Last updated: June 24, 2026
Quick Answer: Skin cancer on the scalp is more common and more dangerous than most people realize. The scalp receives intense, cumulative UV exposure, hair makes visual inspection difficult, and detection is often delayed as a result. The three main types are basal cell carcinoma, squamous cell carcinoma, and melanoma, each with distinct warning signs and treatment approaches. Early detection dramatically improves outcomes.
Scalp skin cancer is more prevalent than most people expect. The scalp and neck together account for a disproportionately high share of skin cancer cases relative to their surface area, because these areas receive direct, uninterrupted sun exposure throughout a person's lifetime [2].
Among all skin cancer sites, the scalp is particularly vulnerable for people who are bald or have thinning hair, spend significant time outdoors, or habitually skip sunscreen on their head. Older adults are at the highest risk, but scalp cancers can develop in younger adults with significant UV exposure histories.
Basal cell carcinoma is the most frequently diagnosed skin cancer overall, and the scalp is a common location. Squamous cell carcinoma (SCC) is the second most common type and is also frequently found on the scalp and ears. Melanoma accounts for a smaller percentage of cases but is responsible for the majority of skin cancer deaths, and scalp melanomas are considered especially high-risk [3].
Skin cancer on the scalp does not always look the same, and its appearance depends heavily on the cancer type. The key warning signs to recognize are listed below [2][4].
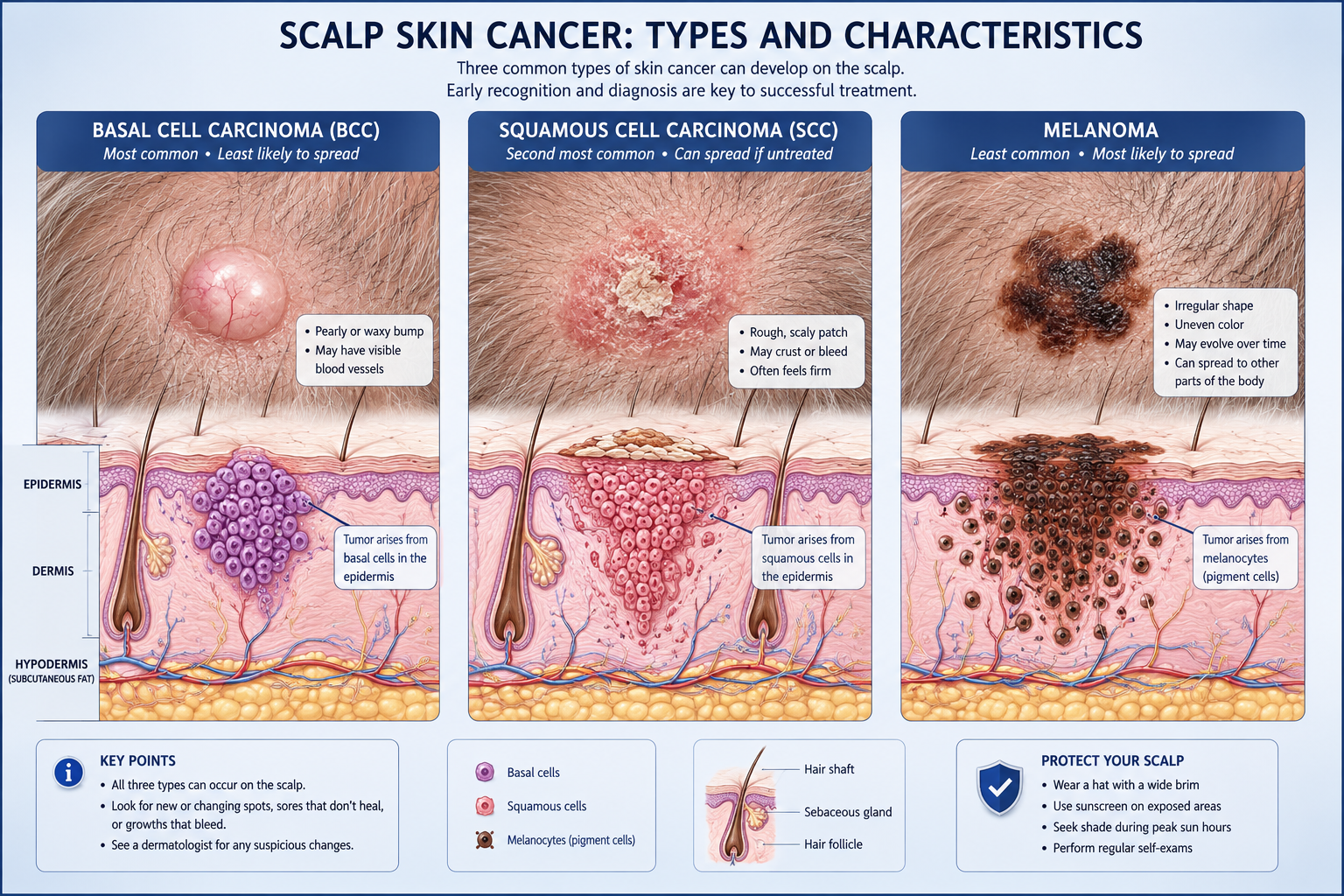
The ABCDE rule applies here: Asymmetry, Border irregularity, Color variation, Diameter larger than 6mm, and Evolution (any change over time) are all red flags for melanoma [2].
For a visual reference on early-stage presentations, see this guide to first stages of skin cancer pictures.
Yes, melanoma absolutely develops on the scalp, and it is one of the most dangerous locations for it to occur. Scalp melanoma accounts for a small but significant share of all melanoma diagnoses, and it carries a worse prognosis than melanoma on the arms, legs, or trunk [3].
The reasons scalp melanoma is particularly aggressive include:
For a detailed clinical overview of this topic, the melanoma on scalp guide covers staging, risk factors, and treatment in depth.
Most moles on the scalp are benign, but distinguishing a normal mole from a suspicious lesion is not always straightforward. Normal moles are typically round or oval, uniformly colored (one shade of brown), and stable in size over years. A scalp lesion that does not fit this profile warrants professional evaluation.
FeatureNormal MoleSuspicious LesionShapeRound or oval, symmetricalAsymmetrical, irregular edgesColorSingle shade of brown or tanMultiple colors or uneven toneSizeUsually under 6mmLarger than 6mm or growingSurfaceSmooth, consistentRough, crusted, or bleedingChange over timeStable for yearsChanging in weeks or monthsHealingN/ANon-healing sore or recurrent bleed
Any mole or growth on the scalp that bleeds without injury, itches persistently, or changes noticeably in a short period should be assessed by a physician. The article on dysplastic nevus explains atypical moles and when they require closer monitoring.
Scalp skin cancer is more dangerous than cancer in many other locations for several interconnected reasons [3][4].
Detection is harder. Hair covers the scalp, making routine visual checks difficult. Most people cannot see the top of their own scalp without mirrors and assistance, and many do not think to look. This means cancers often grow undetected for longer periods [4].
The scalp is highly vascularized. The dense blood supply that keeps hair follicles nourished also provides an efficient route for cancer cells to travel to lymph nodes and distant organs [3].
Thinner skin in some areas. Parts of the scalp have relatively thin skin over the skull, which means invasive cancers can reach deeper structures more quickly than in areas with more subcutaneous tissue.
Sun exposure is cumulative and often unprotected. Many people apply sunscreen to their face and arms but skip the scalp entirely, even during years of outdoor activity [1].
"Scalp melanomas have a higher mortality rate compared to melanomas on other body parts, attributed to the rich blood supply and delays in detection." [3]
Hair is the primary obstacle to early detection of scalp skin cancer. Even a thorough self-examination is limited by the fact that most people cannot part and inspect every section of their scalp without help [4].
Several factors compound this problem:
Who can help: Hairstylists are in a unique position to notice unusual scalp changes during routine cuts and washes. Encouraging a hairstylist to flag any unfamiliar bumps, sores, or color changes can serve as an informal but valuable screening layer between medical appointments [3].
Practical self-check tip: Use two mirrors (one handheld, one wall-mounted) and a comb to systematically part the hair in sections. Do this in good lighting every one to two months.
Hair loss alone is rarely a direct sign of scalp skin cancer, but localized, unexplained hair loss in a small, defined patch can occasionally be associated with an underlying lesion. Certain scalp cancers, particularly SCC, can cause scarring that destroys hair follicles and leads to permanent, localized alopecia.
More commonly, hair loss on the scalp is caused by alopecia areata, traction alopecia, fungal infections, or androgenetic alopecia. However, if hair loss is accompanied by a visible lesion, a sore that won't heal, or a firm lump beneath the skin, a medical evaluation is warranted.
For information on hair loss conditions unrelated to cancer, the alopecia treatment page provides a useful overview of common causes and options.
Diagnosis of scalp skin cancer follows a clear, stepwise process. A physician or dermatologist will typically begin with a visual examination using a dermatoscope, a handheld device that magnifies the skin and reveals subsurface patterns not visible to the naked eye [5].
If a lesion looks suspicious, the next step is a skin biopsy, which is the only definitive way to confirm a skin cancer diagnosis. During a biopsy, a small sample of tissue is removed from the lesion and sent to a pathology lab for analysis. Results typically return within one to two weeks.
Types of biopsy used for scalp lesions:
Once cancer is confirmed, staging tests (such as imaging or sentinel lymph node biopsy) may be ordered to determine whether the cancer has spread. For those in Ontario, resources on how long it takes to get biopsy results can help set expectations during the waiting period.
Treatment for skin cancer on the scalp depends on the cancer type, size, depth, and whether it has spread. Most scalp skin cancers are treated surgically, but several other approaches are used depending on the clinical situation [2].
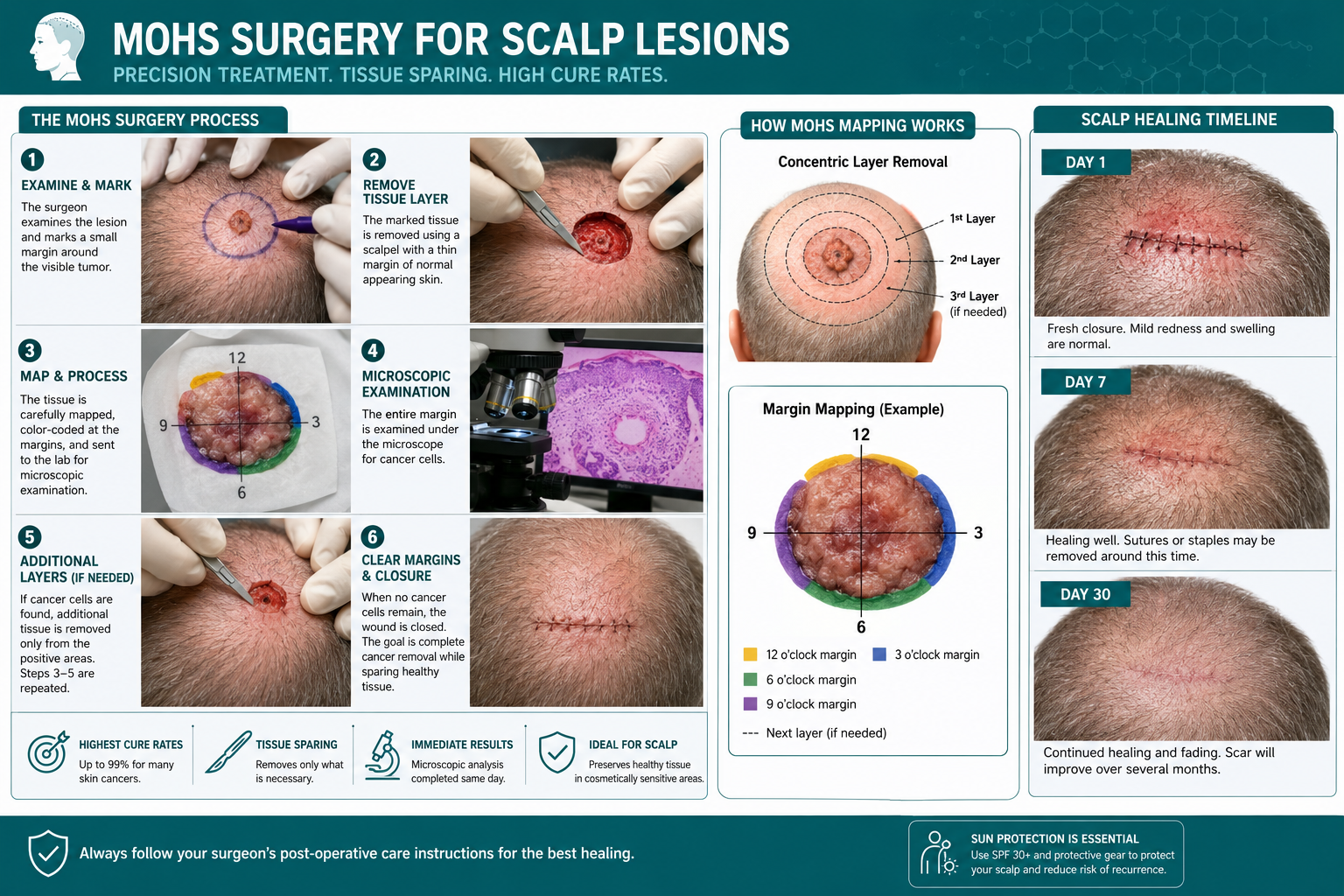
BCC on the scalp responds well to Mohs surgery, with cure rates exceeding 99% for primary (first-time) lesions. Smaller, superficial BCCs may also be treated with:
For a comparison of BCC and SCC treatment approaches, see BCC vs. SCC: What's the Difference.
Melanoma on the scalp typically requires wide local excision with larger margins than BCC or SCC. Depending on depth and staging, treatment may also include:
For a comprehensive breakdown of surgical approaches to melanoma, the melanoma surgery full guide covers each step in detail.
Recovery after scalp skin cancer removal depends on the size of the lesion and the surgical method used. Most patients undergoing standard excision or Mohs surgery on the scalp can expect the following general timeline:
Larger defects may require a skin flap or graft, which extends recovery. Patients should avoid strenuous activity, direct sun on the wound, and blood-thinning medications (as directed) during the healing period.
Common mistake: Returning to outdoor activities without protecting the healing scalp from sun exposure. This can worsen scarring and increase the risk of a new lesion forming nearby.
Prognosis for scalp skin cancer is strongly tied to the type of cancer and the stage at which it is diagnosed. Early-stage detection consistently produces the best outcomes [5].
Basal cell carcinoma: BCC almost never spreads to other organs. When treated promptly, the five-year cure rate with Mohs surgery exceeds 99% for primary lesions. Even recurrent BCC has a cure rate above 94% with Mohs [2].
Squamous cell carcinoma: SCC has a low metastasis rate when caught early (under 5% for localized disease), but scalp SCC carries a slightly higher risk of spread than SCC on the trunk or limbs due to lymphatic drainage patterns [6].
Melanoma: Prognosis depends heavily on Breslow thickness (how deep the tumor has grown) and whether lymph nodes are involved. Scalp melanomas tend to be diagnosed at a later stage, which contributes to their higher mortality compared to melanomas elsewhere [3]. The melanoma TNM staging system explains how staging affects treatment decisions and survival estimates.
Key principle: Every stage improvement in detection corresponds to a meaningful improvement in survival. A melanoma caught at Stage I has a five-year survival rate above 95%; Stage IV drops significantly. This is the single strongest argument for regular scalp skin checks.
Scalp skin cancer is not entirely preventable, but the risk can be substantially reduced with consistent protective habits [1].
Most effective preventive measures:
Who is at highest risk and should be most proactive:
For more on pre-cancerous scalp conditions, the actinic keratosis explained article is a useful reference.
See a doctor promptly if any of the following are present on the scalp [2][5]:
Do not wait for symptoms to become severe. Scalp skin cancer is most treatable when caught early, and a suspicious lesion can be evaluated quickly with a biopsy. For those in the Toronto area, the Skin Cancer Clinic in Toronto offers rapid access without a referral, which removes a common barrier to timely assessment.
Q: Can skin cancer on the scalp spread to the brain?
A: Direct invasion of the skull or brain is rare and typically only occurs with very advanced, neglected cancers. More commonly, scalp melanoma spreads via lymph nodes or bloodstream to distant organs. Early treatment prevents this.
Q: Is scalp skin cancer painful?
A: Many scalp skin cancers are painless in early stages. Some lesions may itch, bleed, or become tender as they grow. Pain alone is not a reliable indicator, but any persistent discomfort in a scalp lesion warrants evaluation. See also: does skin cancer hurt.
Q: Can scalp skin cancer grow back after removal?
A: Recurrence is possible, particularly with SCC and melanoma. Mohs surgery has the lowest recurrence rates for BCC and SCC. Regular follow-up appointments after treatment are essential to catch any recurrence early.
Q: How long does it take to diagnose scalp skin cancer?
A: A dermatologist can often identify a suspicious lesion in a single appointment. Biopsy results typically return within one to two weeks. Staging tests, if needed, add additional time.
Q: Does scalp skin cancer always require surgery?
A: Not always. Very superficial BCC lesions may be treated with topical creams, cryotherapy, or photodynamic therapy. However, surgery (especially Mohs) is the standard of care for most scalp skin cancers because it offers the highest cure rates.
Q: Can children get skin cancer on the scalp?
A: Skin cancer in children is rare but not impossible, particularly in children with genetic conditions such as xeroderma pigmentosum or basal cell nevus syndrome. Sun protection habits established in childhood reduce lifetime risk significantly.
Q: How often should I get a professional scalp skin check?
A: For most adults, once a year is the standard recommendation. Those with a history of skin cancer, multiple atypical moles, or significant sun exposure history may benefit from checks every six months.
Q: Is scalp skin cancer more common in men or women?
A: Men are diagnosed with scalp skin cancer more frequently than women. This is partly attributed to higher rates of baldness and thinning hair, more outdoor occupational exposure, and lower rates of hat use and sunscreen application on the scalp.
Q: What does actinic keratosis on the scalp look like?
A: Actinic keratosis (AK) appears as a rough, dry, scaly patch, often pinkish or skin-colored, on sun-exposed scalp skin. AKs are pre-cancerous and can progress to SCC if left untreated. They should be evaluated and treated by a physician.
Q: Can I use regular sunscreen on my scalp?
A: Yes. A mineral sunscreen (zinc oxide or titanium dioxide) in a spray or powder formulation works well on the scalp without leaving a heavy residue on hair. Reapplication every two hours during outdoor exposure is necessary for adequate protection.
Skin cancer on the scalp is a serious and underappreciated threat. The combination of high UV exposure, limited visibility under hair, and infrequent inspection creates conditions where cancers can grow undetected for months or years. Basal cell carcinoma, squamous cell carcinoma, and melanoma each present differently, but all share one critical truth: outcomes are far better when caught early.
Actionable next steps:
For those in Ontario seeking rapid access to evaluation, the Skin Cancer Clinic in Toronto provides no-referral appointments for suspicious lesions. Early action is the most powerful tool available.
[1] Can Your Hair Protect Your Scalp From Skin Cancer - https://health.clevelandclinic.org/can-your-hair-protect-your-scalp-from-skin-cancer
[2] Skin Cancer On Scalp - https://www.schweigerderm.com/skin-care-articles/skin-cancer/skin-cancer-on-scalp/
[3] Skin Cancer On The Scalp Why This Hidden Area Is High Risk - https://www.doctronic.ai/blog/skin-cancer-on-the-scalp-why-this-hidden-area-is-high-risk/
[4] What Does Skin Cancer Look Like On The Scalp - https://biologyinsights.com/what-does-skin-cancer-look-like-on-the-scalp-2/
[5] Skin Cancer On Scalp - https://www.medicalnewstoday.com/articles/skin-cancer-on-scalp
[6] Squamous Cell Skin Cancer - https://www.hopkinsmedicine.org/health/conditions-and-diseases/squamous-cell-skin-cancer



