Last updated: March 5, 2026

Carpal tunnel syndrome causes numbness and tingling in the thumb, index, and middle fingers due to nerve compression at the wrist. Cervical radiculopathy (a pinched nerve in the neck) causes similar hand symptoms, but also produces neck pain, shoulder pain, and symptoms that radiate down the entire arm from the neck. The key differentiator: if your neck hurts or moves poorly alongside your hand symptoms, the problem is more likely coming from the spine, not the wrist. A nerve conduction study confirms which condition — or both — is present.
Carpal tunnel syndrome and cervical radiculopathy are two distinct nerve compression problems that produce surprisingly similar symptoms in the hand and arm. That overlap is the core reason they're frequently mixed up — even by experienced clinicians.
Carpal Tunnel Syndrome (CTS) occurs when the median nerve is compressed as it passes through the carpal tunnel, a narrow passageway in the wrist formed by bones and a tough ligament (the transverse carpal ligament). The median nerve supplies sensation to the thumb, index finger, middle finger, and the thumb-side half of the ring finger. When it's squeezed, those fingers go numb, tingle, or ache. [5]
Cervical Radiculopathy is a pinched nerve at the root — specifically, where a spinal nerve exits the cervical (neck) vertebrae. The most common culprits are disc herniation, disc degeneration, or bone spurs that narrow the foramen (the opening the nerve passes through). The C6 and C7 nerve roots are most frequently involved, and because these roots contribute fibers to the same hand regions as the median nerve, the symptom overlap can be striking. [2]
"The challenge isn't just that both conditions cause hand tingling — it's that the nerve pathways physically overlap, making symptom location alone an unreliable guide."
Why the confusion matters: Treating the wrong condition wastes months of recovery time. A wrist splint won't fix a herniated disc, and cervical spine surgery won't relieve a compressed median nerve at the wrist. Getting the diagnosis right from the start is essential.
For a broader look at conditions that mimic carpal tunnel, see this comparison of carpal tunnel vs other conditions.
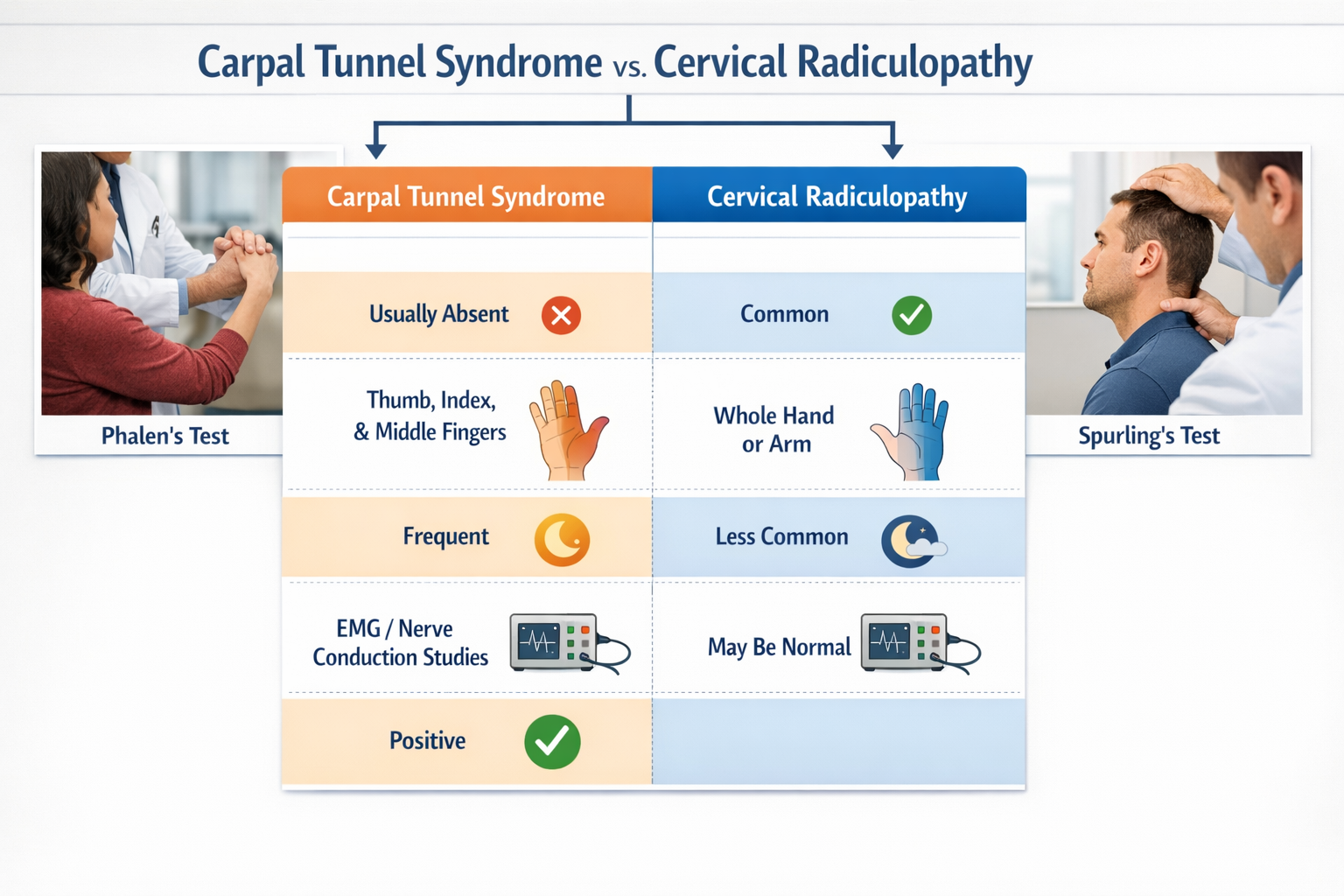
The symptom profiles of carpal tunnel vs cervical radiculopathy ("pinched nerve" in neck) overlap significantly, but several distinguishing features help separate them.
ConditionNerve AffectedTypical Finger SymptomsCarpal Tunnel SyndromeMedian nerve (wrist)Thumb, index, middle, radial half of ring fingerC6 RadiculopathyC6 nerve root (neck)Thumb, index finger, lateral forearmC7 RadiculopathyC7 nerve root (neck)Middle finger, index finger, back of forearmC8 RadiculopathyC8 nerve root (neck)Ring and little finger, medial forearmUlnar nerve entrapmentUlnar nerve (elbow/wrist)Little finger, ring finger
Key insight: C6 and C7 radiculopathy produce finger numbness that closely mirrors carpal tunnel syndrome. C8 radiculopathy, by contrast, affects the little and ring fingers — a pattern that points away from CTS. [4]
For more on how carpal tunnel symptoms can travel up the arm, see how carpal tunnel symptoms can travel.
Several physical examination tests and clinical clues help differentiate these two conditions before ordering imaging or nerve studies.
You can also explore home tests for carpal tunnel to understand what self-assessment looks like before a clinical visit.
Decision rule: If Spurling's maneuver reproduces the patient's arm or hand symptoms, the problem is almost certainly cervical radiculopathy, not carpal tunnel syndrome. [4]
Clinical examination narrows the field, but objective testing confirms which condition is present — especially when both might coexist.
Electrodiagnostic testing is the gold standard for differentiating carpal tunnel syndrome from cervical radiculopathy. [7]
These two tests together can identify the precise location of nerve compression — and can confirm whether both conditions are present simultaneously. [7]
TestBest ForLimitationMRI of the cervical spineDisc herniation, bone spurs, nerve root compressionDoesn't assess wrist directlyMRI of the wristCarpal tunnel anatomy, median nerveDoesn't assess cervical spineX-ray (cervical spine)Degenerative changes, bone spurs, disc narrowingDoesn't show soft tissue or nerveUltrasound (wrist)Median nerve swelling at carpal tunnelOperator-dependent; limited for spine
Important note: Degenerative findings on cervical spine X-ray or MRI — such as osteophytes, disc narrowing, or narrowed neural foramina — increase the likelihood that arm symptoms are radicular rather than from the wrist. [4]
Because the C6 nerve root and the median nerve supply overlapping hand areas, a patient with thumb and index finger numbness could have CTS, C6 radiculopathy, or both. Ordering only a wrist MRI or only a cervical MRI risks missing half the picture. When the clinical story is ambiguous, electrodiagnostic testing covers the entire pathway from neck to fingertip. [7]
Double Crush Syndrome is a real and underappreciated phenomenon where a nerve is compressed at two separate points along its path — for example, at the cervical nerve root and again at the carpal tunnel. Approximately 1 in 4 patients presenting with either suspected cervical radiculopathy or carpal tunnel syndrome may have both conditions. [8]
The theory behind double crush: when a nerve is already under stress from compression at one site, it becomes more vulnerable to injury at a second site. The two compressions together produce symptoms more severe than either would alone.
A striking statistic: One study of 291 patients with confirmed cervical radiculopathy found that 187 of them (64.3%) also had carpal tunnel syndrome, with 154 of those cases involving both hands. [9]
Common mistake: Assuming that because cervical radiculopathy is present, carpal tunnel surgery "won't work." The evidence suggests it often does, and it may be the appropriate first step when wrist-level compression is dominant. [10]
Understanding the root causes helps explain why these conditions sometimes occur together and who is most likely to develop them.
For a deeper look at how pregnancy relates to this condition, see carpal tunnel syndrome and pregnancy.
Risk FactorCarpal TunnelCervical RadiculopathyAge 40–60✓✓Female sex✓ (3x more common)Less pronouncedRepetitive hand/wrist use✓—Desk/computer work✓✓Obesity✓✓Diabetes✓—Degenerative spine changes—✓Prior neck injury—✓
Both conditions are more common after age 40, and both can be aggravated by prolonged desk work and poor ergonomics. This shared risk profile is part of why they co-occur so frequently.
Treatment depends entirely on which condition is confirmed — or, in double crush cases, which compression is more clinically significant.
Conservative (non-surgical) options:
For guidance on conservative approaches, see carpal tunnel physical and occupational therapy techniques and carpal tunnel surgery alternatives.
Surgical option:
Carpal tunnel release — dividing the transverse carpal ligament to decompress the median nerve — is highly effective and one of the most commonly performed outpatient procedures. Recovery timelines vary by job type and hand use demands.
Conservative (non-surgical) options:
Surgical options:
Most cervical radiculopathy cases improve with conservative management. Surgery is reserved for cases with significant weakness, progressive neurological deficit, or failure of prolonged conservative treatment.
When double crush syndrome is confirmed, the treatment sequence matters. Most specialists address the more symptomatic site first and reassess. As noted above, carpal tunnel release has been shown to produce meaningful improvement even in patients with coexisting cervical radiculopathy. [10]
Misdiagnosis between these two conditions is well-documented and has real consequences for patients. Understanding the pitfalls helps both patients and clinicians avoid them.
For more on this topic, see carpal tunnel syndrome misdiagnosis.
Because C6 and C7 radiculopathy affect the same fingers as the median nerve, finger numbness alone cannot confirm CTS. Physical examination tests and electrodiagnostic studies are essential. [4]
Patients often focus on their hand symptoms and don't mention neck stiffness or pain unless asked directly. Clinicians should always ask about neck pain, headaches, and whether neck movement changes hand symptoms.
Finding carpal tunnel syndrome on nerve conduction studies does not rule out cervical radiculopathy. Given that 64.3% of patients with confirmed cervical radiculopathy in one study also had CTS [9], both conditions must be actively considered.
Imaging alone (MRI or X-ray) can show structural abnormalities that are clinically silent. An MRI showing a disc bulge doesn't prove that disc is causing the patient's hand symptoms. EMG and NCS provide functional evidence of nerve compression. [7]
Starting treatment — whether splinting, injections, or surgery — without a confirmed diagnosis risks wasting time and money. A proper workup first saves resources and improves outcomes.
Q: Can a pinched nerve in the neck cause carpal tunnel symptoms?
Yes. Compression of the C6 or C7 nerve root in the neck can produce numbness and tingling in the thumb, index, and middle fingers — the same pattern as carpal tunnel syndrome. This is one of the most common reasons these two conditions are confused. [4]
Q: How do I know if my hand numbness is from my neck or my wrist?
The most reliable clues: neck pain or stiffness alongside hand symptoms suggests a cervical origin. Symptoms that are worst at night and improve with shaking the wrist suggest carpal tunnel. A nerve conduction study and EMG provide the definitive answer. [7]
Q: Does carpal tunnel syndrome cause neck pain?
No. Carpal tunnel syndrome is a wrist-level compression and does not cause neck pain or stiffness. If neck pain accompanies hand numbness, the cervical spine should be investigated. [2]
Q: Can you have carpal tunnel and a pinched nerve in the neck at the same time?
Yes — this is called Double Crush Syndrome. Research suggests roughly 1 in 4 patients with these conditions may have both simultaneously. [8] One study found 64.3% of cervical radiculopathy patients also had carpal tunnel syndrome. [9]
Q: Will carpal tunnel surgery help if I also have cervical radiculopathy?
Often, yes. A retrospective study found that patients with Double Crush Syndrome achieved similar postoperative improvement after carpal tunnel release as those with CTS alone. [10] The key is confirming which compression is dominant before proceeding.
Q: What is Spurling's test and what does it show?
Spurling's maneuver involves applying downward pressure to the head while the neck is extended and rotated toward the affected side. If this reproduces arm or hand symptoms, it strongly suggests cervical nerve root compression — not carpal tunnel syndrome. [4]
Q: Which nerve roots most commonly mimic carpal tunnel syndrome?
C6 and C7 are the most commonly affected roots in cervical radiculopathy, and their symptom distribution closely overlaps with the median nerve territory. C6-C7 disc pathology is the most frequent culprit. [2]
Q: Is cervical radiculopathy more serious than carpal tunnel syndrome?
Both are serious if untreated, but cervical radiculopathy carries a higher risk of progressive arm weakness and, in severe cases, spinal cord involvement (myelopathy). Carpal tunnel syndrome, if left untreated long-term, can cause permanent median nerve damage and thenar muscle wasting. Neither should be ignored.
Q: What is the fastest way to get a correct diagnosis?
See a physician who can perform a focused neurological examination and order electrodiagnostic testing (EMG/NCS). This combination provides the most accurate differentiation between the two conditions and identifies double crush cases.
Q: Can symptoms from a pinched nerve in the neck travel all the way to the hand?
Yes. Cervical radiculopathy causes symptoms that radiate from the neck, through the shoulder, down the arm, and into the hand — following the path of the compressed nerve root. [1] Conversely, severe carpal tunnel syndrome can cause symptoms that seem to travel up the forearm, adding to the diagnostic confusion. [7]
Q: Are there home tests that can help identify carpal tunnel syndrome?
Yes — Phalen's test (holding the wrists in flexion for 60 seconds) and Tinel's sign (tapping over the carpal tunnel) can be performed at home as a preliminary check. For a structured approach, see home tests for carpal tunnel. These tests do not replace clinical evaluation.
Q: What type of doctor should I see for this?
A hand surgeon, orthopedic surgeon, neurologist, or physiatrist (physical medicine and rehabilitation specialist) can evaluate both conditions. If electrodiagnostic testing is needed, a neurologist or physiatrist typically performs it.
Hand numbness, tingling, and arm pain are symptoms that deserve a precise diagnosis — not a best guess. The comparison of carpal tunnel vs cervical radiculopathy ("pinched nerve" in neck) is one of the most clinically important distinctions in upper extremity medicine, precisely because both conditions look alike on the surface but require different treatments.
The bottom line: neck symptoms mean the neck needs investigation. Night-time hand numbness that improves with wrist shaking points to the wrist. When the picture is unclear, electrodiagnostic testing resolves the ambiguity. And when both conditions coexist, treatment can still be effective — carpal tunnel release works even in double crush cases.
For those in the Toronto area seeking expert evaluation and treatment, learn more about carpal tunnel syndrome surgery in Toronto and available carpal tunnel treatment options.
[1] Carpal Tunnel Syndrome Vs Cervical Radiculopathy - https://www.hand2shouldercenter.com/carpal-tunnel-syndrome-vs-cervical-radiculopathy/
[2] Carpal Tunnel Vs Cervical Radiculopathy - https://www.sportsandspinalwellness.com/blog/272080-carpal-tunnel-vs-cervical-radiculopathy
[3] Carpal Tunnel Vs Cervical Radiculopathy - https://www.sportsandspinalwellness.com/blog/272080-carpal-tunnel-vs-cervical-radiculopathy/
[4] CTS Vs C6 - https://www.orthopaedia.com/cts-vs-c6/
[5] Carpal Tunnel Syndrome Vs Cervical Radiculopathy - https://www.spine-health.com/conditions/neck-pain/carpal-tunnel-syndrome-vs-cervical-radiculopathy
[6] Carpal Tunnel Syndrome Vs Cervical Radiculopathy - https://3riversortho.org/2017/03/06/carpal-tunnel-syndrome-vs-cervical-radiculopathy/
[7] Carpal Tunnel Syndrome Or Cervical Radiculopathy: EMG Testing Can Provide The Answer - https://handsonemg.com/carpal-tunnel-syndrome-or-cervical-radiculopathy-emg-testing-can-provide-the-answer/
[8] Carpal Tunnel Syndrome And The Neck - https://chiro-trust.org/carpal-tunnel-syndrome/carpal-tunnel-syndrome-and-the-neck/
[9] PMC10509651 - https://pmc.ncbi.nlm.nih.gov/articles/PMC10509651/
[10] Carpal Tunnel Release Remains Effective In Patients With Double Crush Syndrome And Cervical Radiculopathy - https://www.handtherapyacademy.com/uncategorized/carpal-tunnel-release-remains-effective-in-patients-with-double-crush-syndrome-and-cervical-radiculopathy/



