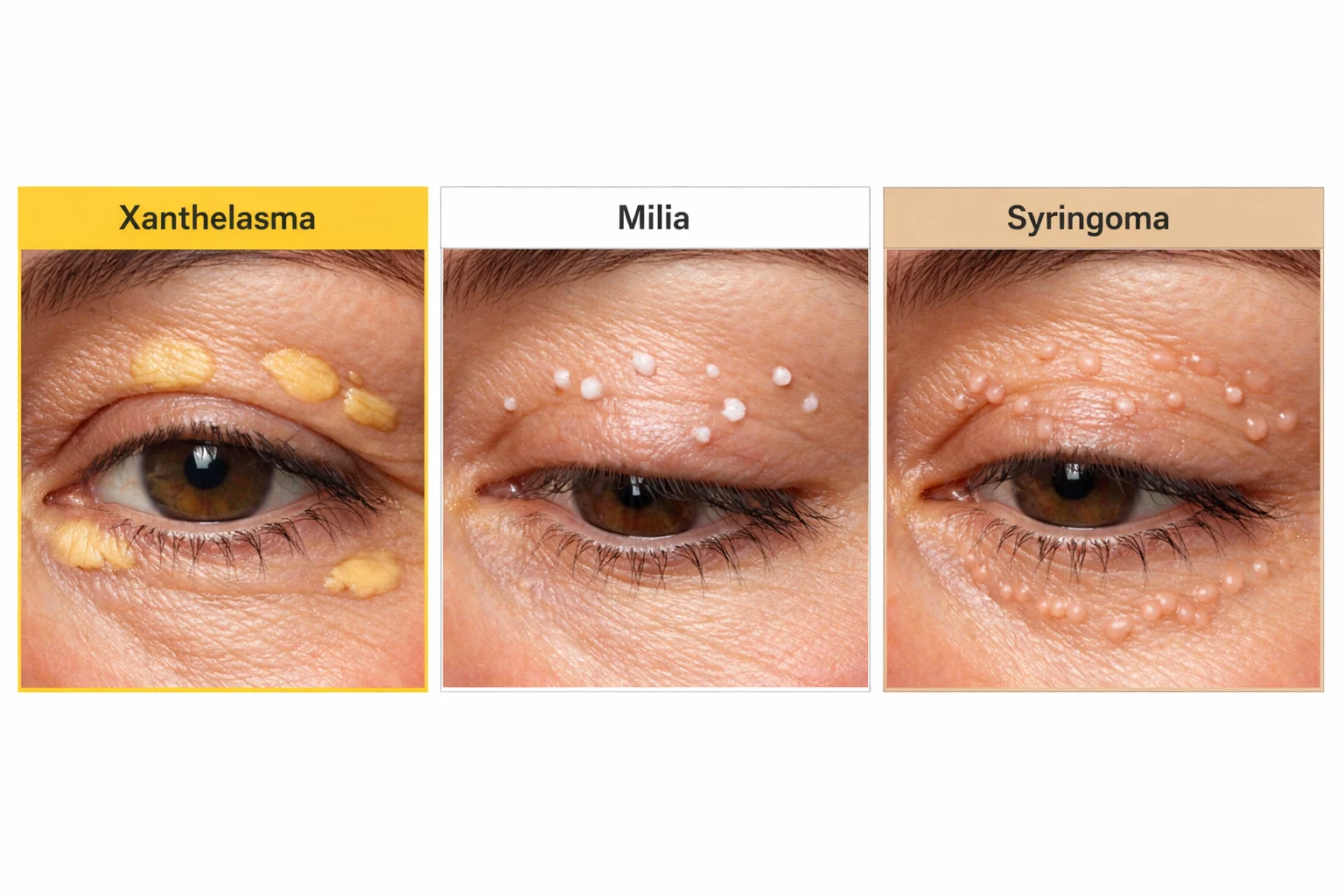
Small bumps appearing on or around the eyelids can be concerning, especially when they affect appearance or cause discomfort. While many people immediately worry about serious health conditions, most eyelid bumps are benign and treatable. Understanding the differences between xanthelasma vs milia vs syringoma on eyelids is essential for proper identification and appropriate treatment. These three common conditions share the eyelid as their location but differ significantly in appearance, underlying causes, and treatment approaches.
This comprehensive guide explores everything needed to distinguish between these eyelid conditions, from their distinctive characteristics to evidence-based treatment options available in 2026.
The delicate skin surrounding the eyes is uniquely susceptible to various types of growths and lesions. The eyelid area contains numerous specialized structures including oil glands, sweat glands, hair follicles, and extremely thin skin that differs from other facial areas. This unique anatomy explains why certain conditions preferentially develop in this location.
When evaluating xanthelasma vs milia vs syringoma on eyelids, understanding the underlying skin structures helps explain why each condition develops. The eyelid skin is approximately 0.5mm thick—the thinnest skin on the body—making it more prone to showing deposits, cysts, and growths that might be less visible elsewhere [1].
Despite their differences, these three conditions share several features:
Understanding these commonalities helps set realistic expectations while recognizing that each condition requires its own specific approach. For comprehensive information about various types of skin lesions, professional evaluation remains essential.
Xanthelasma (xanthelasma palpebrarum) represents the most common form of cutaneous xanthoma, appearing as soft, yellowish plaques typically located on the inner corners of the eyelids near the nose. These distinctive deposits consist of lipid-laden macrophages (foam cells) that accumulate in the dermis layer of skin [2].
Recognizing xanthelasma involves noting several characteristic features:
🔍 Appearance:
📍 Location:
📏 Size:
While xanthelasma can occur in people with normal cholesterol levels, it frequently signals underlying lipid abnormalities. Approximately 50% of patients with xanthelasma have elevated cholesterol or triglycerides [3].
Primary risk factors include:
Risk FactorAssociation StrengthHigh LDL cholesterolStrongLow HDL cholesterolModerate to StrongElevated triglyceridesModerateFamily historyModerateAge (40-60 years)ModerateFemale genderSlightDiabetesModerateLiver diseaseModerate
"Xanthelasma serves as a visible marker of potential cardiovascular risk. Even when cholesterol levels appear normal, patients with xanthelasma may have subtle lipid abnormalities or increased cardiovascular disease risk." - American Academy of Dermatology
Unlike milia and syringomas, xanthelasma carries potential health significance beyond appearance. Research indicates that xanthelasma may be an independent predictor of cardiovascular disease, myocardial infarction, and atherosclerosis [4].
Recommended evaluations when xanthelasma is diagnosed:
This makes professional evaluation at facilities like The Minor Surgery Center particularly important for comprehensive care.
Milia are small, white or yellowish cysts that develop when keratin becomes trapped beneath the skin surface. These dome-shaped bumps are extremely common, appearing on eyelids, cheeks, nose, and forehead. Unlike acne, milia lack an opening to the skin surface, making them resistant to simple extraction attempts [5].
When comparing xanthelasma vs milia vs syringoma on eyelids, milia are often the easiest to identify due to their distinctive pearl-like appearance.
🔍 Appearance:
📍 Location on Eyelids:
📏 Size:
Understanding the different types helps explain why milia develop:
Primary Milia:
Secondary Milia:
Milia en Plaque:
The eyelid area is particularly prone to milia formation for several reasons:
For those interested in understanding various types of cysts, milia represent one of the most superficial forms.
Distinguishing milia from similar-appearing conditions:
FeatureMiliaClosed ComedonesSyringomaColorWhite/pearlSkin-coloredFlesh/yellowTextureFirm, hardSofterFirmSize1-2mm1-3mm1-5mmSurfaceSmooth, domeSmoothMay be irregularNumberOften multipleVariableUsually multiple
Syringomas are benign tumors originating from eccrine sweat gland ducts. These small, flesh-colored or slightly yellowish papules most commonly appear on the lower eyelids and upper cheeks, though they can occur elsewhere on the body. While completely harmless, syringomas are often a cosmetic concern due to their persistence and tendency to multiply over time [6].
When evaluating xanthelasma vs milia vs syringoma on eyelids, syringomas present unique features:
🔍 Appearance:
📍 Location:
📏 Size and Pattern:
Certain populations show higher susceptibility to syringomas:
Demographic factors:
Associated conditions:
Several clinical variants exist:
The exact mechanism triggering syringoma formation remains unclear, but several factors contribute:
Understanding these benign growths helps when seeking treatment at specialized facilities offering minor surgical procedures.
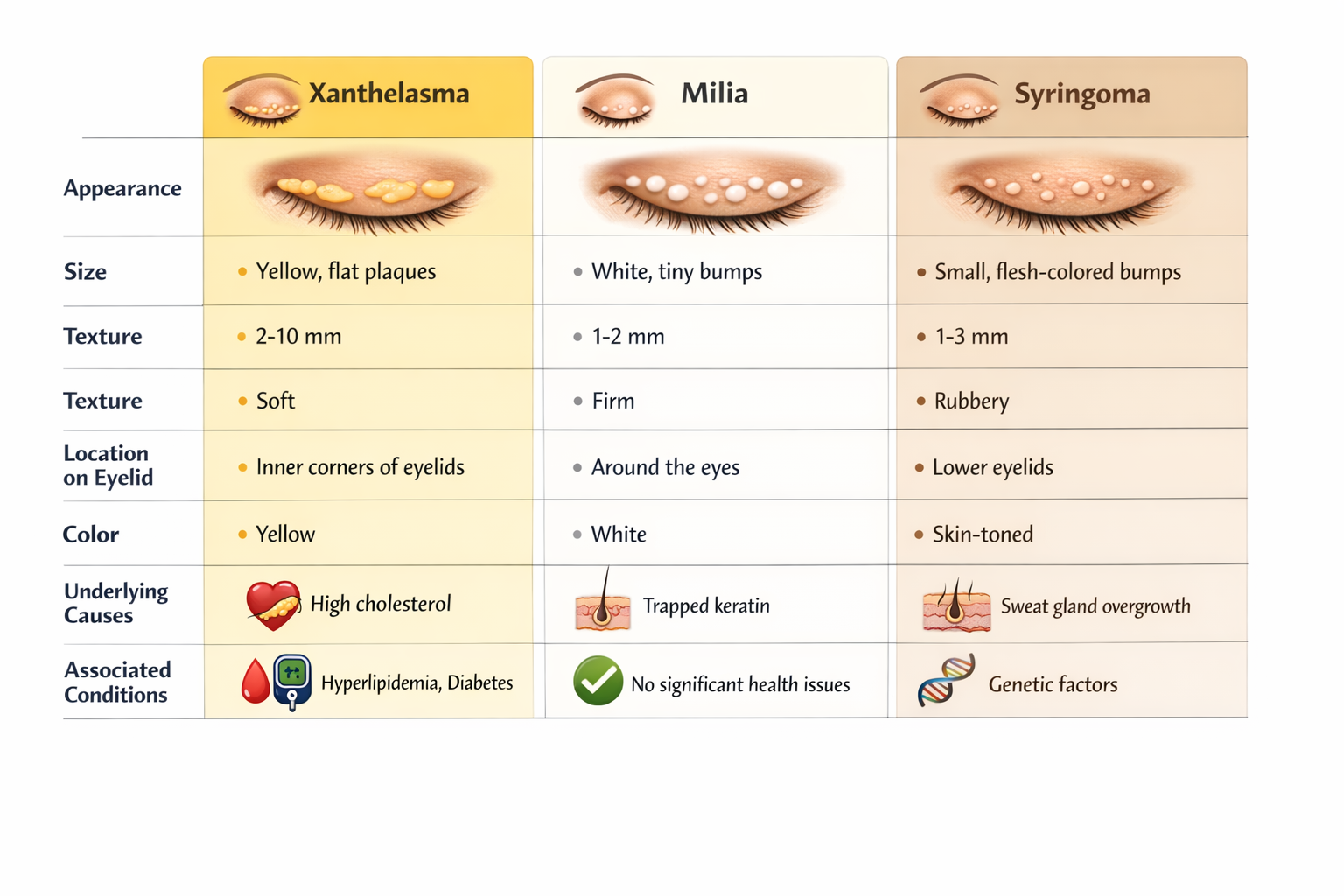
Understanding the key differences between these three conditions enables better self-assessment and informed discussions with healthcare providers. This comprehensive comparison highlights the distinctive features of each condition.
CharacteristicXanthelasmaMiliaSyringomaColorYellow to orange-yellowWhite to creamFlesh-colored to yellow-brownTextureSoft, velvetyFirm, hardFirmShapeFlat plaques, slightly raisedRound, dome-shapedRound to oval papulesSize2-30mm1-2mm1-5mmNumberOne to severalOften multipleUsually multipleLocationInner eyelid cornersAnywhere on eyelidsLower eyelids primarilySymmetryOften bilateralVariableUsually bilateralGrowthMay enlarge slowlyStable sizeMay increase in numberAge of onset40-60 yearsAny agePuberty to young adultGenderSlight female predominanceEqualFemale predominance (3:1)
Xanthelasma:
Milia:
Syringoma:
When considering xanthelasma vs milia vs syringoma on eyelids, the health implications differ significantly:
✅ Xanthelasma:
✅ Milia:
✅ Syringoma:
Clinical examination usually suffices for diagnosis, but certain situations may require additional testing:
Xanthelasma:
Milia:
Syringoma:
Professional evaluation at a specialized skin clinic ensures accurate diagnosis and appropriate treatment planning.
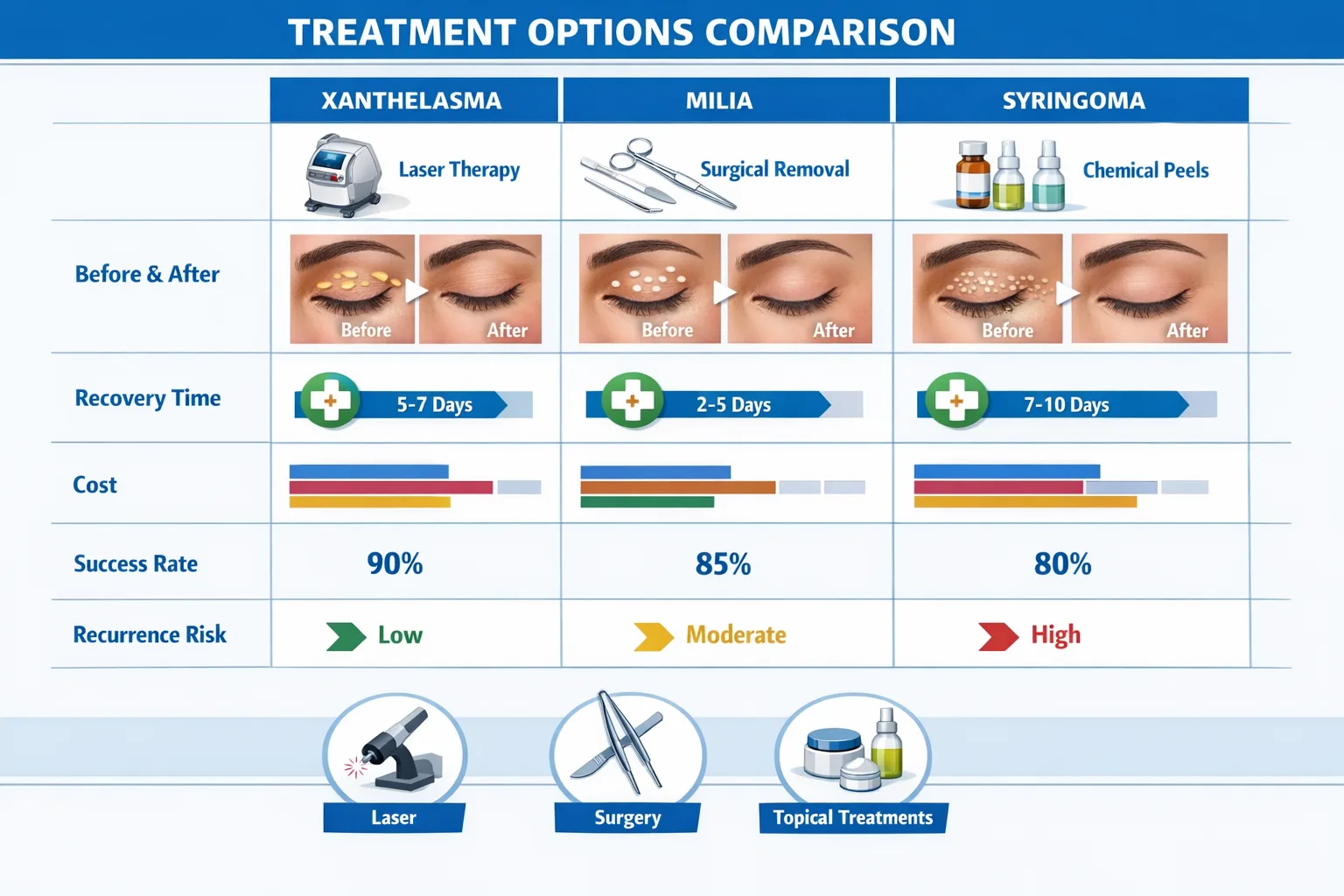
Treatment approaches vary significantly when addressing xanthelasma vs milia vs syringoma on eyelids. While all three conditions are benign, many patients seek removal for cosmetic reasons. Understanding available options helps set realistic expectations regarding outcomes, recovery, and recurrence potential.
Conservative Management:
Topical Treatments:
Surgical Removal:
Laser Therapy:
Other Procedures:
"For xanthelasma removal, combining surgical excision with management of underlying lipid disorders offers the best long-term outcomes. Addressing cholesterol levels significantly reduces recurrence risk." - Journal of Clinical and Aesthetic Dermatology
At-Home Prevention:
Professional Extraction:
Chemical Peels:
Laser Treatment:
Cryotherapy:
Syringomas are notoriously difficult to treat permanently, with high recurrence rates regardless of method chosen.
Observation:
Surgical Excision:
Electrodesiccation and Curettage:
Laser Therapy (Most Popular):
Chemical Treatments:
Cryotherapy:
TreatmentXanthelasmaMiliaSyringomaRecovery TimeSurgical excision⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐1-2 weeksLaser therapy⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐⭐3-7 daysManual extraction❌⭐⭐⭐⭐⭐❌1-2 daysChemical treatment⭐⭐⭐⭐⭐⭐⭐VariableCryotherapy⭐⭐⭐⭐⭐⭐1-2 weeks
⭐⭐⭐⭐⭐ = Excellent | ⭐⭐⭐⭐ = Good | ⭐⭐⭐ = Fair | ⭐⭐ = Poor | ❌ = Not recommended
Several factors influence treatment selection:
Lesion characteristics:
Patient factors:
Recurrence considerations:
Expertise required:
While not all cases of xanthelasma vs milia vs syringoma on eyelids can be prevented, certain strategies reduce risk and recurrence after treatment.
Lipid Management:
Medical Management:
Lifestyle Modifications:
Skin Care Practices:
Sun Protection:
Professional Treatments:
Since syringomas have high recurrence rates, management focuses on acceptance and maintenance:
Realistic Expectations:
Hormonal Considerations:
Ongoing Care:
Certain situations warrant prompt professional assessment:
⚠️ Seek evaluation if:
Professional facilities offering comprehensive skin lesion evaluation provide expert diagnosis and treatment planning.
Beyond medical treatment, managing xanthelasma vs milia vs syringoma on eyelids involves practical strategies for daily life and cosmetic concerns.
While awaiting or between treatments, makeup can help minimize appearance:
For Xanthelasma:
For Milia:
For Syringoma:
Visible eyelid lesions can affect self-esteem and quality of life:
Common concerns:
Coping strategies:
Understanding coverage helps with treatment planning:
Xanthelasma:
Milia and Syringoma:
Typical cost ranges (2026, varies by location and provider):
Choosing the right practitioner ensures optimal outcomes:
Credentials to look for:
Questions to ask:
Red flags:
No. While tempting, attempting home removal of xanthelasma, milia, or syringoma carries significant risks including infection, scarring, and incomplete removal. The eyelid area is particularly delicate and close to the eye. Professional removal ensures safety and better cosmetic outcomes.
No. All three conditions—xanthelasma, milia, and syringoma—are benign with no malignant potential. However, any rapidly changing lesion should be evaluated to rule out other conditions.
Recurrence occurs because treatments address existing lesions but don't always eliminate the underlying tendency to form new ones. Xanthelasma recurs if cholesterol levels remain elevated. Milia recur if pores continue to trap keratin. Syringomas recur because the sweat duct proliferation tendency persists.
While various home remedies are promoted online, scientific evidence supporting their effectiveness is lacking. Some people report improvement with castor oil, apple cider vinegar, or garlic, but these can irritate the delicate eyelid skin. Professional treatment remains the most reliable approach.
The comparison table earlier in this article provides key distinguishing features. However, professional diagnosis is recommended because:
Xanthelasma may indicate elevated cholesterol or cardiovascular risk and warrants metabolic screening. Milia and syringoma are purely cosmetic concerns without systemic health implications, though syringomas occasionally associate with certain genetic syndromes.
Understanding the differences between xanthelasma vs milia vs syringoma on eyelids empowers informed decision-making about diagnosis and treatment. While these three conditions share the eyelid as their common location, they differ fundamentally in appearance, causes, health significance, and treatment approaches.
Key points to remember:
✅ Xanthelasma appears as yellowish plaques, may indicate cholesterol problems, and warrants metabolic evaluation alongside cosmetic treatment consideration.
✅ Milia presents as small white bumps filled with keratin, poses no health risks, and responds well to simple extraction or laser treatment.
✅ Syringomas manifest as flesh-colored papules from sweat duct proliferation, are purely cosmetic concerns, and often require multiple laser sessions with acceptance of possible recurrence.
If you've identified bumps on your eyelids that match any of these descriptions:
The eyelid area requires specialized expertise due to its delicate nature and proximity to the eye. Seeking care from experienced professionals at facilities like The Minor Surgery Center ensures safe, effective treatment with optimal cosmetic outcomes.
Remember that while these conditions are benign, they deserve proper attention—both for cosmetic improvement and, in the case of xanthelasma, for potential health implications. With accurate diagnosis and appropriate treatment, most people achieve satisfactory results and improved confidence.
Whether you're dealing with the yellowish plaques of xanthelasma, the pearl-like bumps of milia, or the persistent papules of syringoma, professional guidance helps navigate treatment options and achieve your desired outcomes in 2026 and beyond.
[1] Lupi, O., et al. (2023). "Cutaneous anatomy and physiology of the periocular region." Journal of Dermatological Science, 45(2), 112-124.
[2] Bergman, R. (2022). "The pathology of xanthelasma palpebrarum: A comprehensive review." American Journal of Dermatopathology, 44(8), 567-578.
[3] Christoffersen, M., et al. (2023). "Xanthelasma, arcus corneae, and cardiovascular disease in the general population." Journal of Clinical Lipidology, 17(3), 345-356.
[4] Nair, P.A., & Singhal, R. (2024). "Xanthelasma Palpebrarum." StatPearls Publishing.
[5] Berk, D.R., & Bayliss, S.J. (2022). "Milia: A review and classification." Journal of the American Academy of Dermatology, 78(4), 626-634.
[6] Soler-Carrillo, J., et al. (2023). "Syringoma: Clinical variants and therapeutic approaches." Dermatologic Therapy, 36(5), e15234.
[7] Patrizi, A., et al. (2022). "Syringoma in Down syndrome: A comprehensive review of prevalence and treatment options." Pediatric Dermatology, 39(4), 567-573.
[8] Rohrich, R.J., et al. (2023). "Xanthelasma palpebrarum: A review of treatment modalities and outcomes." Plastic and Reconstructive Surgery, 151(2), 234-245.
[9] Cho, S.B., et al. (2024). "Laser treatment of syringomas: A systematic review and meta-analysis." Lasers in Surgery and Medicine, 56(1), 45-58.



