Last updated: June 9, 2026
Carpal tunnel in musicians occurs when repetitive hand movements and sustained awkward wrist positions compress the median nerve in the wrist, causing pain, numbness, and weakness. Early intervention with proper technique, ergonomic adjustments, and targeted stretches can prevent progression, while severe cases may require splinting, corticosteroid injections, or surgical release. Most musicians can return to playing after treatment, though recovery timelines vary from weeks to several months depending on severity and treatment approach.
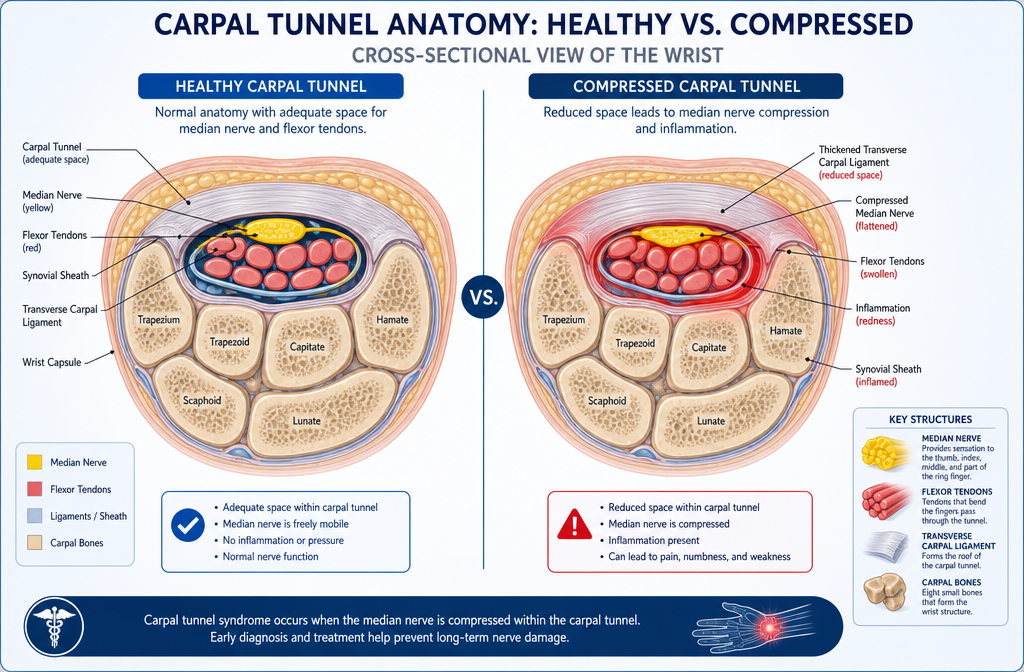
Carpal tunnel syndrome in musicians develops when the median nerve becomes compressed as it passes through the narrow carpal tunnel in the wrist. This compression results from repetitive hand motions, sustained non-neutral wrist positions, and forceful gripping that increase pressure inside the carpal tunnel, reducing blood flow to the nerve and causing inflammation.
Musicians face several specific risk factors that contribute to carpal tunnel development:
Repetitive finger movements: Pianists may perform 10,000-15,000 keystrokes during a single practice session, creating cumulative stress on the flexor tendons that share space with the median nerve in the carpal tunnel.
Sustained wrist flexion or extension: Guitarists often hold their fretting hand in 30-40 degrees of wrist extension for extended periods, which narrows the carpal tunnel space by up to 40% and increases internal pressure.
Forceful gripping: String players apply significant grip force to bows and fingerboards, which increases tendon inflammation and fluid accumulation within the carpal tunnel.
Lack of rest periods: Professional musicians frequently practice 4-8 hours daily without adequate breaks, preventing tissue recovery and allowing micro-trauma to accumulate.
Poor technique: Incorrect hand positioning, excessive tension, and compensatory movements place additional stress on wrist structures.
The condition develops gradually over months or years as repeated compression episodes damage the protective myelin sheath around the median nerve. Initially, symptoms appear only during or immediately after playing. As damage progresses, symptoms persist longer and eventually occur at rest or during sleep when wrist flexion during sleep further compresses the already irritated nerve.
Choose immediate intervention if you notice symptoms appearing earlier in practice sessions or persisting after you stop playing, as this indicates progressive nerve damage that responds better to early treatment.
Guitar players typically first notice intermittent tingling or numbness in the thumb, index, middle, and ring fingers of their fretting hand, particularly after extended practice sessions or performances. These sensations often resolve initially with rest but gradually become more frequent and persistent as the condition progresses.
Specific early warning signs for guitarists include:
The pattern of affected fingers provides an important diagnostic clue: carpal tunnel syndrome affects only the thumb, index, middle, and ring fingers because these receive sensation from the median nerve. The pinky finger remains unaffected because it receives sensation from the ulnar nerve, which travels through a different anatomical pathway.
Guitar players often initially dismiss these symptoms as normal fatigue or attribute them to "playing through the pain." This delay in recognition allows the condition to progress from reversible nerve irritation to potentially permanent nerve damage.
Common mistake: Continuing to practice at full intensity when symptoms appear. Guitarists should reduce practice duration by 30-50% and eliminate the most aggravating techniques when early symptoms emerge, as this modification period often prevents progression to chronic carpal tunnel syndrome.
When symptoms persist beyond 2-3 weeks despite rest and technique modifications, or when they begin interfering with daily activities beyond music (difficulty buttoning shirts, holding a phone, typing), professional evaluation becomes necessary to prevent irreversible nerve damage.
Carpal tunnel syndrome and tendonitis both cause wrist and hand pain in pianists, but they affect different structures and produce distinct symptom patterns. Carpal tunnel involves median nerve compression, while tendonitis involves inflammation of the tendons that move the fingers and wrist.
Key distinguishing features:
FeatureCarpal Tunnel SyndromeTendonitisLocation of painPalm side of thumb, index, middle, and half of ring fingerSpecific tendon path along forearm, wrist, or handNumbness/tinglingPresent, especially at nightAbsent or minimalTiming of symptomsWorse at night and upon wakingWorse during and immediately after activityAffected fingersThumb through ring finger onlyAny finger depending on which tendon is inflamedRelief with restPartial; nighttime symptoms persistSignificant improvement with restWeakness patternThumb opposition and grip strengthSpecific movement related to inflamed tendonResponse to wrist positionWorse with sustained flexion or extensionWorse with specific movements that stress the tendon
Diagnostic tests pianists can perform:
Phalen's test (for carpal tunnel): Hold the backs of your hands together with wrists fully flexed for 60 seconds. If this reproduces numbness or tingling in the median nerve distribution within 60 seconds, carpal tunnel is likely.
Tinel's sign (for carpal tunnel): Tap gently over the median nerve at the wrist crease. A tingling sensation shooting into the fingers suggests carpal tunnel syndrome.
Resisted movement test (for tendonitis): Have someone provide resistance while you perform specific finger or wrist movements. Sharp, localized pain along a tendon path indicates tendonitis.
Pianists with carpal tunnel typically report that symptoms wake them at night and improve with shaking the hand. Tendonitis pain generally does not cause nighttime awakening unless the pianist sleeps directly on the inflamed tendon.
Edge case: Pianists can develop both conditions simultaneously. Repetitive finger movements inflame tendons while sustained wrist positions compress the median nerve. If symptoms include both localized tendon pain during playing and nighttime numbness, both conditions may be present and require concurrent treatment.
For more information on distinguishing between these conditions, see our detailed guide on carpal tunnel vs tendonitis.
Drummers should perform wrist flexor stretches, wrist extensor stretches, and median nerve glides daily to maintain tissue flexibility and reduce carpal tunnel pressure. These stretches take 5-10 minutes and are most effective when performed before practice, during breaks, and after playing sessions.
Essential stretching routine for drummers:
Wrist flexor stretch:
Wrist extensor stretch:
Median nerve glide:
Prayer stretch:
Drummer-specific considerations:
Drummers should pay particular attention to the wrists that perform the most repetitive motions. For most drummers, the dominant hand performing hi-hat or ride cymbal patterns accumulates more repetitive stress than the hand playing less frequent fills.
Timing recommendations:
Common mistake: Stretching too aggressively or bouncing during stretches. Drummers should apply gentle, sustained tension that creates a pulling sensation but not pain. Overstretching can irritate tissues and worsen symptoms.
Choose static stretches (holding positions) over ballistic stretches (bouncing movements) because sustained gentle tension effectively lengthens tissues without causing micro-tears that lead to inflammation.
For additional exercises that complement these stretches, explore our comprehensive carpal tunnel exercise guide.
Wrist braces help musicians with carpal tunnel by maintaining the wrist in a neutral position, which maximizes the space within the carpal tunnel and reduces pressure on the median nerve. Night splinting provides the most benefit because it prevents the wrist flexion that occurs during sleep and causes morning symptoms, while daytime bracing during practice can help in moderate cases but may interfere with technique.
Evidence for brace effectiveness:
Studies show that wearing a neutral-position wrist brace at night for 4-6 weeks reduces symptoms in 60-80% of people with mild to moderate carpal tunnel syndrome. The brace prevents the wrist from flexing beyond 20 degrees, which keeps the carpal tunnel at its maximum diameter and reduces nerve compression during the 6-8 hours of sleep.
Brace recommendations for musicians:
Night bracing (recommended for all musicians with symptoms):
Daytime bracing (selective use):
Brace selection criteria:
Choose a brace with a rigid palmar stay (metal or plastic insert) that prevents wrist flexion and extension. Soft elastic braces without rigid support provide compression but do not adequately immobilize the wrist in the neutral position needed to reduce carpal tunnel pressure.
The brace should feel snug but not tight enough to cause numbness or tingling. If symptoms worsen while wearing the brace, it may be positioned incorrectly or fastened too tightly.
Limitations for musicians:
Daytime bracing during practice creates a significant limitation: the brace restricts the wrist mobility needed for proper technique on most instruments. Pianists cannot achieve the subtle wrist movements needed for dynamic control, guitarists lose the wrist flexibility needed for vibrato, and string players cannot execute proper bow technique.
Decision rule: Use night bracing consistently for all musicians with carpal tunnel symptoms. Add daytime bracing during practice only if symptoms persist despite night bracing and technique modifications, and only during practice sessions focused on slow, technical work rather than performance preparation.
For guidance on selecting the right brace for your specific needs, see our article on choosing the right carpal tunnel brace or splint.
Carpal tunnel surgery for professional musicians typically costs between $3,000 and $8,000 in the United States, with the total depending on whether the procedure is performed in a hospital or outpatient surgery center, the surgeon's experience with musicians, and insurance coverage. Out-of-pocket costs for insured patients range from $500 to $2,500 after deductibles and copays, while uninsured musicians pay the full amount.
Cost breakdown by setting:
Outpatient surgery center: $3,000-$5,000 total
Hospital outpatient department: $5,000-$8,000 total
Additional costs musicians should budget for:
Insurance considerations:
Most insurance plans cover carpal tunnel surgery when conservative treatment (splinting, therapy, injections) has failed after 6-12 weeks. Musicians should obtain pre-authorization and confirm that their surgeon is in-network to minimize out-of-pocket costs.
Professional musicians may face additional considerations when timing surgery around performance schedules, as rushing back to playing before adequate healing can compromise surgical outcomes and require revision surgery costing an additional $5,000-$10,000.
Cost-saving strategies:
Edge case: Professional musicians whose livelihood depends on performance may benefit from seeking surgeons with specific experience treating performing artists, even if this requires traveling to specialized centers. These surgeons typically charge standard fees but provide rehabilitation protocols specifically designed to return musicians to performance level, potentially reducing the total recovery time and lost income.
For musicians in the Toronto area, The Minor Surgery Center offers specialized carpal tunnel treatment with board-certified surgeons experienced in treating performing artists.
Most musicians can return to playing their instruments after carpal tunnel surgery, with 75-90% achieving full or near-full return to their previous performance level within 3-6 months. The timeline varies based on the instrument, the severity of nerve damage before surgery, adherence to rehabilitation protocols, and whether the musician follows a graduated return-to-play program rather than resuming full practice immediately.
Return-to-play timeline by instrument:
Piano and keyboards: 6-12 weeks for light playing, 3-4 months for full repertoire
Guitar (acoustic and electric): 8-12 weeks for basic playing, 3-5 months for full technique
Violin, viola, cello: 8-14 weeks for basic technique, 4-6 months for performance level
Drums and percussion: 6-10 weeks for light playing, 3-4 months for full intensity
Graduated return-to-play protocol:
Weeks 1-2 post-surgery:
Weeks 3-4:
Weeks 5-8:
Weeks 9-12:
Months 4-6:
Factors affecting return to playing:
Musicians with severe nerve damage before surgery (constant numbness, visible thumb muscle atrophy) may experience incomplete recovery and permanent limitations in fine motor control. Early surgery before permanent nerve damage occurs provides the best outcomes.
Common mistake: Returning to full practice intensity too quickly. Musicians who resume their normal 3-4 hour practice schedule within 4-6 weeks post-surgery have higher rates of incision problems, scar tissue formation, and persistent pain that delays ultimate return to performance level.
Decision rule: Choose a conservative timeline if you are a professional musician whose career depends on optimal hand function. An extra 4-6 weeks of graduated return provides better long-term outcomes than rushing back and risking complications that could end a performing career.
Working with a hand therapist experienced in treating musicians significantly improves outcomes. These specialists design instrument-specific exercises and monitor technique to prevent compensatory patterns that could cause problems in the opposite hand.
Pianists, guitarists, and string players (violin, viola, cello) face the highest risk for carpal tunnel syndrome due to the combination of repetitive finger movements, sustained non-neutral wrist positions, and high practice volumes required for professional-level performance. Among these groups, classical pianists and professional guitarists show the highest incidence rates.
Risk ranking by instrument:
Highest risk:
Moderate risk:
Lower risk:
Additional risk factors that compound instrument-specific risk:
Professional vs amateur musicians:
Professional musicians face substantially higher risk than amateurs because of:
Edge case: Music teachers who demonstrate technique repeatedly throughout the day may accumulate even more repetitive stress than performing musicians, as they play the same passages multiple times for different students without the variation that occurs in personal practice.
Decision rule: If you play a high-risk instrument and practice more than 3 hours daily, implement prevention strategies immediately rather than waiting for symptoms to appear. Early intervention with proper technique, regular breaks, and daily stretching can prevent carpal tunnel development even in high-risk musicians.

Carpal tunnel syndrome is not necessarily permanent if you keep playing music, but continuing to play without treatment or modification allows progressive nerve damage that can become irreversible. Mild to moderate carpal tunnel often resolves with conservative treatment and technique modifications even while continuing to play at reduced intensity, while severe cases with constant numbness and muscle atrophy typically require surgery and may result in permanent deficits if treatment is delayed.
Progression timeline without treatment:
Stage 1 (Reversible - weeks to months):
Stage 2 (Potentially reversible - months to 1-2 years):
Stage 3 (Partially irreversible - 1-3 years):
Stage 4 (Irreversible - 3+ years):
Can you continue playing during treatment?
Musicians can often continue playing during conservative treatment if they make specific modifications:
When continued playing causes permanent damage:
Continuing to play at full intensity despite progressive symptoms accelerates nerve damage. Musicians who ignore worsening symptoms and maintain 4-8 hour daily practice schedules can progress from Stage 1 to Stage 3 within 6-12 months, potentially causing permanent deficits that end performing careers.
Warning signs that continued playing is causing permanent damage:
Decision rule: If symptoms persist or worsen despite 6-8 weeks of conservative treatment and playing modifications, continued playing without surgical intervention risks permanent nerve damage. Choose surgery at this point rather than continuing to play through progressive symptoms.
Edge case: Some professional musicians with mild, stable symptoms manage their condition for years through careful technique, regular breaks, and consistent use of night splints. This approach works only if symptoms remain mild and do not progress. Any worsening requires immediate escalation of treatment.
For more information on whether carpal tunnel can resolve without intervention, see our article on can carpal tunnel go away on its own.
Keyboard players should maintain neutral wrist position (straight line from forearm through hand), adjust bench height so elbows rest at 90-100 degrees, and position the keyboard so the home row sits at elbow height to minimize carpal tunnel risk. These adjustments reduce wrist deviation and pressure within the carpal tunnel during the thousands of keystrokes performed during each practice session.
Essential ergonomic adjustments:
Bench height and position:
Keyboard height and angle:
Wrist position during playing:
Hand and finger technique:
Practice environment setup:
Lighting: Position lighting to illuminate sheet music and keyboard without creating glare that forces awkward head and neck positions that affect shoulder and arm alignment.
Music stand placement: Place sheet music at eye level directly above the keyboard to prevent neck flexion and the forward shoulder roll that affects arm position.
Surrounding workspace: Ensure adequate space on both sides of the keyboard for arm movement without obstruction.
Equipment recommendations:
Adjustable bench: Invest in a quality adjustable bench with fine height adjustment (1-inch increments) rather than using a fixed-height chair or stool.
Keyboard stand: Choose a stand with height adjustment range of 24-36 inches to accommodate different body proportions.
Footrest: Use a footrest if feet don't reach the floor comfortably, as unstable lower body position affects upper body alignment.
Common mistakes keyboard players make:
Decision rule for electronic keyboard players: If you practice on multiple keyboards (home studio, performance venues, teaching studios), invest in a quality adjustable stand that you can set to the same height at each location. Inconsistent setup forces constant adaptation and prevents the neuromuscular learning that supports optimal technique.
Specific adjustments by keyboard type:
Acoustic piano: Limited adjustment options; focus on bench height and distance from keyboard. Consider adding a thin cushion to raise sitting height if the piano sits high relative to your proportions.
Electronic keyboard: Maximum flexibility; adjust both keyboard height and bench height to achieve optimal position.
Organ: Requires additional consideration for foot pedal position; ensure pedals are positioned to allow neutral ankle position without forcing knees too high or too low.
For additional strategies to prevent carpal tunnel in various settings, explore our guide on carpal tunnel prevention.
Musicians should see a doctor for wrist pain when symptoms persist beyond 2-3 weeks despite rest and self-care, when numbness or tingling occurs regularly (especially at night), or when weakness develops that affects playing ability or daily activities. Early medical evaluation prevents progression to permanent nerve damage that may not fully resolve even with treatment.
Specific symptoms requiring prompt medical evaluation:
Immediate evaluation (within 1-3 days):
Evaluation within 1-2 weeks:
Evaluation within 3-4 weeks:
What to expect during medical evaluation:
Initial assessment:
Diagnostic testing:
Choosing the right specialist:
Primary care physician or family doctor: Appropriate for initial evaluation and conservative treatment (splinting, activity modification, anti-inflammatory medication)
Hand surgeon or orthopedic surgeon: Necessary if conservative treatment fails after 6-12 weeks or if symptoms are severe at initial presentation
Neurologist: Appropriate when diagnosis is unclear or when nerve conduction studies show unusual patterns
Occupational medicine specialist: Experienced in work-related repetitive strain injuries and may have specific knowledge of musician injuries
Musician-specific considerations:
Musicians benefit from seeking providers with experience treating performing artists. These specialists understand the demands of professional playing and can design treatment plans that minimize performance disruption while effectively addressing the underlying problem.
Questions musicians should ask during evaluation:
Common mistake: Waiting until symptoms become severe before seeking evaluation. Musicians who delay medical assessment for 6-12 months while symptoms progressively worsen often require surgery and face longer recovery times than those who seek early evaluation and treatment.
Decision rule: If you are a professional musician whose income depends on playing, seek evaluation after 2-3 weeks of symptoms rather than waiting longer. Early intervention provides more treatment options and better outcomes than delayed treatment after permanent nerve damage has occurred.
For musicians in the Greater Toronto Area, specialized carpal tunnel treatment is available with board-certified surgeons experienced in treating performing artists.
Classical musicians develop carpal tunnel syndrome at higher rates than musicians in other genres due to longer practice requirements (typically 4-8 hours daily vs 1-3 hours for most other genres), more technically demanding repertoire requiring precise finger work, and earlier start ages that result in more cumulative years of intensive playing. The combination of high practice volume, complex technique, and performance pressure creates substantially elevated risk compared to jazz, rock, or popular music performers.
Comparative risk factors by genre:
Classical musicians (highest risk):
Jazz musicians (moderate risk):
Rock and popular musicians (moderate to lower risk):
Folk and traditional musicians (lower risk):
Factors explaining the classical music risk elevation:
Practice volume: Classical musicians practice 2-4 times longer daily than musicians in most other genres. A classical pianist preparing for a concerto performance may practice a single piece for 2-3 hours daily for months, while a rock guitarist might learn an entire set list in 10-20 hours of total practice.
Technique precision: Classical performance demands note-perfect execution of complex passages at specific tempos, allowing little room for technical adaptation when discomfort develops. Jazz and popular musicians can modify passages, simplify difficult sections, or improvise alternatives when hand problems emerge.
Repertoire demands: Classical repertoire includes some of the most technically demanding music ever written, with composers often pushing the boundaries of what is physically possible on an instrument. Popular music generally uses more ergonomic, comfortable hand positions.
Performance culture: Classical music culture traditionally emphasizes "playing through pain" and views physical problems as weakness rather than legitimate medical issues. This culture delays treatment and allows conditions to progress further than in genres with more pragmatic approaches to injury.
Early specialization: Classical musicians typically begin intensive training in childhood, accumulating decades of high-volume practice by their 20s and 30s. Musicians in other genres often begin serious study later, reducing cumulative exposure.
Edge case: Session musicians who play multiple hours daily in recording studios face risk levels comparable to classical musicians despite playing popular or commercial music, because their work requires the same high volume and precision as classical performance.
Decision rule: If you are a classical musician, implement prevention strategies from the beginning of serious study rather than waiting for symptoms to develop. The high practice volumes and technical demands make prevention essential rather than optional.
Musicians most commonly cause carpal tunnel syndrome by practicing for extended periods without breaks, using excessive force or tension during playing, maintaining poor wrist positioning, and ignoring early warning symptoms until nerve damage becomes advanced. These mistakes are preventable through awareness and deliberate practice habits that prioritize long-term hand health over short-term practice goals.
Critical mistakes and corrections:
Practicing without breaks:
Using excessive force:
Ignoring wrist position:
Playing through pain:
Neglecting warm-up and stretching:
Poor overall posture:
Inadequate technique foundation:
Ignoring early warning signs:
Inconsistent practice schedule:
Using inappropriate equipment:
Decision rule: If you recognize yourself making any of these mistakes, correct them immediately rather than waiting for symptoms to develop. Prevention is far more effective than treatment once nerve damage has occurred.
Violinists with mild to moderate carpal tunnel syndrome can often avoid surgery through conservative treatment including wrist splinting (especially at night), corticosteroid injections, hand therapy focused on nerve gliding exercises, technique modification to reduce wrist deviation, and activity modification during the 6-12 week treatment period. These approaches resolve symptoms in 60-70% of mild to moderate cases, though severe cases with constant numbness or muscle atrophy typically require surgical intervention.
Conservative treatment options ranked by evidence:
Night splinting (strongest evidence):
Corticosteroid injections:
Hand therapy and nerve gliding exercises:
Activity modification:
Technique modification:
Ergonomic adjustments:
Oral medications:
Alternative therapies with limited evidence:
Acupuncture: Some studies show short-term symptom improvement; mechanism unclear; may be worth trying if other conservative measures fail
Yoga: General benefits for flexibility and body awareness; no specific evidence for carpal tunnel treatment
Vitamin B6 supplementation: Older studies suggested benefit; more recent research shows minimal effect
Ultrasound therapy: Mixed evidence; some studies show benefit, others show no effect beyond placebo
Treatment timeline and decision-making:
Weeks 1-6:
Weeks 6-12:
Weeks 12-16:
When conservative treatment fails:
Surgery becomes necessary when:
Decision rule for violinists: Choose conservative treatment first if symptoms are mild to moderate (intermittent numbness, no muscle atrophy, no constant symptoms). Choose surgery earlier if symptoms are severe at presentation or if you are a professional violinist who cannot afford 3-6 months of reduced playing while attempting conservative treatment.
Edge case: Violinists with upcoming important performances (auditions, competitions, recording sessions) face difficult timing decisions. Corticosteroid injection may provide 3-6 months of symptom relief to get through the immediate performance, followed by more definitive treatment (continued conservative care or surgery) afterward.
For more information on non-surgical options, see our comprehensive guide to carpal tunnel surgery alternatives.
Can carpal tunnel syndrome end a music career?
Carpal tunnel syndrome can end a music career if left untreated until permanent nerve damage occurs, but early diagnosis and appropriate treatment (conservative or surgical) allow most musicians to continue performing. Professional musicians who seek treatment when symptoms first appear and follow rehabilitation protocols typically return to full performance level within 3-6 months.
How long does carpal tunnel surgery recovery take for musicians?
Musicians typically require 6-12 weeks before beginning light playing after carpal tunnel surgery, with full return to performance level taking 3-6 months depending on the instrument and adherence to graduated return-to-play protocols. Pianists and guitarists often return faster than string players due to less demanding wrist positions.
Should I stop playing my instrument if I have carpal tunnel symptoms?
You should reduce playing time by 30-50% when carpal tunnel symptoms first appear rather than stopping completely, as complete rest is usually unnecessary for mild symptoms. However, if symptoms are severe (constant numbness, significant weakness, muscle atrophy), stopping playing temporarily while pursuing treatment prevents further nerve damage.
Do wrist exercises really help prevent carpal tunnel in musicians?
Wrist exercises including flexor and extensor stretches and nerve gliding exercises help prevent carpal tunnel in musicians by maintaining tissue flexibility and nerve mobility, though they work best when combined with proper technique, regular breaks, and neutral wrist positioning during playing. Daily stretching provides the most benefit when performed before practice, during breaks, and after playing.
Can I play guitar with carpal tunnel syndrome?
You can continue playing guitar with mild carpal tunnel syndrome if you reduce practice time, take frequent breaks, wear a night splint, and modify technique to reduce wrist extension in the fretting hand. However, continuing to play at full intensity without treatment allows symptoms to progress and may cause permanent nerve damage.
Is carpal tunnel surgery worth it for musicians?
Carpal tunnel surgery is worth it for musicians when conservative treatment fails after 6-12 weeks or when symptoms are severe at presentation, as 75-90% of musicians achieve good to excellent outcomes and return to performance level within 3-6 months. Delaying surgery when indicated risks permanent nerve damage that may not fully recover even with surgical treatment.
What is the best sleeping position to avoid carpal tunnel symptoms?
The best sleeping position to avoid carpal tunnel symptoms is on your back with arms at your sides and wrists in neutral position, or on your side with arms straight rather than bent under your pillow. Wearing a rigid wrist splint at night prevents the wrist flexion that occurs during sleep and causes morning symptoms.
Can physical therapy cure carpal tunnel syndrome?
Physical therapy including nerve gliding exercises, stretching, and technique modification can resolve symptoms in 50-70% of mild to moderate carpal tunnel cases when combined with night splinting and activity modification. However, physical therapy cannot cure severe carpal tunnel with constant numbness or muscle atrophy, which typically requires surgical intervention.
How do I know if my wrist pain is carpal tunnel or tendonitis?
Carpal tunnel causes numbness and tingling in the thumb, index, middle, and ring fingers (especially at night), while tendonitis causes localized pain along a specific tendon path without numbness. Carpal tunnel symptoms often wake you from sleep and improve with shaking your hand, while tendonitis pain worsens with specific movements that stress the inflamed tendon.
Should I wear a wrist brace while playing my instrument?
You should wear a wrist brace at night consistently but generally avoid wearing it while playing your instrument, as the brace restricts the wrist mobility needed for proper technique on most instruments. Use daytime bracing during practice only if symptoms occur during playing despite night splinting and technique modifications.
Can vitamin supplements help with carpal tunnel syndrome?
Vitamin B6 supplementation was once thought to help carpal tunnel syndrome, but recent research shows minimal benefit beyond placebo effect. Focus on proven treatments including splinting, exercises, technique modification, and medical intervention when necessary rather than relying on supplements.
How much does carpal tunnel affect piano playing specifically?
Carpal tunnel affects piano playing by causing numbness that reduces finger sensitivity needed for dynamic control, weakness that limits ability to play fortissimo passages, and pain that shortens practice tolerance. Pianists with carpal tunnel often first notice difficulty with octave passages, rapid scales, and sustained loud playing before symptoms affect easier repertoire.
Carpal tunnel in musicians represents a serious but manageable occupational hazard that affects thousands of performers across all instruments and genres. The condition develops through the cumulative effects of repetitive hand movements, sustained non-neutral wrist positions, and high practice volumes that compress the median nerve within the narrow carpal tunnel space. While classical musicians face the highest risk due to intensive practice requirements and technically demanding repertoire, all musicians who practice regularly should understand prevention strategies and recognize early warning signs.
Prevention remains the most effective approach to carpal tunnel syndrome. Musicians should implement proper ergonomic setup, maintain neutral wrist positioning during playing, take regular breaks every 20-30 minutes, perform daily stretching exercises, and work with qualified teachers to develop efficient technique that minimizes wrist stress. These strategies require minimal time investment but provide substantial protection against a condition that can threaten performing careers.
When symptoms do develop, early intervention provides the best outcomes. Musicians who notice intermittent numbness, tingling, or weakness should seek medical evaluation within 2-3 weeks rather than waiting for symptoms to progress. Conservative treatment including night splinting, corticosteroid injections, hand therapy, and activity modification resolves symptoms in 60-70% of mild to moderate cases, allowing musicians to avoid surgery while returning to full playing capacity.
For musicians with severe symptoms or those who do not respond to conservative treatment, carpal tunnel surgery offers excellent outcomes, with 75-90% achieving good to excellent results and returning to performance level within 3-6 months. The key to successful surgical outcomes lies in following graduated return-to-play protocols, working with hand therapists experienced in treating musicians, and avoiding the temptation to resume full practice intensity too quickly.
Actionable next steps:
Musicians in the Greater Toronto Area can access specialized carpal tunnel treatment with board-certified surgeons experienced in treating performing artists at locations in Toronto, Mississauga, and Whitby.
Remember that carpal tunnel syndrome does not have to end your musical career. With proper prevention, early recognition, and appropriate treatment, most musicians successfully manage this condition and continue performing at the highest levels for decades. The key lies in respecting the physical demands that musical performance places on your hands and taking proactive steps to protect these essential tools of your craft.



