Last updated: February 24, 2026
Wrist pain sends millions of people searching for answers each year, and many turn to simple at-home tests found online. But here's the problem: Carpal Tunnel vs Tendonitis conditions share overlapping symptoms, and the popular wrist tests you'll find in videos and articles have surprisingly poor accuracy rates. Phalen's test, one of the most commonly recommended self-assessments, shows sensitivity ranging from just 51-91% and specificity from 33-88%, making it unreliable as a standalone diagnostic tool[4]. This wide variability means you could have carpal tunnel syndrome and test negative, or have tendonitis and test positive for carpal tunnel.

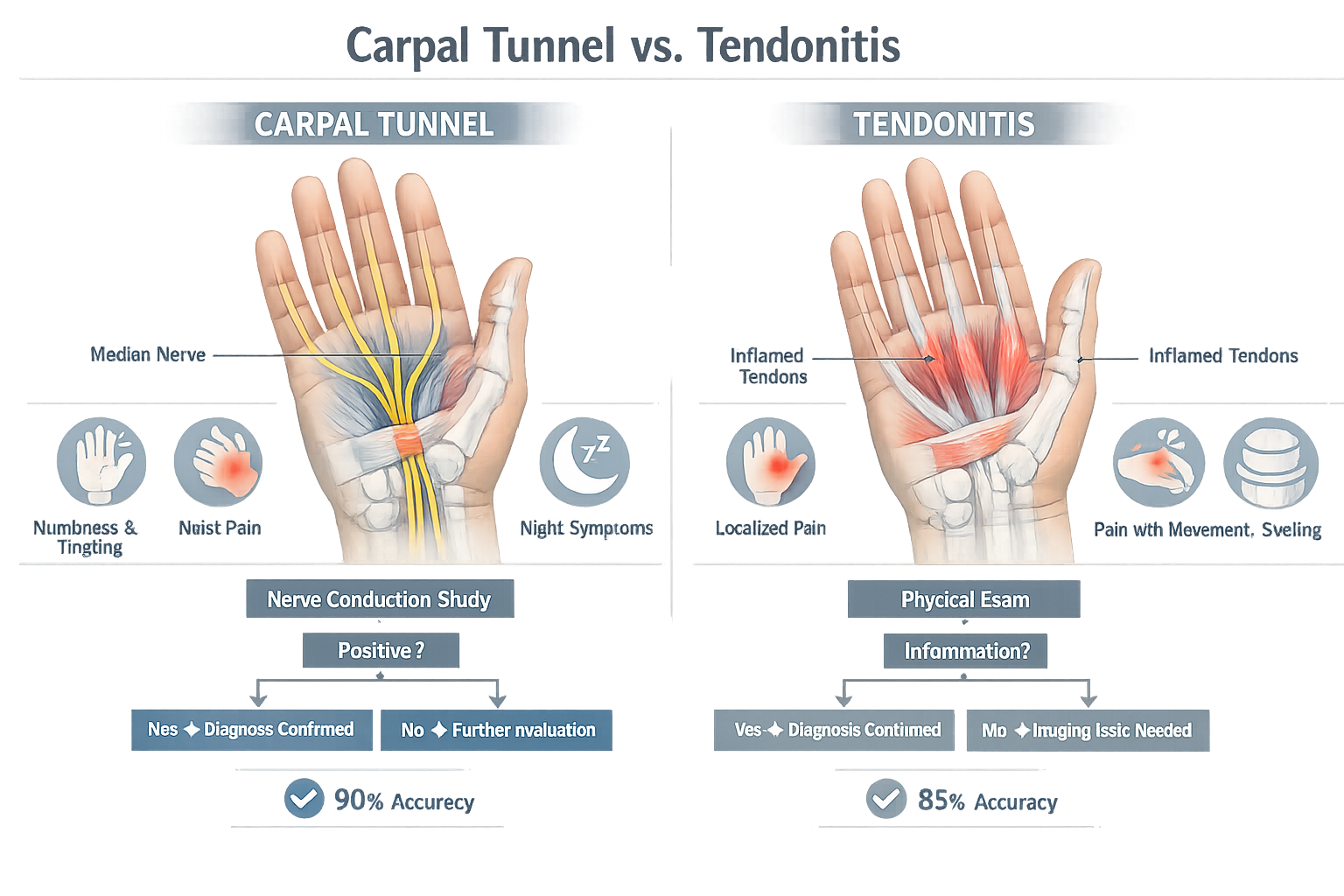
Carpal Tunnel vs Tendonitis conditions are frequently confused because both cause wrist and hand discomfort, but they affect different structures. Carpal tunnel syndrome involves compression of the median nerve as it passes through the carpal tunnel in the wrist, causing numbness, tingling, and weakness in specific fingers. Tendonitis involves inflammation of the tendons that move the wrist and fingers, causing pain that worsens with movement. Simple wrist tests like Phalen's and Tinel's can mislead because they have poor sensitivity and specificity rates, often producing false positives or false negatives. Accurate diagnosis requires professional evaluation with nerve conduction studies and comprehensive clinical assessment.
Both carpal tunnel syndrome and wrist tendonitis cause pain in the same general area and often develop from similar activities like repetitive computer work, assembly line tasks, or sports. This overlap makes self-diagnosis particularly challenging.
Carpal tunnel syndrome occurs when the median nerve becomes compressed as it travels through the narrow carpal tunnel in the wrist. This tunnel is formed by wrist bones on three sides and the transverse carpal ligament on the palm side. When tissues inside the tunnel swell or the tunnel narrows, the nerve gets squeezed, disrupting normal nerve signals.
Wrist tendonitis (also called tenosynovitis when the tendon sheath is involved) happens when the tendons that control finger and wrist movement become inflamed from overuse, injury, or repetitive strain. These tendons run through the same general wrist area but are separate structures from the median nerve.
FeatureCarpal Tunnel SyndromeWrist TendonitisAffected StructureMedian nerveFlexor or extensor tendonsPrimary SymptomNumbness, tinglingPain with movementFinger DistributionThumb, index, middle, half of ring fingerAny finger depending on affected tendonNight SymptomsOften worse at nightUsually better with restWeakness PatternThumb opposition, grip strengthPain-limited movementSwelling LocationInside carpal tunnel (not visible)May see visible swelling along tendon path
The confusion intensifies because both conditions can coexist. Someone with carpal tunnel syndrome may also develop tendonitis from compensatory movement patterns, or vice versa. This layering of conditions makes simple tests even less reliable.
People often assume they have carpal tunnel syndrome when they actually have:
Conversely, some dismiss true carpal tunnel syndrome as "just tendonitis," delaying proper treatment until nerve damage becomes permanent. For more information on distinguishing these conditions, see our comprehensive comparison of carpal tunnel, tendonitis, and arthritis.
The short answer: not very accurate at all. The most commonly recommended at-home tests for carpal tunnel syndrome have significant limitations that make them unreliable for self-diagnosis.
Phalen's test involves pressing the backs of your hands together with wrists flexed for 30-60 seconds. If you experience numbness or tingling in the median nerve distribution, the test is considered positive for carpal tunnel syndrome[3].
The reality of Phalen's test accuracy:
The wide variability in these numbers comes from differences in how long the wrist is held flexed, patient populations studied, and what constitutes a "positive" result. Some studies use 30 seconds, others use 60 seconds, and the threshold for symptom reproduction varies.
Tinel's test involves tapping over the median nerve at the wrist. A positive test produces tingling or "electric shock" sensations radiating into the fingers[5].
Tinel's test problems:
This test applies direct pressure over the carpal tunnel for 30 seconds. While it may be slightly more specific than Phalen's or Tinel's tests, it still lacks the accuracy needed for definitive diagnosis[4].
Why these tests fail:
For a detailed look at which tests actually matter, explore our guide on home tests for carpal tunnel.
While overlap exists, each condition has characteristic features that help distinguish them when you know what to look for.
Numbness and tingling are the defining symptoms of carpal tunnel syndrome. This occurs because nerve compression disrupts sensory signals from the median nerve.
Specific carpal tunnel indicators:
The nighttime worsening happens because most people sleep with bent wrists, which increases pressure inside the carpal tunnel. Learn more about carpal tunnel and sleeping positions to understand this connection.
Pain with specific movements defines tendonitis, since inflamed tendons hurt when they're used.
Tendonitis indicators:
Choose carpal tunnel as more likely if:
Choose tendonitis as more likely if:
Seek immediate professional evaluation if:
The fundamental problem with physical examination tests for Carpal Tunnel vs Tendonitis diagnosis lies in what they actually measure versus what clinicians need to know.
Physical tests like Phalen's, Tinel's, and Durkan's attempt to provoke symptoms by:
The critical limitation: these tests only tell you whether symptoms can be reproduced under specific conditions. They don't measure:
Anatomical variation plays a huge role. The carpal tunnel size, median nerve position, and tendon arrangement vary significantly between individuals. What provokes symptoms in one person may not in another with the same condition.
Symptom fluctuation means someone might test negative in the morning but positive in the evening, or vice versa. Carpal tunnel symptoms often vary with:
Technique inconsistency occurs because:
Coexisting conditions complicate interpretation. Many people with wrist pain have multiple overlapping issues:
When a test has 70% sensitivity and 70% specificity (better than many wrist tests), here's what happens in a population where 30% actually have carpal tunnel syndrome:
This means only 50% of positive tests are actually correct (21 true positives out of 42 total positives). This is why physical examination tests should only be used adjunctively, never as definitive diagnostic tools[4].
Accurate diagnosis of Carpal Tunnel vs Tendonitis requires tests that directly measure the affected structures rather than simply provoking symptoms.
Nerve Conduction Studies (NCS) and Electromyography (EMG) provide objective measurements of nerve function with 95-98% accuracy for carpal tunnel diagnosis[7].
How NCS works:
What NCS reveals:
NCS can detect carpal tunnel syndrome even before symptoms become severe, and it quantifies the degree of nerve compression (mild, moderate, or severe)[6]. This information guides treatment decisions and helps predict outcomes.
EMG testing examines the electrical activity of muscles controlled by the median nerve. It can detect:
For comprehensive information about electrodiagnostic testing, see our article on EMG testing for carpal tunnel.
High-resolution ultrasound can visualize:
Ultrasound advantages:
Ultrasound limitations:
MRI provides detailed images of soft tissues and can identify:
When MRI is recommended:
While physical tests have poor accuracy, certain validated questionnaires show better diagnostic utility[1]:
CTS-6 Questionnaire asks about:
Kamath and Stothard Questionnaire focuses on:
Katz and Stirrat Hand Symptom Diagram has patients:
These tools work better because they capture the pattern and behavior of symptoms over time rather than just a single moment of provocation.
A systematic approach to diagnosing Carpal Tunnel vs Tendonitis increases accuracy and ensures appropriate treatment.
Before seeing a healthcare provider, track:
Symptom characteristics:
Timing patterns:
Functional impact:
Medical history:
Start with your primary care physician who can:
Consider specialist referral to:
A thorough evaluation should include:
Clinical examination:
Electrodiagnostic studies:
Imaging when indicated:
Your healthcare provider should evaluate for conditions that mimic carpal tunnel or tendonitis:
For more information on distinguishing carpal tunnel from other conditions, read our guide on carpal tunnel syndrome misdiagnosis.
Don't assume one test tells the whole story. Even EMG/NCS can be normal in early or mild carpal tunnel syndrome. Diagnosis should combine clinical findings, patient history, and test results.
Don't ignore bilateral symptoms. When both hands are affected, consider systemic causes like diabetes, thyroid disease, or pregnancy rather than just local compression.
Don't dismiss symptoms that don't fit the textbook pattern. Anatomical variations mean some people have atypical symptom distributions.
Don't delay evaluation for progressive symptoms. Permanent nerve damage can occur if carpal tunnel syndrome goes untreated for too long.
Treatment for Carpal Tunnel vs Tendonitis differs significantly because the underlying problems are different.
Wrist splinting is the first-line treatment for mild to moderate carpal tunnel syndrome:
Learn about choosing the right carpal tunnel brace or splint for optimal results.
Activity modification:
Corticosteroid injections:
Oral medications:
Rest and activity modification:
Ice therapy:
Anti-inflammatory measures:
Physical therapy:
Splinting or bracing:
For specific exercises that help both conditions, see our 10-minute daily carpal tunnel exercise routine.
Carpal tunnel release surgery is recommended when:
The surgery involves cutting the transverse carpal ligament to relieve pressure on the median nerve. Success rates exceed 90% for appropriately selected patients[7].
Tendon surgery may be needed for:
Choose conservative treatment first if:
Consider surgery sooner if:
Combine treatments when:
For more information about surgical options, explore our guide on carpal tunnel surgery alternatives.
Prevention strategies differ for carpal tunnel syndrome and tendonitis, but many ergonomic principles benefit both.
Workplace ergonomics:
Work habits:
Lifestyle factors:
For comprehensive prevention strategies, read our article on carpal tunnel prevention and proven tips to keep your wrists pain-free.
Proper technique:
Conditioning:
Equipment considerations:
Some risk factors for carpal tunnel syndrome and tendonitis are beyond your control:
Genetic factors:
Demographic factors:
Medical conditions:
Understanding these non-modifiable risk factors helps you recognize when you need more aggressive prevention strategies or earlier intervention.
Misdiagnosis of Carpal Tunnel vs Tendonitis is common, and recognizing the signs of incorrect diagnosis can save months of ineffective treatment.
Treatment isn't working: If you've followed proper conservative treatment for 6-8 weeks without any improvement, the diagnosis may be incorrect. Some improvement should occur within this timeframe for most cases.
Symptoms don't match the pattern:
Bilateral symptoms with no clear cause: When both hands are affected simultaneously without obvious repetitive strain, consider systemic causes like:
Symptoms extend beyond the expected distribution:
Consider another evaluation if:
Questions to ask during second opinion:
Cervical radiculopathy (pinched nerve in the neck):
Thoracic outlet syndrome:
Pronator syndrome:
Diabetic neuropathy:
Vitamin B12 deficiency:
For a comprehensive look at conditions that mimic carpal tunnel, see our article on carpal tunnel vs other conditions.
Beyond basic physical examination and electrodiagnostic studies, advanced imaging can provide valuable diagnostic information for Carpal Tunnel vs Tendonitis cases.
Dynamic ultrasound allows real-time visualization of structures during movement:
For carpal tunnel evaluation:
For tendonitis evaluation:
Ultrasound advantages:
Ultrasound limitations:
MRI provides superior soft tissue detail and is particularly useful when:
What MRI reveals:
For carpal tunnel:
For tendonitis:
MRI drawbacks:
Standard X-rays don't show nerves or tendons but are valuable for:
Special X-ray views:
The most accurate diagnosis comes from integrating multiple data sources:
Example of integrated diagnosis:
A patient presents with wrist pain and numbness. Initial assessment suggests carpal tunnel syndrome, but:
Revised diagnosis: Primary flexor tendonitis with secondary mild carpal tunnel syndrome. Treatment focuses on tendonitis first, with carpal tunnel monitoring.
This integrated approach prevents the misdiagnosis that occurs when clinicians rely too heavily on simple wrist tests.
Yes, carpal tunnel syndrome and wrist tendonitis frequently coexist. The conditions can develop independently or one can lead to the other through compensatory movement patterns. When both are present, treatment must address each condition specifically, which is why accurate diagnosis through EMG/NCS and imaging is essential rather than relying on simple physical tests.
See a doctor within 2 weeks if wrist pain or numbness interferes with daily activities, wakes you at night, or causes weakness. Don't wait if you experience progressive symptoms, muscle wasting at the base of the thumb, or frequent dropping of objects. Early intervention prevents permanent nerve damage in carpal tunnel syndrome and chronic tendon degeneration in tendonitis.
At-home wrist tests aren't completely useless, but they shouldn't be used for self-diagnosis. They can help you recognize that a problem exists and prompt you to seek professional evaluation. However, with sensitivity as low as 51% and specificity as low as 33%, these tests miss many true cases and falsely identify many people without the condition[4].
Carpal tunnel syndrome typically worsens at night because most people sleep with bent wrists, which increases pressure inside the carpal tunnel and compresses the median nerve. Fluid redistribution during sleep also contributes to increased swelling. Tendonitis, in contrast, usually improves with rest and shouldn't wake you from sleep unless you're sleeping on the affected wrist.
Carpal tunnel syndrome rarely resolves completely without treatment, though symptoms may fluctuate. Mild cases related to temporary conditions like pregnancy may improve after delivery. However, progressive nerve compression typically worsens over time without intervention. Early conservative treatment with splinting and activity modification can prevent progression and avoid the need for surgery. For more information, read our article on can carpal tunnel go away on its own.
A positive Phalen's test means you experience numbness or tingling when your wrists are flexed for 30-60 seconds. However, this doesn't confirm carpal tunnel syndrome because the test has poor specificity (33-88%)[4]. Many people without carpal tunnel syndrome test positive, and many with confirmed carpal tunnel test negative. Actual carpal tunnel syndrome is diagnosed through EMG/NCS showing median nerve compression, combined with characteristic symptoms and clinical findings.
EMG/NCS testing has 95-98% accuracy for diagnosing carpal tunnel syndrome[7], compared to physical examination tests with accuracy rates as low as 51%. EMG/NCS directly measures nerve conduction speed and signal strength, providing objective data about nerve function. Physical tests only assess whether symptoms can be provoked, which is much less reliable for diagnosis.
Start with EMG/NCS for suspected carpal tunnel syndrome, as it's the gold standard diagnostic test. Ultrasound is useful for evaluating tendons and can be done during your office visit. MRI is reserved for complex cases where diagnosis remains unclear, surgical planning is needed, or masses are suspected. Your doctor will recommend imaging based on your specific symptoms and initial test results.
Yes, diabetes increases risk for both conditions. High blood sugar damages nerves (diabetic neuropathy) and also affects tendons and connective tissues. People with diabetes are 3-4 times more likely to develop carpal tunnel syndrome than those without diabetes. They also have increased risk of tendon problems due to glycosylation of collagen fibers, which makes tendons stiffer and more prone to injury.
Request electrodiagnostic testing (EMG/NCS) before starting aggressive treatment or considering surgery. While experienced clinicians can make accurate clinical diagnoses, nerve testing provides objective confirmation and measures severity, which guides treatment decisions. If your doctor is unwilling to order testing, consider seeking a second opinion from a hand surgeon or neurologist.
Most people notice some improvement within 2-4 weeks of consistent night splinting for carpal tunnel syndrome. Maximum benefit typically occurs after 6-8 weeks. If you experience no improvement after 8 weeks of proper splinting use, the diagnosis may be incorrect or the condition may be too severe for conservative treatment. Splinting works best for mild to moderate cases.
Not necessarily. Carpal tunnel braces keep the wrist in a neutral position and are worn primarily at night. Tendonitis braces may immobilize different movements depending on which tendon is affected. De Quervain's tendonitis requires thumb immobilization, while flexor tendonitis may need different support. Use a brace specifically designed for your diagnosed condition for best results.
Carpal Tunnel vs Tendonitis diagnosis requires much more than simple at-home wrist tests. The popular Phalen's, Tinel's, and Durkan's tests have accuracy rates as low as 51%, meaning they miss nearly half of actual cases and produce false positives in many people without the condition[4]. These tests can mislead because they only assess symptom provocation, not the underlying structural or functional problems causing symptoms.
Accurate diagnosis depends on integrating multiple sources of information: detailed symptom history, comprehensive physical examination, electrodiagnostic testing with 95-98% accuracy[7], and appropriate imaging when needed. Carpal tunnel syndrome involves median nerve compression causing numbness in specific fingers and nighttime awakening, while tendonitis involves inflamed tendons causing pain with movement. The conditions can coexist, further complicating diagnosis.
If you're experiencing wrist pain or numbness:
If you've been diagnosed but treatment isn't working:
For prevention:
The key message: don't let simple wrist tests mislead you into thinking you have an accurate diagnosis or, worse, into delaying proper evaluation. Early, accurate diagnosis followed by appropriate treatment prevents permanent nerve damage and chronic tendon problems. When it comes to Carpal Tunnel vs Tendonitis, professional evaluation with objective testing is the only reliable path to correct diagnosis and effective treatment.
For comprehensive care and accurate diagnosis of wrist conditions, consider consulting with specialists who use evidence-based diagnostic approaches rather than relying solely on physical examination tests. Your wrists are essential for nearly every daily activity—they deserve accurate diagnosis and proper treatment.
[1] Jospt.2020 - https://www.jospt.org/doi/10.2519/jospt.2020.9599
[2] Carpal Tunnel Which Tests Matter - https://curemycarpaltunnel.com/blog/carpal-tunnel-which-tests-matter/
[3] 25133 Phalens Test - https://my.clevelandclinic.org/health/diagnostics/25133-phalens-test
[4] Phalen's Test - https://www.physio-pedia.com/Phalen%E2%80%99s_Test
[5] Tests Used To Diagnose Carpal Tunnel Syndrome - https://www.baltimoreperipheralnervepain.com/blog/tests-used-to-diagnose-carpal-tunnel-syndrome.cfm
[6] Ncs Testing For Carpal Tunnel Syndrome Diagnosis And Beyond - https://integrity-dx.com/blog/ncs-testing-for-carpal-tunnel-syndrome-diagnosis-and-beyond/
[7] Emg Testing For Carpal Tunnel - https://www.indianahandtoshoulder.com/blog/emg-testing-for-carpal-tunnel



