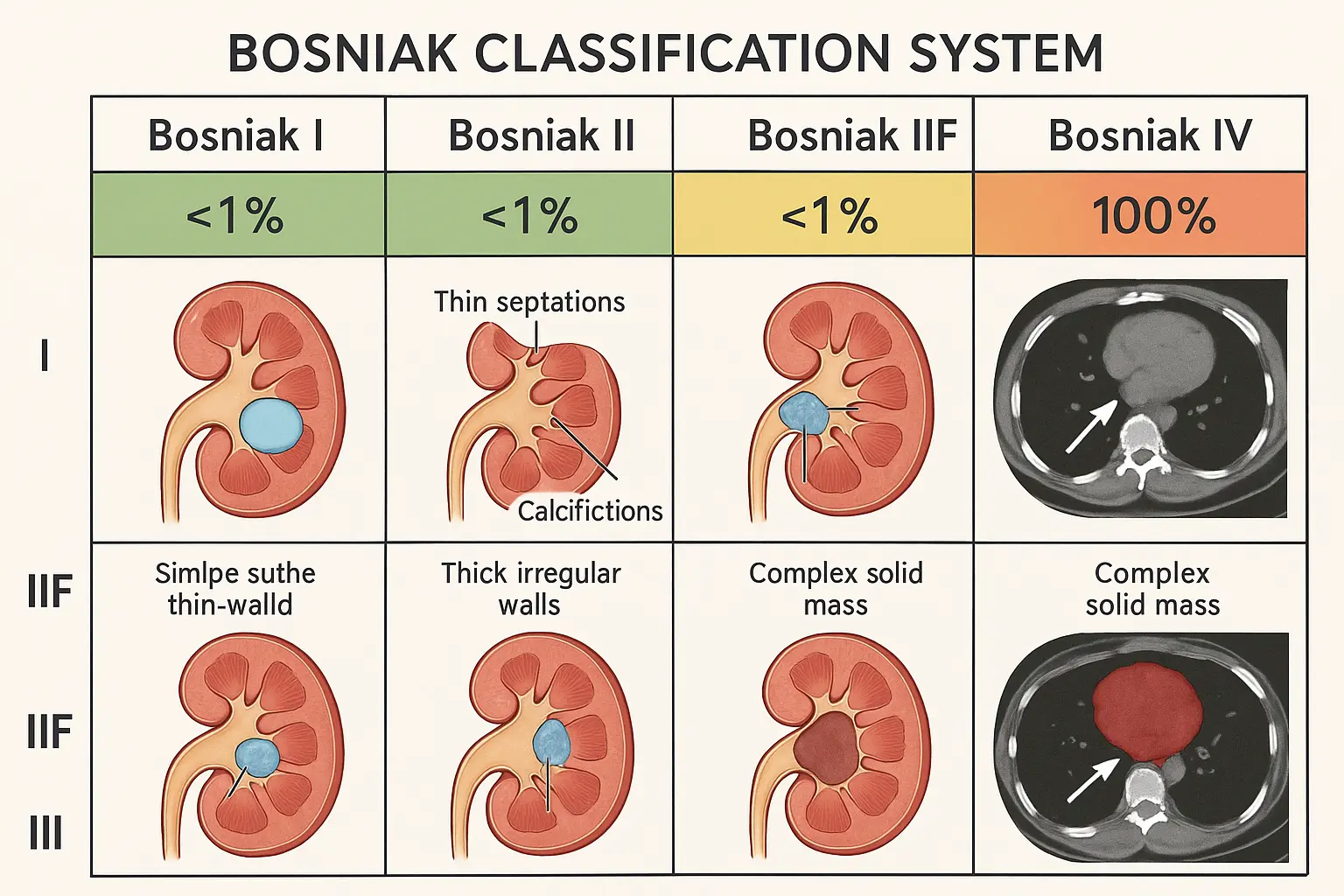
In 1986, Dr. Morton Bosniak developed a standardized system for categorizing kidney cysts based on their appearance on CT scans. This classification helps doctors assess malignancy risk and determine appropriate follow-up strategies.
Bosniak CategoryDescriptionMalignancy RiskRecommended ActionISimple cyst with thin wall, no septations, calcifications, or solid components<1%No follow-up neededIIMinimally complex with few thin septa, fine calcification, or high-density content<1%No follow-up neededIIFMore septa, minimal wall thickening, or nodular calcification5%Regular imaging follow-up every 6-12 monthsIIIThickened irregular walls, thick septa, or enhancement after contrast55%Surgical evaluation recommendedIVClearly malignant features with solid enhancing components100%Surgical removal typically required
When reviewing imaging reports, patients often encounter confusing medical terminology. Here's what key terms mean:
Septations: Internal walls dividing the cyst into compartments. Thin septa (like tissue paper) are less concerning than thick septa (like cardboard).
Calcification: Calcium deposits that appear bright white on CT scans. Fine, peripheral calcification is less worrisome than thick, nodular calcification.
Enhancement: When contrast dye is injected during CT or MRI, areas with blood supply "light up" or enhance. Simple cysts don't enhance; cancerous tissue typically does.
Hounsfield units (HU): A measurement of density on CT scans. Simple cysts measure 0-20 HU (water density), while higher numbers suggest more complex content.
Approximately 90% of all kidney cancers are renal cell carcinomas (RCC), which originate in the kidney's filtering tubes. Understanding how these tumors differ from benign cysts is crucial for early detection and treatment.
Clear Cell RCC (70-75% of cases):
Papillary RCC (10-15% of cases):
Chromophobe RCC (5% of cases):
Other rare types include collecting duct carcinoma and medullary carcinoma, which together account for less than 5% of cases.
The fundamental difference between kidney cysts and cancer lies in their growth patterns and cellular behavior:
🔬 Cysts:
🔬 Cancer:
Determining when a kidney finding requires ongoing monitoring versus reassurance involves careful evaluation of multiple factors. Understanding these decision points empowers patients to advocate for appropriate care.
Certain imaging features or symptoms demand urgent evaluation:
⚠️ Imaging Red Flags:
⚠️ Symptom Red Flags:
Even cysts initially classified as Bosniak I or II may require follow-up in certain circumstances:
Size matters: Cysts larger than 4cm may cause symptoms through compression of surrounding structures, including:
Symptom development: Any new symptoms potentially related to a previously asymptomatic cyst warrant re-evaluation.
Growth rate: While simple cysts can grow, rapid enlargement (>0.5cm per year) may indicate the need for reclassification.
Patient risk factors: Individuals with genetic conditions like Von Hippel-Lindau disease or tuberous sclerosis require more aggressive monitoring regardless of cyst appearance.
Most kidney cysts and early kidney cancers produce no symptoms whatsoever. This silent nature explains why approximately 60% of kidney tumors are discovered incidentally during imaging performed for unrelated reasons.
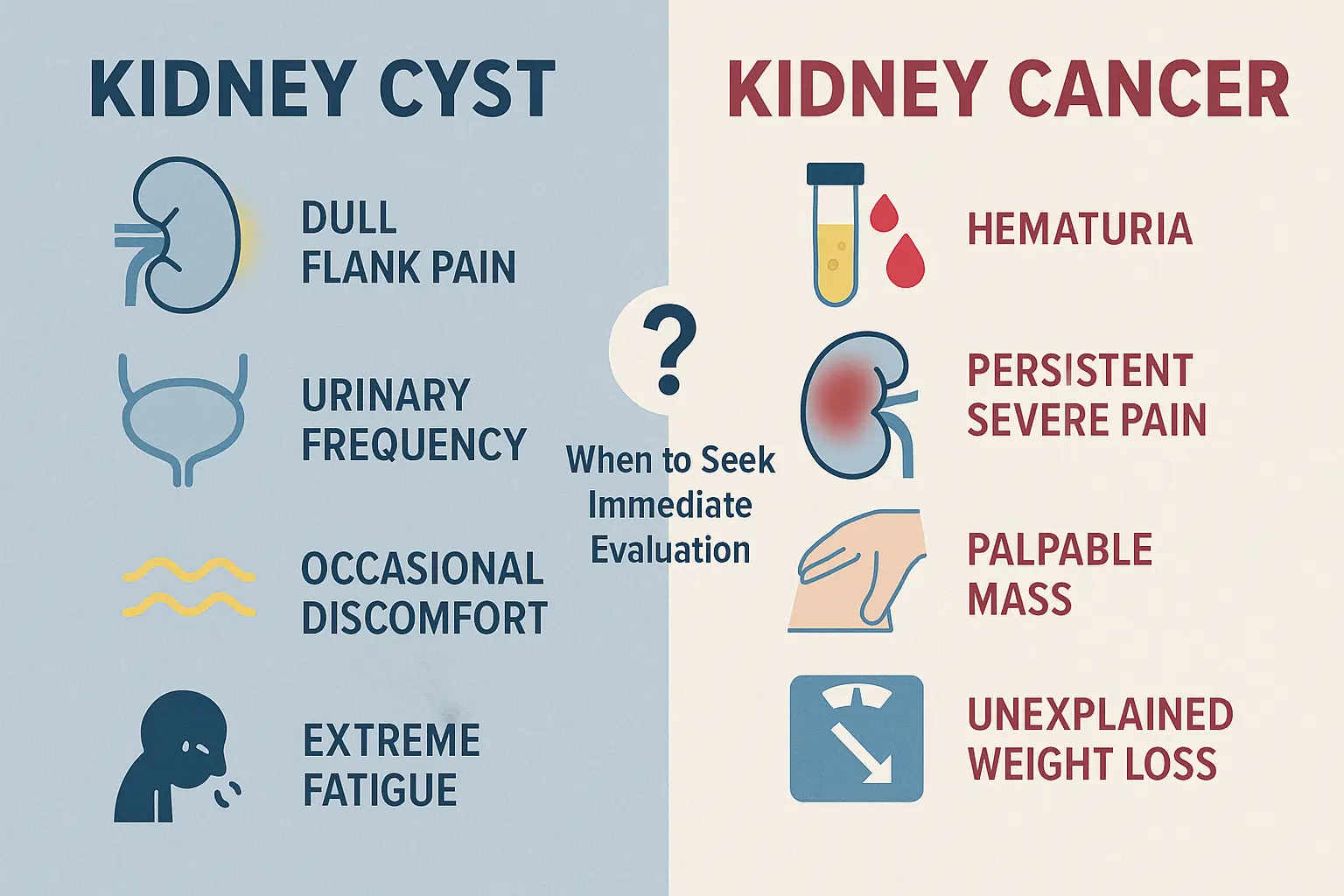
When simple cysts do cause symptoms, they typically include:
💧 Dull, aching pain in the flank (side) or upper abdomen
💧 Urinary changes:
💧 Infection (if cyst becomes infected):
Kidney cancer symptoms often appear only in advanced stages. The classic triad (occurring together in less than 10% of cases) includes:
🚨 Hematuria (blood in urine):
🚨 Flank pain:
🚨 Palpable mass:
Advanced kidney cancer may produce symptoms throughout the body:
Similar to how understanding skin cancer symptoms helps with early detection, recognizing kidney-related warning signs can be lifesaving.
Modern imaging technology allows precise characterization of kidney lesions, distinguishing benign from malignant with increasing accuracy.
Renal ultrasound often serves as the initial imaging modality:
✅ Advantages:
❌ Limitations:
Ultrasound excels at confirming simple cysts but often requires follow-up with CT or MRI for complex lesions.
Contrast-enhanced CT remains the preferred imaging for characterizing kidney masses:
✅ Advantages:
❌ Limitations:
Protocol matters: A dedicated renal mass CT protocol includes images before and after contrast administration, allowing assessment of enhancement—the key feature distinguishing solid tumors from cysts.
Magnetic resonance imaging serves as an excellent alternative or adjunct to CT:
✅ Advantages:
❌ Limitations:
When reviewing reports, look for these key descriptors:
"Homogeneous": Uniform appearance throughout—reassuring for simple cysts
"Heterogeneous": Mixed appearance—raises concern for complexity
"Enhancing": Shows increased brightness after contrast—concerning for solid tissue
"Non-enhancing": No change with contrast—reassuring for simple cyst
"Septated": Contains internal walls—degree of concern depends on septa thickness
The appropriate follow-up strategy depends entirely on the Bosniak classification and individual patient factors.
No follow-up imaging required for these categories. Patients can be reassured that:
The "F" stands for "follow-up," indicating these lesions require monitoring:
Recommended protocol:
What to watch for:
Approximately 5% of Bosniak IIF lesions will progress to higher categories requiring intervention.
These indeterminate lesions require urologic evaluation:
Management options:
These lesions are presumed malignant and typically require:
Treatment strategies for kidney lesions span a spectrum from watchful waiting to aggressive surgical intervention.
Observation remains appropriate for:
Symptom management for large cysts:
Partial nephrectomy (kidney-sparing surgery):
Radical nephrectomy (complete kidney removal):
Ablative therapies:
Outcomes for kidney cancer vary dramatically by stage:
📊 5-Year Survival Rates:
These statistics underscore the importance of early detection and appropriate follow-up of suspicious kidney lesions.
While many kidney cysts develop without identifiable cause, certain factors increase risk for both cysts and kidney cancer.
🔸 Age: Risk increases significantly after age 50 🔸 Male gender: Men develop cysts more frequently than women 🔸 Chronic kidney disease: Damaged kidneys develop more cysts 🔸 Dialysis: Long-term dialysis patients have very high cyst prevalence 🔸 Genetic conditions: Polycystic kidney disease, Von Hippel-Lindau disease
🔸 Smoking: Doubles the risk of kidney cancer 🔸 Obesity: Increases risk by 20-30% 🔸 Hypertension: Elevated blood pressure increases risk 🔸 Family history: First-degree relative with kidney cancer 🔸 Occupational exposures: Asbestos, cadmium, organic solvents 🔸 Genetic syndromes: Von Hippel-Lindau, hereditary papillary RCC 🔸 Chronic kidney disease: Particularly dialysis patients
While not all kidney cancers are preventable, risk reduction strategies include:
✅ Smoking cessation: Single most important modifiable risk factor ✅ Weight management: Maintaining healthy BMI ✅ Blood pressure control: Managing hypertension ✅ Occupational safety: Minimizing exposure to carcinogens ✅ Healthy diet: Fruits, vegetables, limited processed foods ✅ Regular exercise: At least 150 minutes weekly of moderate activity
Just as building a skin-healthy lifestyle reduces cancer risk, kidney-healthy habits promote overall urologic wellness.
Knowing when to seek specialist evaluation can be lifesaving. Consider urology consultation for:
🚨 Visible blood in urine (hematuria) 🚨 Palpable abdominal or flank mass 🚨 Bosniak III or IV lesion on imaging 🚨 Unexplained weight loss with kidney mass 🚨 Rapidly growing kidney lesion
📋 Bosniak IIF lesion requiring surveillance 📋 Symptomatic simple cyst causing pain 📋 Microscopic hematuria with kidney lesion 📋 Family history of kidney cancer with new lesion 📋 Patient preference for specialist opinion
Prepare for your consultation by asking:
For the vast majority of people diagnosed with simple kidney cysts, life continues completely unchanged. Understanding this can alleviate significant anxiety.
For Bosniak I and II cysts:
For Bosniak IIF cysts under surveillance:
The period between discovering a complex cyst and determining its nature can be stressful. Helpful strategies include:
💚 Education: Understanding your specific situation reduces fear 💚 Support: Connecting with others who've faced similar diagnoses 💚 Communication: Maintaining open dialogue with your healthcare team 💚 Perspective: Remembering that most kidney lesions are benign 💚 Action: Focusing on controllable factors like healthy lifestyle choices
Certain groups require modified approaches to kidney cyst evaluation and management.
Von Hippel-Lindau (VHL) disease:
Hereditary papillary renal cell carcinoma:
Birt-Hogg-Dubé syndrome:
Children with kidney cysts require different evaluation:
Kidney cysts discovered during pregnancy:
Emerging technologies promise improved characterization of kidney lesions.
Contrast-enhanced ultrasound (CEUS):
Dual-energy CT:
Multiparametric MRI:
Research is exploring blood and urine tests that might:
Machine learning algorithms are being developed to:
Understanding Kidney (Renal) Cysts vs Kidney Cancer: When a 'Simple Cyst' Needs Follow-Up empowers patients to participate actively in their healthcare decisions. The key principles to remember:
Simple cysts are common and benign: Finding a simple cyst on imaging is not a cause for alarm. These fluid-filled sacs affect nearly half of people over 50 and carry essentially no cancer risk.
The Bosniak system provides a roadmap: This classification translates complex imaging findings into actionable risk categories, guiding appropriate follow-up from reassurance to surgical intervention.
Most kidney cancers are caught early: The widespread use of imaging means most renal cell carcinomas are discovered incidentally when small and highly curable.
Follow-up matters: For intermediate-risk lesions (Bosniak IIF), compliance with surveillance imaging is essential to detect any concerning changes early.
Symptoms warrant evaluation: While most kidney lesions cause no symptoms, new onset of blood in urine, flank pain, or systemic symptoms requires prompt medical attention.
For additional information about various types of cysts and their management, explore our resources at The Minor Surgery Center.
The discovery of a kidney cyst or mass on imaging can trigger significant anxiety, but understanding the distinction between benign and malignant lesions transforms fear into informed vigilance. Kidney (Renal) Cysts vs Kidney Cancer: When a 'Simple Cyst' Needs Follow-Up represents more than a medical question—it's about empowering patients with the knowledge to advocate for appropriate care.
✅ If you have a simple cyst (Bosniak I or II): Breathe easy. No follow-up is needed. Continue regular health maintenance.
✅ If you have a Bosniak IIF lesion: Mark your calendar for follow-up imaging. Compliance with surveillance is your best protection.
✅ If you have a Bosniak III or IV lesion: Schedule a urology consultation promptly. Early evaluation expands treatment options.
✅ If you develop symptoms: Don't wait. Blood in urine, persistent pain, or unexplained weight loss warrant immediate medical evaluation.
✅ If you have risk factors: Discuss screening with your physician, especially if you have a family history of kidney cancer or genetic syndromes.
Modern imaging has revolutionized kidney lesion detection, often finding abnormalities that would have remained unknown in previous generations. While this creates moments of anxiety when cysts or masses are discovered, it also provides unprecedented opportunities for early intervention when needed. The overwhelming majority of kidney cysts are simple, benign, and require nothing more than reassurance. For the minority that require follow-up, standardized classification systems and surveillance protocols ensure appropriate care.
Knowledge truly is power when it comes to kidney health. By understanding the differences between simple cysts and complex lesions, recognizing warning signs that require evaluation, and knowing when follow-up is necessary, patients can navigate kidney findings with confidence rather than fear.
For more information about cyst management and other minor surgical procedures, visit The Minor Surgery Center blog for comprehensive, evidence-based health information.



