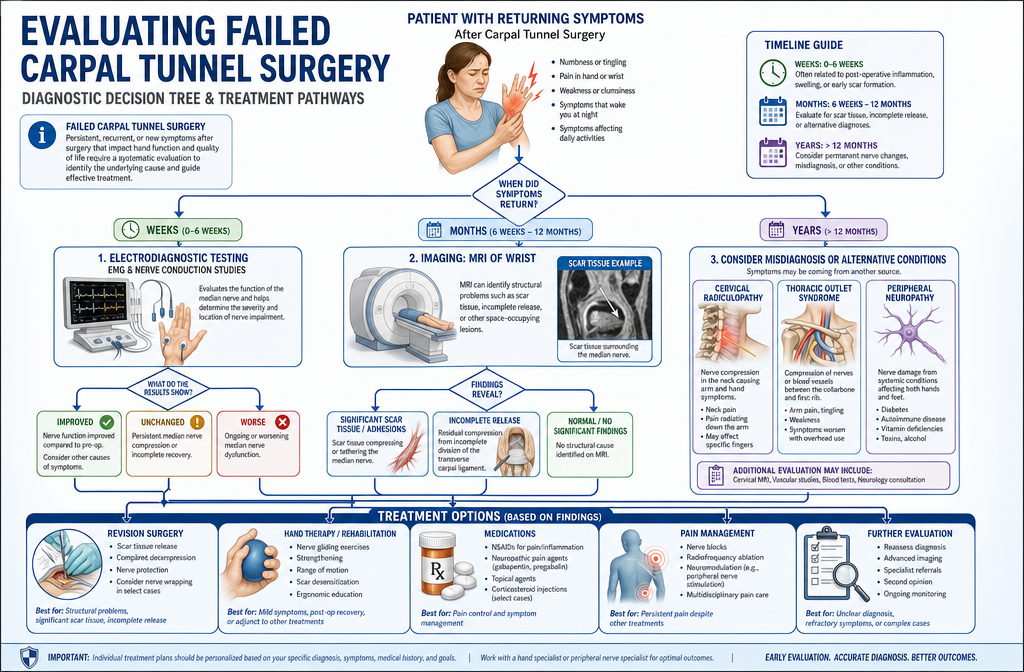
Carpal tunnel surgery failure occurs when symptoms like numbness, tingling, or pain persist or return after carpal tunnel release surgery. This happens in approximately 5-20% of cases and can result from incomplete ligament release, scar tissue formation, misdiagnosis of the original condition, nerve damage during surgery, or development of new compression. The timing of symptom return, whether immediate or delayed, helps determine the underlying cause and appropriate treatment approach.

Carpal tunnel surgery failure means the procedure did not achieve its goal of relieving median nerve compression and eliminating symptoms. This can manifest in three distinct patterns: symptoms that never improved after surgery, symptoms that improved initially but returned within weeks to months, or complete relief followed by new symptom development years later.
The definition of failure depends partly on patient expectations and surgical goals. Some patients experience significant improvement but retain minor symptoms, which may or may not constitute failure depending on the severity of pre-operative symptoms and functional goals.
Common manifestations of surgical failure include:
The timing and pattern of symptoms provide important diagnostic clues. Immediate post-operative symptoms suggest surgical complications or incomplete release, while symptoms appearing months or years later typically indicate scar tissue formation or progression of underlying conditions.
Choose revision evaluation if symptoms persist beyond three months post-surgery or if initially improved symptoms return and interfere with daily function. Many surgeons recommend waiting at least three to six months after initial surgery before considering revision, as some improvement can continue during this healing period.
Carpal tunnel symptoms return in approximately 5-20% of patients after surgery, with rates varying based on surgical technique, surgeon experience, and patient factors. Studies tracking long-term outcomes show that most recurrences happen within the first two years, though some patients experience symptom return five to ten years after initially successful surgery.
The recurrence rate differs significantly between open carpal tunnel release and endoscopic techniques, though both approaches can fail. Patient factors like diabetes, rheumatoid arthritis, obesity, pregnancy, and occupational exposure to vibration or repetitive motion increase recurrence risk substantially.
Factors affecting recurrence rates:
Most patients who experience true surgical success maintain symptom relief long-term. When symptoms do return, they often develop gradually rather than suddenly, giving patients time to seek evaluation before severe nerve damage recurs.
A common mistake is assuming any post-operative discomfort means surgery failed. Normal healing involves incision pain, pillar pain (discomfort at the base of the palm), and temporary weakness that can last several weeks to months. These expected post-operative symptoms differ from true surgical failure.
Persistent numbness and tingling after carpal tunnel release typically indicates either incomplete nerve decompression, permanent nerve damage from pre-operative compression, or an alternative diagnosis that wasn't carpal tunnel syndrome. The median nerve requires time to recover after compression is relieved, but symptoms should show progressive improvement within the first three months.
If numbness and tingling remain unchanged or worsen after surgery, the transverse carpal ligament may not have been completely divided, leaving the nerve partially compressed. This is the most common cause of immediate post-operative symptom persistence and requires careful clinical examination and often repeat nerve conduction studies to confirm.
Reasons for persistent symptoms after surgery:
Timing matters significantly. Symptoms that never improve suggest incomplete release or misdiagnosis, while symptoms that improve then return point toward scar tissue or disease recurrence. Patients with diabetes or other metabolic conditions may experience slower nerve recovery, requiring six months or more to see maximum benefit.
If you still have significant numbness and tingling three months after surgery, consult your surgeon for evaluation. Nerve conduction studies can determine if the nerve remains compressed and whether the electrical signals have improved since pre-operative testing. This objective data helps distinguish incomplete release from slow nerve recovery.
For more information about the standard recovery timeline, see our guide on carpal tunnel surgery recovery.
Incomplete release means the surgeon did not fully divide the transverse carpal ligament during the initial surgery, leaving the median nerve partially compressed. Recurrent carpal tunnel syndrome means the surgery was initially successful with complete ligament release and symptom relief, but new compression developed later due to scar tissue, ligament regrowth, or progression of underlying disease.
These two conditions require different treatment approaches and have different prognoses. Incomplete release typically responds well to revision surgery because the anatomy hasn't been altered by scarring, while recurrent syndrome involves operating through scar tissue, which is more technically challenging.
Key differences:
FeatureIncomplete ReleaseRecurrent Carpal Tunnel SyndromeSymptom timingNever fully resolved after surgeryInitial relief, then symptoms returnCauseSurgical error or technical difficultyScar tissue, disease progressionTime frameImmediate or within weeksMonths to years after surgeryNerve studiesShow persistent compressionMay show new compression or scarringRevision success85-95%60-80%Surgical difficultyEasier, clearer anatomyMore complex due to scar tissue
Incomplete release happens more commonly with endoscopic techniques when the surgeon cannot visualize the entire ligament, though experienced endoscopic surgeons have rates comparable to open surgery. Anatomical variations like a thick ligament, bifid median nerve, or unusual muscle anatomy can make complete release technically challenging regardless of technique.
Recurrent carpal tunnel syndrome often develops when patients have ongoing risk factors like diabetes, inflammatory arthritis, or continued occupational exposure. The body's healing response creates scar tissue around the nerve, or the cut edges of the ligament develop fibrous tissue that gradually compresses the nerve again.
Choose immediate evaluation if symptoms never improved after surgery, as this suggests incomplete release. Wait three to six months if symptoms initially resolved but gradually returned, as some cases improve with conservative treatment like physical therapy and bracing.
Scar tissue can definitely cause carpal tunnel symptoms to return after initially successful surgery. The body's natural healing process creates fibrous scar tissue around the surgical site, and in some patients, this tissue forms adhesions that tether the median nerve or create new compression. This process typically develops gradually over months to years rather than immediately after surgery.
Perineural fibrosis (scarring around the nerve) is one of the most common causes of late symptom recurrence. The scar tissue can bind the nerve to surrounding structures, limiting its normal gliding motion and causing traction injury with wrist movement. In severe cases, the scar tissue itself becomes thick enough to compress the nerve directly.
Factors that increase scar tissue formation:
Scar tissue symptoms often differ slightly from original carpal tunnel symptoms. Patients may notice more pain and burning sensations along with numbness and tingling. The symptoms may worsen with specific wrist positions or activities that stretch the scarred area.
MRI imaging can identify significant scar tissue around the median nerve, though not all scar tissue visible on MRI causes symptoms. Ultrasound examination by an experienced operator can also detect nerve tethering and reduced nerve mobility during wrist movement.
Treatment for symptomatic scar tissue may include physical therapy focused on nerve gliding exercises, corticosteroid injections to reduce inflammation, or revision surgery to remove scar tissue and perform neurolysis (freeing the nerve from adhesions). The success rate for revision surgery addressing scar tissue ranges from 60-80%, lower than revision for incomplete release because scar tissue can reform after the second surgery.
A common mistake is aggressive hand use during the first six weeks after surgery, which increases inflammation and scar formation. Following your surgeon's activity restrictions during healing helps minimize problematic scar tissue development.
Symptoms can return anywhere from immediately after surgery to many years later, with the timing providing important clues about the underlying cause. Immediate symptom persistence suggests incomplete release or surgical complications, while delayed recurrence typically indicates scar tissue formation, disease progression, or development of new compression.
Most recurrences that will happen occur within the first two years after surgery. Studies following patients for five to ten years show that late recurrences (more than five years post-surgery) are uncommon and often relate to new risk factors or progression of systemic conditions like diabetes or arthritis rather than surgical failure.
Typical timeline patterns:
Patients who experience complete symptom relief for at least six months before recurrence almost certainly had successful initial surgery. Their symptom return represents a new problem rather than surgical failure, though the distinction matters less for treatment planning than identifying the current cause of compression.
The speed of symptom return also provides information. Gradual onset over weeks to months suggests progressive scar tissue formation or disease progression, while sudden symptom return may indicate acute nerve injury, new trauma, or development of another condition.
Choose immediate evaluation if symptoms return suddenly or worsen rapidly, as this may indicate a complication requiring urgent treatment. Gradual symptom return warrants evaluation within a few weeks to months, depending on severity and functional impact.
For patients considering surgery, understanding the expected recovery timeline helps set realistic expectations. Learn more about recovery time and returning to work after carpal tunnel surgery.
If carpal tunnel surgery didn't work, your options include conservative management with physical therapy and bracing, corticosteroid injections, revision surgery, or addressing alternative diagnoses that may have been missed. The best approach depends on why the surgery failed, how severe your symptoms are, and how much they interfere with daily function.
Start with a thorough evaluation by a hand surgeon or neurologist to determine the cause of persistent symptoms. This typically includes repeat nerve conduction studies, MRI or ultrasound imaging, and careful physical examination to identify incomplete release, scar tissue, nerve damage, or alternative diagnoses.
Treatment options after failed surgery:
Conservative management:
Interventional treatments:
Surgical options:
Conservative treatment works best for patients with mild to moderate symptoms, especially when scar tissue or inflammation contributes to the problem. Physical therapy can improve nerve mobility and reduce symptoms in 30-40% of patients with failed surgery, potentially avoiding revision surgery.
Revision surgery becomes the best option when nerve conduction studies confirm persistent or recurrent compression, symptoms significantly impair function, and conservative treatment has failed after three to six months. The success rate for revision surgery ranges from 60-90% depending on the cause of failure and whether the nerve has permanent damage.
A common mistake is rushing into revision surgery without proper diagnostic workup. Understanding why the first surgery failed is essential for planning an effective revision procedure and managing expectations about outcomes.
If you're exploring alternatives before considering surgery, review our comprehensive guide to carpal tunnel surgery alternatives.
Whether to pursue revision surgery or try conservative treatment depends on the cause of surgical failure, severity of symptoms, degree of nerve damage, and impact on your daily life. Revision surgery offers the best chance for significant improvement when nerve conduction studies confirm persistent compression and conservative treatment has failed, but it carries higher risks than initial surgery and has lower success rates.
Consider revision surgery if you have objective evidence of continued nerve compression, symptoms that significantly impair hand function or sleep, and you've tried conservative treatment for at least three to six months without adequate improvement. Patients with incomplete ligament release have the best revision outcomes, with success rates of 85-95%.
Choose revision surgery when:
Try conservative treatment first when:
The decision also depends on your expectations and risk tolerance. Revision surgery through scar tissue carries higher risks of nerve injury, infection, and complex regional pain syndrome compared to initial surgery. Success rates of 60-80% mean that 20-40% of patients don't achieve satisfactory improvement even with revision.
Patient factors matter significantly. Diabetic patients, smokers, and those with inflammatory arthritis have lower revision success rates and higher complication risks. Addressing these modifiable factors before revision surgery may improve outcomes.
Seek a second opinion from an experienced hand surgeon if you're uncertain about the best approach. Surgeons who perform high volumes of carpal tunnel surgery and revisions can provide more accurate prognosis and may identify issues missed by less experienced surgeons.
For patients in the Toronto area seeking expert evaluation, specialized carpal tunnel surgery centers offer comprehensive assessment and treatment options.
Nerve damage can be permanent after failed carpal tunnel surgery, especially when severe compression existed for a long time before surgery or when surgical complications injured the nerve. The median nerve has limited capacity for regeneration, and prolonged compression causes irreversible changes to nerve fibers, including demyelination and axonal loss that surgery cannot reverse.
Permanent nerve damage manifests as persistent numbness, loss of two-point discrimination (ability to distinguish two nearby touch points), weakness in thumb opposition, and thenar muscle atrophy (wasting of the muscle at the base of the thumb). These findings indicate that nerve fibers have died and will not recover even with successful decompression.
Factors that increase permanent nerve damage risk:
Nerve conduction studies help predict recovery potential. Severe abnormalities with absent sensory responses or very slow conduction velocities indicate significant nerve damage that may not fully recover. Moderate abnormalities typically improve substantially after successful decompression, though recovery takes months.
Even with permanent nerve damage, surgery may still provide benefit by preventing further deterioration and reducing pain, even if sensation and strength don't fully normalize. Many patients with some permanent damage still achieve functional improvement and symptom reduction that makes surgery worthwhile.
The concept of "point of no return" in nerve compression is important. Nerves compressed for many years undergo structural changes that become irreversible. This is why early surgical intervention for severe carpal tunnel syndrome is recommended rather than prolonged conservative treatment that allows progressive nerve damage.
A common mistake is delaying surgery for years while trying conservative treatments, then expecting complete recovery after surgery. While conservative treatment is appropriate for mild to moderate carpal tunnel syndrome, severe cases with significant nerve damage on testing should proceed to surgery promptly to prevent permanent injury.
If you're experiencing symptoms and wondering whether you need surgery, understanding the severity levels of carpal tunnel syndrome can help you make informed decisions about timing.
Several conditions produce symptoms similar to carpal tunnel syndrome and can be misdiagnosed, leading to surgery that cannot resolve the true problem. The most common mimics include cervical radiculopathy (nerve compression in the neck), thoracic outlet syndrome, peripheral neuropathy, tendonitis, and arthritis. Accurate diagnosis requires careful clinical examination and appropriate testing beyond just nerve conduction studies.
Cervical radiculopathy from a herniated disc or bone spurs in the neck can cause hand numbness and tingling that patients and even some doctors mistake for carpal tunnel syndrome. The key difference is that cervical radiculopathy typically affects different fingers (often the thumb and index finger for C6 radiculopathy, or the ring and small fingers for C8), includes neck or arm pain, and worsens with neck movements.
Common conditions misdiagnosed as carpal tunnel syndrome:
Cervical radiculopathy:
Thoracic outlet syndrome:
Peripheral neuropathy:
Pronator syndrome:
De Quervain's tenosynovitis:
Arthritis:
Double crush syndrome complicates diagnosis further. This condition involves nerve compression at multiple sites, such as both the neck and wrist. Surgery on the wrist alone won't fully resolve symptoms if significant neck compression also exists. Careful examination and sometimes cervical spine MRI help identify this situation.
The misdiagnosis rate for carpal tunnel syndrome ranges from 5-20% depending on the study and diagnostic criteria used. This means that a significant number of patients undergoing surgery don't actually have carpal tunnel syndrome as their primary problem, explaining why surgery fails to help them.
Choose a surgeon who performs thorough clinical examination including neck evaluation, tests for alternative diagnoses, and correlates symptoms with nerve conduction study findings. Nerve conduction studies alone cannot diagnose carpal tunnel syndrome; they must be interpreted in the context of clinical symptoms and examination findings.
For a detailed comparison of carpal tunnel syndrome with other conditions, see our guide on carpal tunnel vs other conditions and carpal tunnel syndrome misdiagnosis.
Doctors diagnose why carpal tunnel surgery failed through a combination of detailed patient history, physical examination, repeat nerve conduction studies, and imaging with MRI or ultrasound. The evaluation focuses on determining whether the nerve remains compressed, identifying scar tissue or anatomical problems, and ruling out alternative diagnoses that may have been missed initially.
The history provides crucial information about symptom timing and pattern. Symptoms that never improved suggest incomplete release or misdiagnosis, while initial relief followed by gradual return points toward scar tissue or disease recurrence. The specific symptoms matter too: burning pain suggests nerve injury or complex regional pain syndrome, while classic numbness and tingling indicate ongoing compression.
Diagnostic evaluation components:
Clinical examination:
Nerve conduction studies:
MRI imaging:
Ultrasound examination:
Additional tests when indicated:
The diagnostic workup should identify one of several scenarios: incomplete ligament release with persistent compression, complete release with scar tissue causing recurrent compression, nerve injury from surgery, misdiagnosis with another condition causing symptoms, or permanent nerve damage that cannot improve further.
Incomplete release appears on MRI as residual ligament tissue compressing the nerve. The nerve may appear swollen above the compression point and flattened at the compression site. Scar tissue shows as abnormal tissue surrounding the nerve with loss of normal fat planes between structures.
A common mistake is assuming failed surgery means surgical error. Many failures result from patient factors, disease progression, or diagnostic challenges rather than technical mistakes. A thorough evaluation identifies the true cause and guides appropriate treatment.
Seek evaluation from a hand surgeon experienced in revision surgery, as they have the expertise to identify subtle causes of failure that less experienced surgeons might miss. High-volume centers often have better diagnostic protocols and more experience interpreting complex cases.
Revision carpal tunnel surgery is generally less successful than first-time surgery, with success rates ranging from 60-90% compared to 85-95% for initial surgery. The lower success rate reflects several factors: operating through scar tissue is technically more challenging, some patients have permanent nerve damage that cannot improve, and recurrent cases often involve complex underlying conditions that contributed to the initial failure.
The success rate for revision surgery varies significantly based on the reason for failure. Incomplete ligament release has the best prognosis, with success rates of 85-95% because the anatomy is relatively preserved and the problem is straightforward to correct. Revision for scar tissue has intermediate success rates of 70-80%, while revision for misdiagnosis or severe nerve damage has the poorest outcomes.
Factors affecting revision surgery success:
Favorable factors (higher success rates):
Unfavorable factors (lower success rates):
Revision surgery is technically more demanding than initial surgery. The surgeon must work through scar tissue, carefully identify the median nerve without injuring it, completely release any remaining ligament, perform neurolysis to free the nerve from adhesions, and sometimes use tissue to wrap the nerve or prevent scar reformation.
Complications occur more frequently with revision surgery compared to initial surgery. Nerve injury risk increases from less than 1% to 2-5%, infection rates are slightly higher, and complex regional pain syndrome (a chronic pain condition) develops in 2-5% of revision cases compared to less than 1% of initial surgeries.
Despite lower success rates and higher risks, revision surgery remains the best option for many patients with failed initial surgery, particularly when objective testing confirms persistent nerve compression and conservative treatment has failed. The key is proper patient selection and accurate identification of the failure cause.
Choose revision surgery when you have clear evidence of incomplete release or recurrent compression, symptoms that significantly impair function, realistic expectations about outcomes, and you're willing to accept the higher complication risk. Avoid revision surgery if you have primarily pain without numbness or tingling, normal nerve conduction studies, or unrealistic expectations for complete symptom resolution.
Patients considering revision surgery should discuss expected outcomes, risks, and alternatives thoroughly with their surgeon. Understanding that 20-40% of patients don't achieve satisfactory improvement helps set realistic expectations and make informed decisions.
Surgeons can make several technical errors during carpal tunnel release that lead to surgical failure. The most common mistake is incomplete division of the transverse carpal ligament, leaving part of the ligament intact and the nerve still compressed. This occurs in approximately 2-5% of procedures and happens more frequently with endoscopic techniques when visualization is limited or with anatomical variations that make complete release challenging.
Other surgical errors include injuring the median nerve or its branches during dissection, inadequate release of the distal or proximal extent of the ligament, failure to identify and release anatomical variations like a separate compartment for the thumb flexor tendon, and creating excessive scar tissue through rough tissue handling.
Common surgical errors:
Incomplete ligament release:
Nerve injury:
Inadequate distal or proximal release:
Missing anatomical variations:
Excessive tissue trauma:
Not all surgical failures result from errors. Some patients have anatomical variations that make complete release technically challenging even for experienced surgeons. Others develop complications like infection or excessive scar tissue despite technically perfect surgery.
Surgeon experience significantly affects outcomes. Studies show that surgeons performing more than 50 carpal tunnel releases annually have lower complication rates and better outcomes than lower-volume surgeons. This doesn't mean low-volume surgeons are incompetent, but experience with the procedure and its potential complications improves results.
The choice between open and endoscopic technique depends partly on surgeon experience and comfort. Both techniques can achieve excellent results in experienced hands, and both can fail. Open surgery provides better visualization and may be preferred for revision cases or when anatomical variations are suspected, while endoscopic surgery offers faster recovery and less scar discomfort when performed by experienced surgeons.
A common mistake patients make is choosing a surgeon based solely on convenience or cost rather than experience and outcomes. While most surgeons can perform competent carpal tunnel release, choosing a hand surgeon or orthopedic surgeon who specializes in hand surgery and performs high volumes of the procedure reduces failure risk.
For patients in the Greater Toronto Area seeking experienced surgeons, specialized carpal tunnel surgery centers offer expertise in both initial and revision procedures.
Carpal tunnel surgery failure is considered medical malpractice only when the surgeon's care fell below the accepted standard of practice and that substandard care directly caused injury or harm to the patient. Not all surgical failures constitute malpractice, as even properly performed surgery can fail due to patient factors, anatomical variations, or disease progression beyond the surgeon's control.
Medical malpractice requires proving four elements: the surgeon owed a duty of care to the patient, the surgeon breached that duty by providing substandard care, the breach directly caused injury, and the patient suffered damages as a result. Simply having a poor outcome or persistent symptoms doesn't meet this standard unless negligence can be demonstrated.
Situations that may constitute malpractice:
Clear surgical errors:
Failure to obtain informed consent:
Inadequate pre-operative evaluation:
Post-operative negligence:
Situations that typically do not constitute malpractice:
The standard of care is determined by what a reasonably competent surgeon with similar training would do in similar circumstances. Surgical technique variations exist, and not all surgeons perform the procedure identically. As long as the approach falls within accepted practice standards, differences in technique don't constitute malpractice.
Proving medical malpractice requires expert testimony from other surgeons who can review the medical records, operative notes, and outcomes to determine whether care met accepted standards. This process is complex and expensive, and many cases that patients perceive as malpractice don't meet the legal standard.
If you believe you experienced malpractice, consult with a medical malpractice attorney who can review your case and obtain expert opinions. Most attorneys offer free initial consultations and work on contingency (no fee unless they win). However, understand that the legal process is lengthy, stressful, and uncertain, and many patients find that focusing on getting appropriate treatment for their current condition provides more benefit than pursuing litigation.
A common mistake is confusing poor outcomes with malpractice. Medicine involves uncertainty, and even excellent surgeons experience complications and failures. The question isn't whether the outcome was perfect, but whether the care provided met professional standards.
Carpal tunnel surgery failure, while relatively uncommon, affects 5-20% of patients and can result from multiple causes including incomplete ligament release, scar tissue formation, misdiagnosis, nerve damage, and disease progression. Understanding why symptoms persist or return after surgery is essential for determining the most appropriate treatment approach and setting realistic expectations for outcomes.
The timing and pattern of symptom return provides important diagnostic clues. Immediate persistence suggests incomplete release or misdiagnosis, while delayed recurrence typically indicates scar tissue or disease progression. Thorough evaluation with repeat nerve conduction studies and imaging helps identify the specific cause and guide treatment decisions.
Treatment options range from conservative management with physical therapy and bracing to revision surgery, with the best approach depending on the cause of failure, symptom severity, and degree of nerve damage. Revision surgery offers 60-90% success rates when the cause is properly identified, though outcomes are generally less favorable than initial surgery.
Key action steps if you're experiencing carpal tunnel surgery failure:
Prevention remains the best approach to surgical failure. Choose an experienced surgeon who performs high volumes of carpal tunnel surgery, follow post-operative activity restrictions carefully, address underlying medical conditions, and modify activities that contribute to nerve compression. Early surgical intervention for severe carpal tunnel syndrome prevents permanent nerve damage that cannot be reversed even with successful surgery.
For patients in the Greater Toronto Area seeking expert evaluation and treatment for carpal tunnel syndrome, whether initial surgery or revision procedures, The Minor Surgery Center offers specialized care with experienced surgeons and comprehensive diagnostic capabilities.
If you're experiencing symptoms and want to understand your options before considering surgery, explore our resources on carpal tunnel treatment alternatives and prevention strategies.
Remember that while carpal tunnel surgery failure can be frustrating and concerning, most cases can be successfully managed with appropriate evaluation and treatment. Working with experienced specialists who understand the complexities of failed carpal tunnel surgery gives you the best chance for improvement and return to normal hand function.
How long should I wait before considering revision surgery?
Wait at least three to six months after initial surgery before considering revision, as nerve recovery and symptom improvement can continue during this period. If symptoms are severe, rapidly worsening, or nerve studies show significant ongoing compression, earlier revision may be appropriate. Use this time to try conservative treatments like physical therapy and to complete thorough diagnostic evaluation.
Can carpal tunnel syndrome come back after successful surgery?
Yes, carpal tunnel syndrome can recur years after initially successful surgery due to scar tissue formation, ligament regrowth, or progression of underlying conditions like diabetes or arthritis. Late recurrence (more than two years after surgery) is less common than early failure but does occur in approximately 2-5% of patients over a 10-year period.
Will my insurance cover revision carpal tunnel surgery?
Most insurance plans cover medically necessary revision surgery when conservative treatment has failed and objective testing confirms persistent or recurrent nerve compression. Documentation of failed conservative treatment and clear diagnostic evidence of ongoing compression are typically required for approval. Check with your insurance provider about specific coverage requirements and pre-authorization needs.
How do I know if my surgeon made a mistake during my carpal tunnel surgery?
You cannot definitively know if a surgical error occurred without thorough evaluation including review of operative notes, repeat nerve conduction studies, and imaging. Persistent symptoms don't automatically mean an error occurred, as many failures result from patient factors or disease progression. If you suspect an error, seek evaluation from another experienced hand surgeon who can provide an objective assessment.
What is the success rate for a second carpal tunnel surgery?
Success rates for revision carpal tunnel surgery range from 60-90% depending on the cause of initial failure. Incomplete release has the best prognosis at 85-95%, scar tissue has intermediate success at 70-80%, and cases with permanent nerve damage or complex underlying conditions have lower success rates of 50-70%. Your specific prognosis depends on individual factors that your surgeon can discuss.
Can physical therapy help if carpal tunnel surgery failed?
Physical therapy can help 30-40% of patients with failed carpal tunnel surgery, particularly when scar tissue or nerve adhesions contribute to symptoms. Therapy focuses on nerve gliding exercises, scar tissue mobilization, and activity modification. It works best for mild to moderate symptoms and is worth trying before considering revision surgery unless you have clear evidence of significant ongoing nerve compression.
How can I tell the difference between normal post-operative pain and surgical failure?
Normal post-operative pain includes incision discomfort, pillar pain at the palm base, and temporary weakness that gradually improves over weeks to months. Surgical failure typically involves persistent or worsening numbness and tingling in the median nerve distribution (thumb, index, middle, and ring fingers), night symptoms that don't improve, and symptoms that remain unchanged or worsen beyond three months after surgery.
What questions should I ask my surgeon about revision surgery?
Ask about the specific cause of your surgical failure, what the revision surgery will involve, expected success rates for your situation, risks and complications, recovery time, alternatives to surgery, and your surgeon's experience with revision cases. Also ask what will be done differently in the revision to address the cause of failure and prevent recurrence.
Can I prevent carpal tunnel syndrome from coming back after revision surgery?
You can reduce recurrence risk by controlling underlying conditions like diabetes, maintaining healthy weight, modifying activities that stress the wrist, using proper ergonomics at work, performing regular wrist exercises, and following all post-operative restrictions carefully. However, some recurrence risk remains, particularly if you have genetic predisposition or unavoidable occupational exposures.
Should I see the same surgeon who did my first surgery or find someone new?
This depends on your relationship with the original surgeon and their experience with revision surgery. If you trust your surgeon and they have revision experience, they may be the best choice as they know your anatomy and surgical history. However, seeking a second opinion or choosing a surgeon who specializes in revision surgery is reasonable, especially if you have concerns about the initial procedure or if your surgeon has limited revision experience.
How much does revision carpal tunnel surgery cost?
Costs vary widely based on location, surgeon, facility, and insurance coverage. Without insurance, revision surgery typically costs between $3,000-$8,000 including surgeon fees, facility fees, and anesthesia. With insurance, your out-of-pocket costs depend on your deductible, copayments, and coverage terms. Get detailed cost estimates from your surgeon's office and verify coverage with your insurance before proceeding.
What are the risks of having multiple carpal tunnel surgeries on the same wrist?
Multiple surgeries increase risks of nerve injury (2-5% vs less than 1% for initial surgery), infection, complex regional pain syndrome, excessive scar tissue formation, and permanent stiffness. Success rates also decrease with each subsequent surgery. These increased risks must be weighed against the potential benefits when considering multiple revisions.



