Subchondral Bone Cysts in Arthritis: What They Mean for Your Joints
When joint pain becomes a constant companion, understanding what's happening beneath the surface becomes crucial. Subchondral bone cysts in arthritis represent one of the hidden changes occurring deep within your joints—changes that can significantly impact your mobility, comfort, and quality of life. These fluid-filled pockets that form in the bone just beneath the cartilage tell an important story about joint health and the progression of arthritic conditions.
For millions of adults living with arthritis in 2025, subchondral cysts are more than just medical terminology—they're a reality that affects daily activities, from climbing stairs to opening jars. Understanding what these cysts are, why they develop, and what they mean for your joint health empowers you to make informed decisions about treatment and management strategies.
Key Takeaways
Subchondral bone cysts are fluid-filled pockets that develop in the bone directly beneath joint cartilage, commonly associated with osteoarthritis and rheumatoid arthritis
These cysts form due to increased pressure and mechanical stress on damaged joints, where synovial fluid is forced through cartilage defects into the underlying bone
Larger cysts can weaken bone structure and contribute to joint pain, stiffness, and reduced mobility, though smaller cysts may not cause noticeable symptoms
Early detection through imaging (X-rays, MRI, CT scans) allows for better treatment planning and can help prevent further joint deterioration
Treatment approaches range from conservative management (medication, physical therapy, lifestyle modifications) to surgical interventions depending on cyst size, location, and symptom severity
Understanding Subchondral Bone Cysts in Arthritis: The Basics
What Are Subchondral Bone Cysts?
Subchondral bone cysts, also called geodes or pseudocysts, are fluid-filled cavities that develop within the bone tissue located just beneath the cartilage surface of joints. The term "subchondral" literally means "below the cartilage," referring to the layer of bone that provides crucial support to the smooth cartilage covering joint surfaces[1].
Unlike other types of cysts that may develop in soft tissues throughout the body, subchondral cysts specifically form within bone tissue and are closely linked to joint disease. These structures typically contain:
Synovial fluid (the lubricating fluid normally found in joint spaces)
Mucoid material (thick, gel-like substances)
Fibrous tissue (connective tissue elements)
Bone fragments (in some cases)
The cysts can range dramatically in size, from tiny lesions barely visible on imaging to large cavities measuring several centimeters in diameter. They most commonly appear in weight-bearing joints such as:
🦵 Knees (most frequent location)
🦴 Hips
🦶 Ankles
🤚 Hands and wrists
🔄 Spine (facet joints)
The Anatomy Behind the Problem
To understand subchondral bone cysts in arthritis, it's essential to grasp the normal structure of healthy joints. A typical synovial joint consists of several key components:
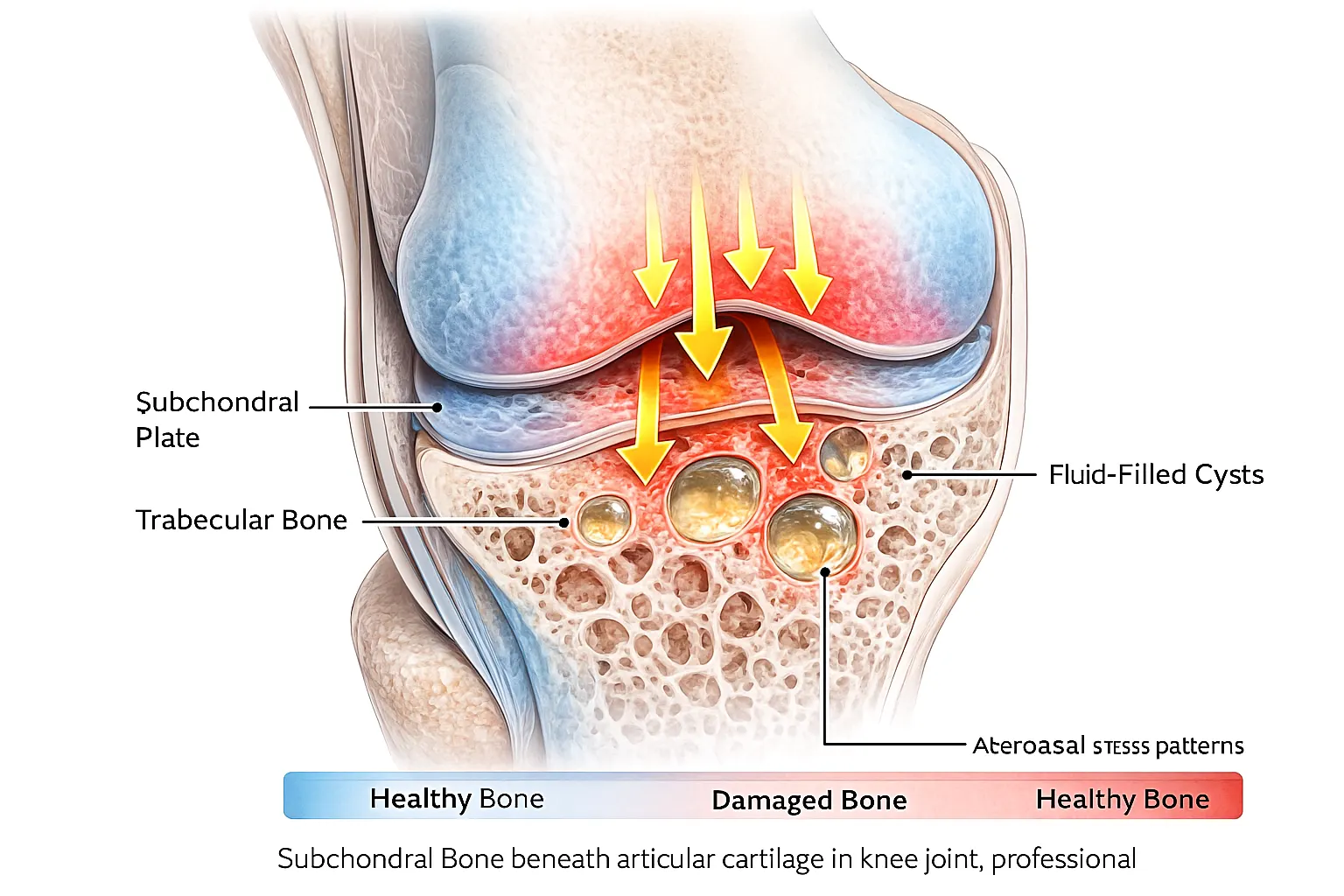
Joint ComponentFunctionRole in Cyst FormationArticular CartilageProvides smooth, friction-free movementDamage creates pathways for fluid penetrationSubchondral PlateThin layer of dense bone beneath cartilageBecomes compromised, allowing cyst developmentTrabecular BoneSpongy bone with interconnected spacesSite where cysts actually form and expandSynovial MembraneProduces lubricating joint fluidSource of fluid that fills cystsJoint CapsuleEncloses and stabilizes the jointContains increased pressure in diseased joints
In healthy joints, the subchondral bone plate acts as a protective barrier. However, when arthritis damages the cartilage above, this protective system breaks down, creating conditions favorable for cyst formation[2].
What Causes Bone Cysts in Adults: The Mechanisms Explained
Primary Theories of Cyst Formation
Medical researchers have identified several mechanisms that explain what causes bone cysts in adults, particularly in the context of arthritis. The two predominant theories are:
1. The Synovial Fluid Intrusion Theory 💧
This widely accepted explanation suggests that subchondral cysts form when:
Arthritis damages and thins the protective cartilage layer
Cracks and fissures develop in the remaining cartilage
Joint movement creates hydraulic pressure within the joint space
Synovial fluid is forcefully pushed through cartilage defects
The fluid penetrates the subchondral bone plate
Repeated pressure cycles cause the fluid to accumulate in bone tissue
A cyst cavity gradually expands as more fluid enters
This mechanism is particularly relevant in osteoarthritis, where mechanical wear-and-tear creates the initial cartilage damage[3].
2. The Bone Contusion and Remodeling Theory 🔨
An alternative explanation focuses on direct bone trauma:
Repetitive impact on damaged joints causes bone bruising
Microfractures develop in the subchondral bone
The body's healing response is inadequate or abnormal
Instead of proper bone repair, fluid-filled spaces form
Inflammatory mediators contribute to bone resorption
Cystic spaces develop as bone tissue breaks down
This theory is especially applicable to rheumatoid arthritis and other inflammatory joint conditions[4].
Risk Factors for Developing Subchondral Cysts
Understanding what increases your risk for developing these bone changes helps with prevention and early intervention:
Cartilage loss – Greater cartilage damage means more vulnerability
Mechanical Factors:
Obesity – Excess weight increases load on weight-bearing joints
Joint malalignment – Knock-knees or bow-legs concentrate stress unevenly
Repetitive impact activities – Running, jumping, or heavy lifting
Previous joint injuries – Old trauma predisposes to arthritis and cysts
Demographic Factors:
Age over 50 – Cumulative joint wear increases with time
Female gender – Women have higher rates of certain arthritic conditions
Genetic predisposition – Family history of arthritis increases risk
Occupational demands – Jobs requiring prolonged kneeling or heavy lifting
Subchondral Bone Cysts in Arthritis: Types and Locations
Cysts in Osteoarthritis vs. Rheumatoid Arthritis
The characteristics of subchondral bone cysts in arthritis vary depending on the underlying arthritic condition:
Osteoarthritis-Associated Cysts:
Typically larger in size
Usually fewer in number
Located in areas of maximum weight-bearing stress
Associated with bone sclerosis (increased bone density around cyst)
Often accompanied by osteophytes (bone spurs)
Progress more slowly over time
Rheumatoid Arthritis-Associated Cysts:
Generally smaller and more numerous
Distributed more symmetrically across joints
Associated with bone erosions rather than sclerosis
Accompanied by soft tissue swelling and inflammation
May progress more rapidly during disease flares
Often present in multiple joints simultaneously
Common Joint Locations and Their Implications
Knee Joint Cysts 🦵
The knee is the most frequent site for subchondral cysts, particularly in the:
Medial femoral condyle (inner thigh bone)
Tibial plateau (top of shin bone)
Patellofemoral joint (behind the kneecap)
Clinical significance: Large knee cysts can significantly limit mobility, cause pain with weight-bearing, and increase the risk of subchondral bone collapse.
Hip Joint Cysts 🦴
Hip cysts commonly develop in:
Femoral head (ball of the hip joint)
Acetabulum (hip socket)
Clinical significance: Hip cysts can be particularly problematic, sometimes necessitating joint replacement surgery when they compromise bone integrity.
Hand and Wrist Cysts 🤚
Smaller joints of the hands frequently show cysts in:
Distal interphalangeal joints (finger joints nearest the nails)
Carpometacarpal joint of the thumb
Clinical significance: While typically smaller, hand cysts can significantly impact fine motor skills and grip strength. For information about other hand conditions, explore our resources on carpal tunnel and arthritis.
Symptoms and Clinical Presentation
How Subchondral Cysts Affect Joint Function
Many people with subchondral bone cysts experience a range of symptoms, though some smaller cysts remain asymptomatic and are discovered incidentally on imaging studies. Common manifestations include:
Pain Characteristics:
🔴 Deep, aching pain within the joint
🔴 Worsening with activity and weight-bearing
🔴 Night pain that disrupts sleep
🔴 Pain with specific movements that stress the affected area
🔴 Sudden sharp pain if a cyst causes bone collapse
Functional Limitations:
⚠️ Reduced range of motion
⚠️ Joint stiffness, especially after rest
⚠️ Difficulty with stairs (for knee/hip cysts)
⚠️ Weakness in the affected limb
⚠️ Instability or feeling that the joint might "give way"
Physical Findings:
👁️ Joint swelling and effusion (fluid accumulation)
👁️ Tenderness over the cyst location
👁️ Crepitus (grinding or crackling sensation)
👁️ Deformity in advanced cases
👁️ Muscle atrophy around the affected joint
When Cysts Become Problematic
Not all subchondral cysts cause significant problems. Several factors determine clinical impact:
Size Matters:
Cysts smaller than 5mm often remain asymptomatic
Cysts between 5-10mm may cause intermittent symptoms
Cysts larger than 10mm typically produce noticeable symptoms
Very large cysts (>20mm) can compromise bone structural integrity
Location Determines Impact:
Cysts in weight-bearing areas cause more symptoms
Cysts near joint margins may limit movement more
Multiple cysts in one joint compound the problem
Cysts in non-weight-bearing areas may be better tolerated
Complications to Watch For:
Subchondral bone collapse – Cyst weakens bone, leading to fracture
Rapid cyst expansion – Indicates active disease progression
Infection – Rare but serious complication requiring urgent treatment
Nerve compression – Large cysts may impinge on nearby nerves
Diagnosis: Detecting Subchondral Bone Cysts in Arthritis
Clinical Examination
The diagnostic process begins with a thorough clinical evaluation:
Medical History Assessment:
Duration and pattern of joint symptoms
Previous joint injuries or surgeries
Family history of arthritis
Occupational and recreational activities
Response to previous treatments
Presence of other arthritic symptoms
Physical Examination:
Joint inspection for swelling, deformity, or asymmetry
Palpation to identify tender areas
Range of motion testing
Stability assessment
Gait analysis (for lower extremity joints)
Muscle strength evaluation
Imaging Studies: The Gold Standard
Definitive diagnosis of subchondral bone cysts in arthritis requires imaging studies:
X-Rays (Radiography) 📸
Advantages:
Widely available and cost-effective
Excellent for detecting larger cysts
Shows associated arthritic changes (joint space narrowing, osteophytes)
Useful for monitoring progression over time
Limitations:
May miss small or early cysts
Two-dimensional view can underestimate cyst size
Limited soft tissue detail
Typical X-ray Findings:
Well-defined radiolucent areas (dark spots) in bone
Usually located near joint surfaces
May have sclerotic margins (white rim around cyst)
Associated signs of arthritis present
Magnetic Resonance Imaging (MRI) 🧲
Advantages:
Superior soft tissue contrast
Detects smaller cysts not visible on X-rays
Reveals bone marrow edema and cartilage damage
Can differentiate cyst contents
No radiation exposure
Limitations:
More expensive than X-rays
Longer examination time
Not suitable for patients with certain metal implants
May not be readily available in all settings
MRI Characteristics:
Cysts appear as bright (hyperintense) signals on T2-weighted images
Dark (hypointense) signals on T1-weighted images
Surrounding bone marrow edema often visible
Detailed cartilage assessment possible
Computed Tomography (CT) Scans 💻
Advantages:
Excellent bone detail
Precise measurement of cyst size and location
Useful for surgical planning
Can create 3D reconstructions
Limitations:
Radiation exposure
Less detailed soft tissue information than MRI
Higher cost than X-rays
CT Findings:
Clear delineation of cyst boundaries
Accurate assessment of bone quality
Identification of subchondral bone plate integrity
Detection of associated fractures or collapse
Laboratory Tests
While imaging confirms cyst presence, blood tests help identify the underlying arthritic condition:
Rheumatoid factor (RF) – Elevated in rheumatoid arthritis
Anti-CCP antibodies – Specific for rheumatoid arthritis
Targeted anti-inflammatory agents – Precision medicine for arthritis
Bone metabolism modulators – Influence cyst formation and healing
Cartilage protective agents – Prevent further joint damage
Living with Subchondral Bone Cysts: Long-Term Management
Monitoring and Follow-Up
Regular monitoring ensures optimal management of subchondral bone cysts in arthritis:
Imaging Follow-Up Schedule:
Baseline imaging at diagnosis
Repeat imaging at 6-12 months for active symptoms
Annual imaging for stable, asymptomatic cysts
Immediate imaging if symptoms suddenly worsen
Clinical Assessments:
Regular appointments with rheumatologist or orthopedist
Functional assessment questionnaires
Pain and symptom tracking
Medication effectiveness evaluation
Physical therapy progress reviews
Preventing Progression
While you cannot always prevent cyst formation, several strategies may slow progression:
Optimize Arthritis Management:
Maintain consistent medication adherence
Control inflammatory arthritis activity
Regular follow-up with healthcare providers
Promptly address disease flares
Protect Your Joints:
Maintain healthy body weight
Engage in appropriate exercise
Use proper body mechanics
Avoid joint trauma
Modify high-risk activities
Support Overall Health:
Eat an anti-inflammatory diet rich in omega-3 fatty acids, fruits, and vegetables
Get adequate sleep for tissue repair
Manage stress effectively
Avoid smoking, which impairs bone healing
Limit alcohol consumption
Impact on Quality of Life
Understanding the broader implications helps patients and families prepare:
Physical Impact:
May limit participation in favorite activities
Can affect work capacity and productivity
Influences independence in daily tasks
May require home modifications
Emotional and Psychological Considerations:
Chronic pain can contribute to depression and anxiety
Uncertainty about progression causes stress
Body image concerns with joint deformity
Social isolation due to mobility limitations
Coping Strategies:
Join support groups for people with arthritis
Work with mental health professionals when needed
Maintain social connections and activities
Focus on abilities rather than limitations
Celebrate small victories in symptom management
For comprehensive information about various health conditions and treatments, visit The Minor Surgery Center and explore our blog for additional resources.
Special Considerations for Different Patient Populations
Younger Adults with Subchondral Cysts
When cysts develop in people under 50:
Unique Challenges:
Greater impact on career and family responsibilities
Longer disease duration ahead
Higher activity demands
Concerns about joint replacement longevity
Management Priorities:
Aggressive arthritis control to slow progression
Joint preservation strategies emphasized
Consideration of activity modification
Planning for potential future surgeries
Psychological support for chronic disease at young age
Molecular biology research identifying biochemical pathways
Biomechanical modeling of joint stress patterns
Genetic studies exploring predisposition factors
Treatment Innovation:
Clinical trials of regenerative medicine approaches
Development of targeted drug therapies
Refinement of surgical techniques
Investigation of combination treatment strategies
Promising Future Therapies
Several exciting developments may change cyst management:
Precision Medicine:
Genetic profiling to predict cyst risk
Personalized treatment based on individual biology
Biomarkers to monitor treatment response
Targeted therapies for specific cyst types
Advanced Imaging:
Artificial intelligence analysis of imaging studies
Quantitative imaging biomarkers
Improved early detection capabilities
Non-invasive monitoring techniques
Tissue Engineering:
Bioengineered cartilage replacement
Advanced scaffold materials
Growth factor delivery systems
3D-printed bone grafts
The Role of Technology
Modern technology enhances cyst management:
Digital Health Tools:
Mobile apps for symptom tracking
Telemedicine consultations
Wearable devices monitoring activity levels
Online patient education resources
Surgical Advances:
Robotic-assisted procedures
Computer navigation systems
Minimally invasive techniques
Enhanced visualization technologies
Frequently Asked Questions
Can subchondral bone cysts heal on their own?
Small cysts occasionally stabilize or improve with conservative treatment, but complete spontaneous resolution is uncommon. The underlying arthritis typically continues to progress, and most cysts either remain stable or slowly enlarge over time. Effective arthritis management offers the best chance for cyst stabilization.
Are subchondral cysts cancerous?
No, subchondral bone cysts are benign (non-cancerous) lesions. They represent a response to joint disease rather than a tumor. However, if imaging shows atypical features, additional testing may be recommended to rule out other conditions.
How fast do these cysts grow?
Growth rates vary considerably depending on arthritis activity, mechanical stress, and individual factors. Some cysts remain stable for years, while others expand relatively quickly over months. Regular imaging monitoring helps track progression and guide treatment decisions.
Will I need surgery?
Most patients manage successfully with conservative treatments. Surgery becomes necessary when:
Pain and disability significantly impact quality of life
Cysts threaten bone structural integrity
Conservative treatments have failed
Joint damage is severe
Your healthcare provider will help determine the most appropriate approach for your specific situation.
Can I prevent subchondral cysts from forming?
While you cannot guarantee prevention, several strategies reduce risk:
Maintain healthy body weight
Engage in joint-friendly exercise
Protect joints from injury
Manage arthritis effectively
Address joint problems early
Early and aggressive arthritis treatment offers the best opportunity to minimize cyst development.
Conclusion
Subchondral bone cysts in arthritis represent a significant manifestation of joint disease that affects millions of people worldwide. These fluid-filled cavities developing beneath damaged cartilage tell an important story about the health of your joints and the progression of arthritic conditions. Understanding what these cysts are, why they form, and how they impact joint function empowers you to take an active role in managing your joint health.
From the mechanical stress theories explaining what causes bone cysts in adults to the sophisticated imaging techniques that detect them, modern medicine offers comprehensive approaches to diagnosis and treatment. Whether through conservative management with medications, physical therapy, and lifestyle modifications, or through surgical interventions when necessary, effective options exist for addressing these challenging lesions.
The key to optimal outcomes lies in:
✅ Early detection through appropriate imaging when symptoms arise ✅ Comprehensive arthritis management to address the underlying disease ✅ Regular monitoring to track cyst progression and treatment response ✅ Personalized treatment plans tailored to your specific situation ✅ Proactive lifestyle modifications to protect joint health ✅ Open communication with your healthcare team about symptoms and concerns
Your Next Steps
If you're concerned about subchondral bone cysts or experiencing joint symptoms:
Schedule an evaluation with a rheumatologist or orthopedic specialist
Discuss imaging studies to assess your joint health comprehensively
Develop a treatment plan addressing both cysts and underlying arthritis
Implement lifestyle changes to support long-term joint health
Stay informed about new treatment developments and research
Remember that while subchondral bone cysts present challenges, they are manageable conditions. With appropriate medical care, lifestyle adjustments, and a proactive approach to joint health, most people successfully maintain function and quality of life. The field continues advancing, with promising new treatments on the horizon offering hope for even better outcomes in the future.
Your journey with arthritis and subchondral cysts is unique, but you don't have to navigate it alone. Work closely with your healthcare providers, stay engaged in your treatment plan, and remain optimistic about the possibilities for maintaining active, fulfilling lives despite these joint challenges.
References
[1] Crema MD, Roemer FW, Marra MD, et al. Articular cartilage in the knee: current MR imaging techniques and applications in clinical practice and research. Radiographics. 2011;31(1):37-61.
[2] Ondresik M, Azevedo Maia FR, da Silva Morais A, et al. Management of knee osteoarthritis. Current status and future trends. Biotechnology and Bioengineering. 2017;114(4):717-739.
[3] Roemer FW, Guermazi A, Javaid MK, et al. Change in MRI-detected subchondral bone marrow lesions is associated with cartilage loss: the MOST Study. A longitudinal multicentre study of knee osteoarthritis. Annals of the Rheumatic Diseases. 2009;68(9):1461-1465.
[4] McQueen FM, Benton N, Crabbe J, et al. What is the fate of erosions in early rheumatoid arthritis? Tracking individual lesions using x rays and magnetic resonance imaging over the first two years of disease. Annals of the Rheumatic Diseases. 2001;60(9):859-868.