Lipoma vs Abscess: Understanding the Critical Differences Between These Common Skin Lumps
Discovering an unexpected lump beneath your skin can trigger immediate concern and countless questions. Is it dangerous? Will it go away on its own? Should you see a doctor right away? When it comes to lipoma vs abscess, understanding the fundamental differences between these two common conditions can help you make informed decisions about your health and determine the appropriate course of action. While both conditions present as lumps under the skin, they have distinctly different causes, characteristics, symptoms, and treatment approaches that are essential to recognize.
Key Takeaways
Lipomas are benign fatty tumors that develop slowly over months or years and feel soft and doughy, while abscesses are infected pockets of pus that appear suddenly and feel firm, warm, and painful
Texture and mobility are key differentiators: lipomas move freely under the skin when pressed, whereas abscesses remain fixed and may feel fluctuant due to fluid accumulation
Treatment approaches differ significantly: lipomas typically require surgical excision for permanent removal, while abscesses need incision and drainage to eliminate infection
Pain levels vary considerably: lipomas are usually painless unless pressing on nerves, but abscesses cause significant pain, tenderness, and often systemic symptoms like fever
Professional evaluation is essential for accurate diagnosis, especially since other conditions can mimic both lipomas and abscesses
What Is a Lipoma? 🔬
A lipoma represents one of the most common types of benign soft tissue tumors found in adults. These growths consist entirely of mature fat cells (adipocytes) that cluster together to form a distinct mass between the skin's surface and the underlying muscle layer [1]. Understanding what lipomas are and how they develop provides important context when comparing lipoma vs abscess characteristics.
Composition and Structure
Lipomas are composed of lobules of mature white adipose tissue surrounded by a thin fibrous capsule. This encapsulation distinguishes them from normal subcutaneous fat and allows them to maintain their distinct, movable nature beneath the skin. The fatty tissue within a lipoma is histologically identical to normal fat cells, which explains why these growths are classified as benign rather than malignant [2].
Common Characteristics
Lipomas typically present with several distinctive features that help differentiate them from other skin conditions:
Soft, doughy texture that feels rubbery when touched
Mobile nature - they move freely when pressed with fingers
Slow growth pattern developing over months to years
Painless in most cases, unless they compress nearby nerves
Dome-shaped or oval appearance beneath the skin
Flesh-colored with no visible changes to overlying skin
Small to moderate size, typically less than 2 inches (5 cm) in diameter
Typical Locations
While lipomas can theoretically develop anywhere fatty tissue exists, certain body areas show higher prevalence. The most common sites include [3]:
Body LocationFrequencySpecial ConsiderationsNeck and shouldersVery commonMay be visible, cosmetic concernBackVery commonOften multiple lipomas presentAbdomenCommonCan grow larger before detectionArms and thighsCommonMay interfere with movement if largeForeheadLess commonHigher cosmetic impactChestModerateMay be confused with other masses
Lipomas most frequently appear in adults between the ages of 40 and 60, though they can develop at any age [4]. They occur slightly more often in women than men, and genetic predisposition plays a significant role in their development. Approximately 2-3% of the general population develops lipomas, with some individuals developing multiple lipomas throughout their lifetime—a condition sometimes called familial multiple lipomatosis.
What Is an Abscess? 💉
An abscess represents the body's defensive response to bacterial infection, manifesting as a localized collection of pus within a newly formed cavity in tissue. Unlike the benign fatty composition of lipomas, abscesses result from active infection and inflammation, making the comparison of lipoma vs abscess particularly important for appropriate treatment decisions.
Formation and Development
Abscesses form when bacteria invade tissue through breaks in the skin barrier, hair follicles, or blocked glands. The immune system responds by sending white blood cells to fight the infection, and as these cells accumulate along with bacteria, dead tissue, and cellular debris, they create the characteristic pus-filled pocket [5]. The body attempts to wall off this infection by forming a membrane around it, preventing the infection from spreading to surrounding tissues.
Distinctive Features
Abscesses present with markedly different characteristics compared to lipomas:
Firm, fluctuant texture due to fluid (pus) accumulation
Fixed position - minimal movement when pressed
Rapid onset appearing within days following infection
Painful and tender with significant discomfort
Red, warm skin overlying the abscess
Swelling that may increase rapidly
Possible drainage of pus if the abscess ruptures
Systemic symptoms including fever and malaise
Types of Abscesses
Abscesses can develop in various forms and locations throughout the body:
Skin Abscesses (Cutaneous)
Furuncles (boils) - infections of hair follicles
Carbuncles - clusters of infected follicles
Pilonidal abscesses - near the tailbone
Hidradenitis suppurativa - recurring abscesses in sweat glands
The most common bacterial culprits responsible for abscess formation include:
Staphylococcus aureus (including MRSA strains) - most frequent cause
Streptococcus species - particularly Group A Streptococcus
Escherichia coli - especially in abdominal abscesses
Pseudomonas aeruginosa - in certain wound infections
Anaerobic bacteria - in deeper tissue abscesses
Understanding the difference between boils and cysts can also help distinguish abscess-related conditions from other skin growths.
Risk Factors for Abscess Development
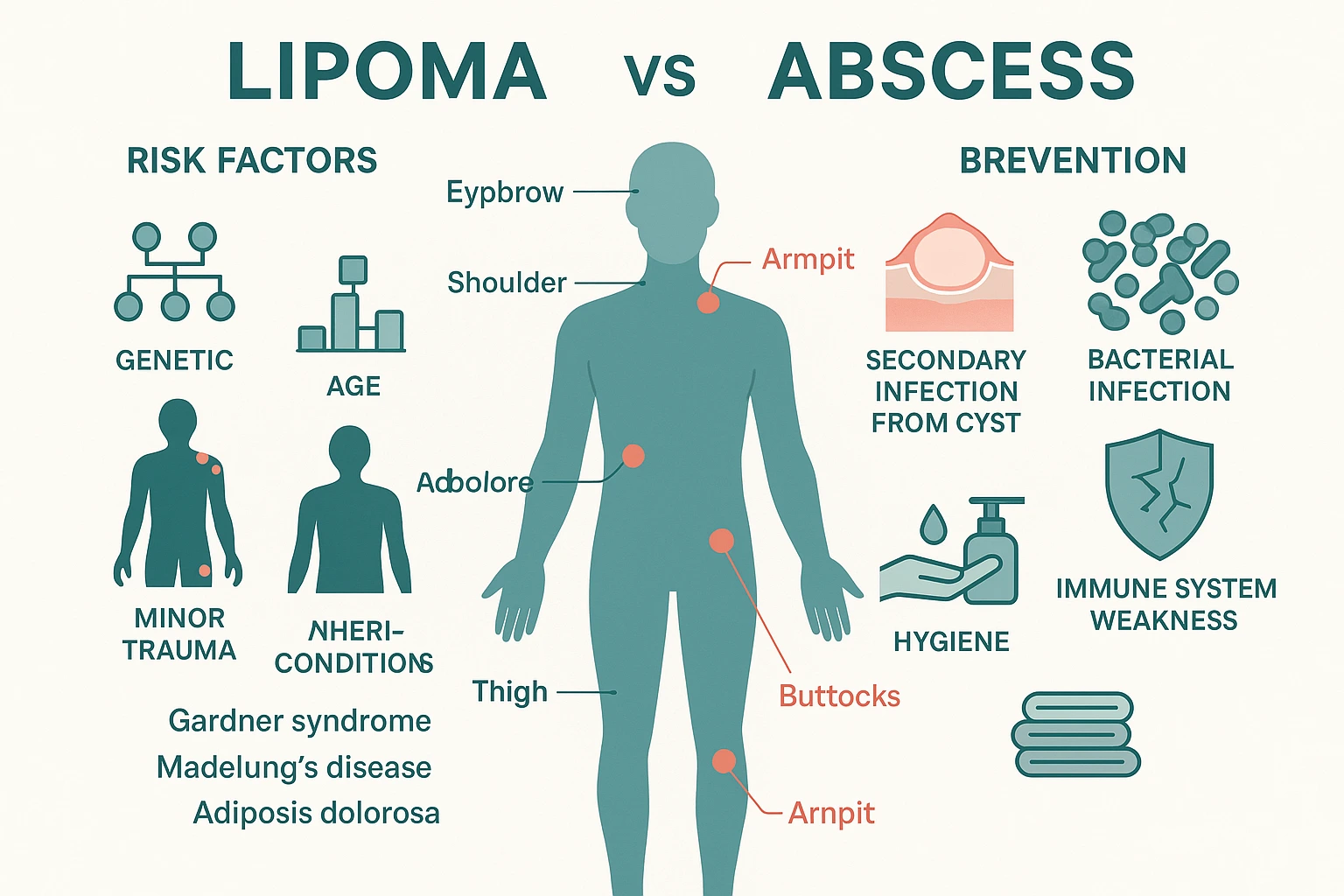
Several factors increase the likelihood of developing an abscess [6]:
Compromised immune system (diabetes, HIV, chemotherapy)
Poor hygiene or skin care practices
Close contact with infected individuals
Existing skin conditions (eczema, acne)
Intravenous drug use
Obesity
Advanced age
Previous abscess history
Lipoma vs Abscess: Key Differences in Appearance and Texture 👁️
When examining the critical distinctions in the lipoma vs abscess comparison, appearance and texture provide some of the most reliable diagnostic clues. These physical characteristics can often help differentiate between these conditions even before professional medical evaluation.
Texture Comparison
The tactile differences between lipomas and abscesses are among the most distinctive features:
Lipoma Texture:
Soft and doughy - feels similar to soft rubber or dough
Smooth surface with well-defined borders
Compressible - yields to gentle pressure
Rubbery consistency that springs back when released
Uniform throughout with consistent texture
Abscess Texture:
Firm initially becoming fluctuant as pus accumulates
Tense surface due to internal pressure from fluid
Fluctuant quality - feels like a water balloon when fully formed
Indurated (hardened) surrounding tissue from inflammation
Variable consistency depending on stage of development
Mobility and Movement
How a lump moves beneath the skin provides crucial diagnostic information:
Lipoma Mobility: Lipomas demonstrate remarkable mobility because they exist within a capsule separate from surrounding tissue. When you press on a lipoma with your fingers, it typically:
Moves freely in multiple directions
Slides easily beneath the skin
Can be manipulated away from the pressure point
Maintains its shape while moving
Returns to original position when released
Abscess Mobility: Abscesses show minimal to no mobility because inflammation causes them to adhere to surrounding tissues. When examining an abscess:
Remains fixed in position
Cannot be moved away from the site
Surrounding tissue moves with the abscess
Pressure causes pain rather than movement
Feels anchored to deeper structures
Visual Appearance
The overlying skin appearance differs markedly between these conditions:
FeatureLipomaAbscessSkin colorNormal, flesh-coloredRed, inflamed, possibly purpleSkin temperatureNormal to touchWarm or hot to touchSkin textureSmooth, unchangedTight, shiny, stretchedVisible changesSubtle bulge onlyObvious swelling, possible pustuleSkin integrityIntactMay show pointing or drainageSurrounding areaNormal appearanceRedness extending beyond lump
Size and Shape Characteristics
Lipoma Dimensions:
Typically 1-3 cm (0.4-1.2 inches) in diameter
Can grow up to 10 cm (4 inches) or larger in rare cases
Oval or dome-shaped with smooth contours
Well-circumscribed with clear boundaries
Symmetrical appearance
Slow, gradual size increase over months to years
Abscess Dimensions:
Variable size from small (1 cm) to large (10+ cm)
Rapid size increase over days
Round or irregular shape
Less defined boundaries due to surrounding inflammation
May appear asymmetrical
Size fluctuates with pus accumulation and drainage
Surface Temperature
Temperature differences provide important diagnostic clues in the lipoma vs abscess evaluation:
Lipoma Temperature: Lipomas maintain normal body temperature because they lack the inflammatory response. The overlying skin feels no different from surrounding areas, and there is no heat generation from the growth itself.
Abscess Temperature: Abscesses generate significant heat due to active infection and inflammation. The increased blood flow to the area, combined with the metabolic activity of white blood cells fighting infection, creates a noticeably warm or hot sensation when touched. This warmth often extends beyond the abscess itself into surrounding tissue [7].
For comprehensive evaluation of unusual skin lumps and professional diagnosis, specialized centers offering skin lesion assessment can provide expert guidance.
Lipoma vs Abscess: Symptoms and Pain Levels 🩺
The symptom profile represents another crucial differentiator when comparing lipoma vs abscess. While both conditions present as palpable lumps, their associated symptoms vary dramatically, reflecting their fundamentally different natures—benign fatty growth versus active infection.
Pain and Discomfort
Lipoma Pain Profile: Most lipomas are completely painless and may go unnoticed for extended periods. However, certain circumstances can cause discomfort:
Nerve compression: When a lipoma grows near or around a nerve, it can cause pain, tingling, or numbness
Size-related discomfort: Large lipomas may create pressure sensations or mechanical discomfort
Location-dependent pain: Lipomas in areas subject to friction or pressure (such as under bra straps or waistbands) may become tender
Angiolipomas: A specific subtype containing blood vessels that can be tender or painful
Rapid growth: Unusually fast-growing lipomas may cause stretching sensations
Abscess Pain Profile: Abscesses are characteristically painful from early development through resolution:
Throbbing pain: Constant, pulsating discomfort that worsens with touch
Tenderness: Extreme sensitivity even to light pressure
Progressive pain: Increasing intensity as the abscess enlarges
Positional pain: Worsening with certain movements or positions
Pressure sensation: Feeling of tightness or fullness
Pain relief after drainage: Significant improvement once pus is released
Associated Symptoms
Beyond pain, the symptom constellation differs markedly:
Lipoma Associated Symptoms:
Generally no systemic symptoms
No fever or chills
No skin changes (redness, warmth)
No discharge or drainage
Occasional cosmetic concern
Rarely affects daily activities
May cause anxiety about appearance
Abscess Associated Symptoms:
Fever (temperature above 100.4°F/38°C) [8]
Chills and sweating
Fatigue and malaise
Loss of appetite
Swollen lymph nodes near the affected area
Pus drainage (yellow, white, or bloody discharge)
Foul odor from infected material
Red streaking from the site (indicating spreading infection)
General feeling of illness
Symptom Timeline
The temporal pattern of symptom development provides diagnostic clarity:
Lipoma Timeline:
Appears gradually over months to years
Slow, steady growth without sudden changes
Symptoms (if any) develop proportionally to size
Stable condition without fluctuation
No acute worsening episodes
Can remain unchanged for years
Abscess Timeline:
Develops rapidly over days (24-72 hours typical)
Acute onset of pain and swelling
Progressive worsening until treated
May spontaneously rupture and drain
Symptoms fluctuate with pus accumulation
Requires prompt intervention
Functional Impact
The effect on daily activities differs substantially:
Lipoma Functional Impact:
Minimal interference with normal activities
Possible cosmetic concerns affecting self-esteem
Large lipomas may limit range of motion
Generally no urgent treatment needed
Quality of life impact primarily psychological
Abscess Functional Impact:
Significant pain limiting movement
Difficulty performing normal tasks
Sleep disturbance due to discomfort
Inability to wear certain clothing
Urgent treatment required
Work or school absence often necessary
Warning Signs Requiring Immediate Attention
Certain symptoms indicate serious complications requiring emergency evaluation:
For Suspected Lipomas:
Rapid growth over days or weeks
Sudden onset of pain
Changes in texture or firmness
Size larger than 2 inches (5 cm)
Fixed to underlying structures
Overlying skin changes
For Suspected Abscesses:
Fever above 101°F (38.3°C)
Red streaking extending from the abscess
Increasing area of redness and warmth
Severe pain unresponsive to over-the-counter medication
Multiple abscesses developing
Confusion or altered mental status
Rapid heart rate or breathing difficulty
Understanding these symptom differences in the lipoma vs abscess comparison enables appropriate timing for medical consultation and helps prevent complications from delayed treatment.
Causes and Risk Factors: Lipoma vs Abscess 🧬
Understanding the underlying causes and risk factors for each condition provides essential context in the lipoma vs abscess discussion. While both manifest as subcutaneous lumps, their etiologies are fundamentally different—genetic and metabolic factors for lipomas versus infectious processes for abscesses.
What Causes Lipomas?
The exact cause of lipoma formation remains incompletely understood, but research has identified several contributing factors [9]:
Genetic Factors:
Familial predisposition: Strong hereditary component with 2-3 times higher risk if family members have lipomas
Dercum's disease (adiposis dolorosa): Painful lipomas throughout the body
Gardner syndrome: Part of familial adenomatous polyposis with multiple lipomas
Madelung's disease: Symmetric lipomatosis affecting neck and shoulders
Cowden syndrome: Multiple hamartomas including lipomas
Chromosomal Abnormalities: Research has identified chromosomal rearrangements in lipoma tissue, particularly involving chromosomes 12 and 13, suggesting genetic mutations may trigger abnormal fat cell growth [10].
Metabolic Factors:
Obesity (though lipomas also occur in thin individuals)
Glucose intolerance and insulin resistance
Liver disease
Alcohol consumption (particularly in Madelung's disease)
Trauma and Injury: Some evidence suggests minor injuries or blunt trauma may trigger lipoma formation, though this remains controversial. The "post-traumatic lipoma" theory proposes that tissue injury stimulates adipocyte proliferation in susceptible individuals.
Age-Related Factors: Peak incidence between ages 40-60 suggests age-related metabolic or hormonal changes may contribute to lipoma development.
What Causes Abscesses?
Abscesses result from bacterial infection, with several pathways leading to their formation:
Primary Bacterial Invasion:
Breaks in skin integrity (cuts, scrapes, puncture wounds)
Hair follicle infections (folliculitis progressing to abscess)
Prompt treatment: Addressing skin infections early
For individuals experiencing unusual skin growths or recurrent lumps, professional evaluation at specialized skin assessment centers can identify underlying risk factors and provide appropriate management strategies.
Diagnosis: How Doctors Differentiate Lipoma vs Abscess 🔍
Accurate diagnosis is essential in the lipoma vs abscess comparison, as treatment approaches differ dramatically. Healthcare providers use a systematic evaluation combining clinical examination, imaging studies, and occasionally laboratory tests to distinguish between these conditions and rule out other possibilities.
Clinical Examination
The diagnostic process begins with thorough physical assessment:
Healthcare providers must also consider other conditions that may mimic lipomas or abscesses:
Conditions Mimicking Lipomas:
Liposarcoma: Malignant fatty tumor (rare, requires biopsy to distinguish)
Epidermoid cysts: May feel similar but have central punctum
Lymph nodes: Mobile but firmer, often multiple
Hernias: May reduce with pressure, change with position
Neurofibromas: Associated with nerve tissue, may cause tingling
Conditions Mimicking Abscesses:
Infected cysts: May have abscess features but with cyst history
Cellulitis: Infection without pus collection
Hematoma: Blood collection from trauma
Inflamed lipoma: Rare but can become tender
Thrombosed blood vessels: Firm, tender, linear
Malignancies: Some cancers present as inflamed masses
When to Seek Immediate Medical Evaluation
Certain presentations require urgent assessment:
Red Flag Symptoms:
Rapid growth over days
Severe pain or fever
Red streaking from the lump
Multiple abscesses developing
Abscess on face (risk of spreading to brain)
Inability to move affected body part
Signs of systemic infection (confusion, rapid heartbeat)
Recurrent abscesses in same location
Abscess in immunocompromised individual
For comprehensive diagnostic evaluation and expert assessment of skin lumps, specialized minor surgery centers offer advanced diagnostic capabilities and treatment options.
Biopsy and Pathological Examination
In uncertain cases, tissue sampling provides definitive diagnosis:
Fine Needle Aspiration (FNA):
Thin needle extracts cells for microscopic examination
Useful for distinguishing lipoma from other soft tissue masses
Lipoma findings: Mature adipocytes without atypia
Minimally invasive outpatient procedure
Core Needle Biopsy:
Larger tissue sample than FNA
Better architectural assessment
Performed under local anesthesia
Useful when liposarcoma suspected
Excisional Biopsy:
Complete removal of small masses for diagnosis
Provides both treatment and diagnosis
Standard approach for suspicious lipomas
Entire specimen sent for pathological examination
Pathology Report Elements:
Microscopic description of tissue
Cell type identification
Presence or absence of malignancy
Margins assessment (if excised)
Special stains if needed
Final diagnosis and recommendations
The combination of clinical assessment, imaging, and when necessary, tissue sampling, allows healthcare providers to accurately differentiate lipoma vs abscess and develop appropriate treatment plans tailored to each condition's specific requirements.
Treatment Options: Lipoma vs Abscess 💊
The treatment approaches for lipoma vs abscess differ fundamentally, reflecting their distinct natures—benign fatty growth versus active infection. Understanding these treatment differences is crucial for appropriate management and optimal outcomes.
Lipoma Treatment Options
Since lipomas are benign and typically harmless, treatment focuses on removal for symptomatic or cosmetic concerns:
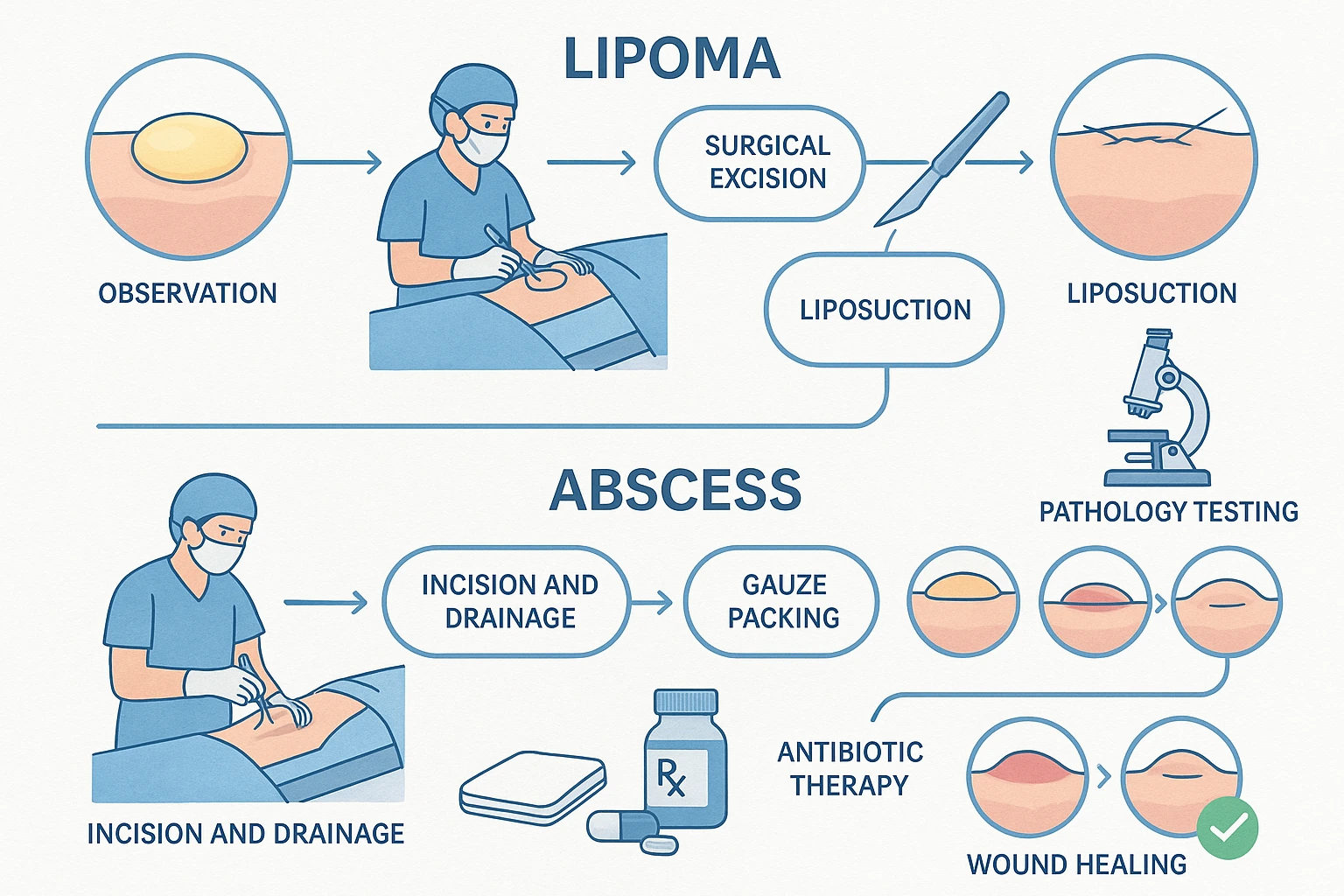
Observation (Watchful Waiting): Many lipomas require no treatment if they:
Remain small and stable
Cause no symptoms or discomfort
Don't interfere with function
Don't create cosmetic concerns
Show no signs of rapid growth
Patients should monitor for changes in size, texture, or symptoms and report any concerning developments to their healthcare provider.
Surgical Excision (Most Common and Definitive): Complete surgical removal represents the gold standard for lipoma treatment [12]:
Procedure Details:
Performed under local anesthesia (larger lipomas may require sedation)
Diabetes control: Maintaining blood sugar in target range
Treatment Comparison Summary
AspectLipoma TreatmentAbscess TreatmentUrgencyElective, can waitUrgent, requires prompt treatmentPrimary approachSurgical excisionIncision and drainageAnesthesiaLocal (sometimes sedation)LocalAntibioticsNot neededSometimes requiredRecovery time1-2 weeks2-4 weeksRecurrence rateLow (1-2% with complete excision)Moderate (10-20% without addressing risk factors)Follow-upSuture removal, pathology resultsPacking changes, wound checksHome careMinimalExtensive (dressing changes, warm compresses)
Complications and When to Seek Additional Care
Lipoma Removal Complications (Rare):
Bleeding or hematoma formation
Infection at surgical site
Nerve damage causing numbness
Scarring or poor cosmetic outcome
Incomplete removal with recurrence
Abscess Treatment Complications:
Incomplete drainage: Persistent infection
Spreading infection: Cellulitis, lymphangitis
Sepsis: Life-threatening systemic infection
Fistula formation: Abnormal tract development
Scarring: Particularly with large or recurrent abscesses
Warning Signs Requiring Immediate Attention:
Fever above 101°F (38.3°C)
Red streaking from treatment site
Increasing pain despite treatment
Pus or drainage from surgical site
Signs of allergic reaction to antibiotics
Confusion or altered mental status
For expert treatment of both lipomas and abscesses, specialized facilities offering cyst and lipoma removal services provide comprehensive care with experienced practitioners.
Understanding the distinct treatment approaches in the lipoma vs abscess comparison enables patients to have realistic expectations about procedures, recovery, and outcomes, facilitating informed decision-making and optimal results.
When to See a Doctor: Lipoma vs Abscess 👨⚕️
Knowing when to seek medical evaluation is crucial in managing both lipomas and abscesses effectively. While the urgency differs significantly between these conditions, professional assessment ensures accurate diagnosis and appropriate treatment in the lipoma vs abscess scenario.
Lipoma: When Medical Evaluation Is Recommended
While lipomas are benign and often require no immediate intervention, certain situations warrant professional assessment:
Recommended Evaluation Scenarios:
First-time discovery: Any new lump should be evaluated to confirm it's a lipoma and not something more serious
Size changes: Rapid growth or significant size increase
Developing symptoms: New pain, tenderness, or discomfort
Large size: Lipomas exceeding 2 inches (5 cm) in diameter
Functional interference: Limiting movement or daily activities
Multiple lipomas: Numerous growths suggesting possible genetic syndrome
Texture changes: Becoming firmer or developing irregular borders
Fixed position: Loss of mobility suggesting deeper attachment
Non-Urgent Timeline: Lipoma evaluation can typically be scheduled as a routine appointment within days to weeks. There's generally no need for emergency or urgent care visits for uncomplicated lipomas.
What to Expect at the Appointment:
Physical examination of the lump
Medical and family history discussion
Possible ultrasound or imaging
Discussion of treatment options
Observation versus removal decision
Scheduling of excision if desired
Abscess: When Medical Evaluation Is Essential
Abscesses require more urgent attention due to their infectious nature:
Immediate Medical Attention Needed:
Any abscess larger than 1 cm (about ½ inch)
Facial abscesses: Risk of spreading to brain or eyes
Severe pain: Interfering with sleep or function
Fever: Temperature above 100.4°F (38°C)
Red streaking: Lines extending from the abscess
Rapid expansion: Noticeable growth within hours
Multiple abscesses: Several developing simultaneously
Immunocompromised status: Diabetes, HIV, cancer, or immunosuppressive medications
Failed home treatment: No improvement after 48 hours of warm compresses
Recurrent abscesses: Multiple episodes in same or different locations
Emergency Department Indications: Seek immediate emergency care for:
High fever (above 101°F/38.3°C)
Confusion or altered mental status
Rapid heartbeat or breathing difficulty
Abscess on face, especially near eyes or nose
Severe pain uncontrolled by medication
Signs of sepsis: Extreme illness, low blood pressure, rapid pulse
Spreading redness covering large area
Inability to move affected body part
Urgent Care Timeline: Most abscesses should be evaluated within 24 hours of recognition. Don't wait to see if they improve on their own, as delayed treatment can lead to complications.
Choosing the Right Healthcare Provider
Different healthcare settings offer appropriate care for various situations:
Primary Care Physician:
Initial evaluation of lipomas
Small, uncomplicated abscesses
Follow-up care after treatment
Management of recurrent infections
Coordination of specialist referrals
Dermatologist:
Expert evaluation of skin lumps
Diagnosis of unusual presentations
Treatment of complex or recurrent abscesses
Management of underlying skin conditions
Cosmetic concerns with lipomas
Surgeon or Minor Surgery Specialist:
Lipoma excision procedures
Large or complex abscess drainage
Recurrent abscess management
Lipomas in difficult locations
Multiple lipoma removal
Specialized centers like The Minor Surgery Center offer comprehensive evaluation and treatment for both conditions with experienced practitioners.
Urgent Care Centers:
After-hours abscess evaluation
Incision and drainage procedures
Antibiotic prescriptions
Initial assessment before specialist referral
Emergency Department:
Life-threatening infections
Severe systemic symptoms
Facial abscesses
Complicated or spreading infections
When other options unavailable
Preparing for Your Appointment
Maximize the value of your medical visit with proper preparation:
Information to Gather:
Timeline: When did you first notice the lump?
Changes: Has it grown, changed color, or become painful?
Symptoms: Any fever, drainage, or systemic symptoms?
Previous lumps: History of lipomas, cysts, or abscesses?
Family history: Do relatives have similar conditions?
Medical conditions: Diabetes, immune disorders, skin conditions?
Medications: Current prescriptions and supplements
Allergies: Particularly to antibiotics or anesthetics
Questions to Ask:
Is this a lipoma or an abscess?
What caused this to develop?
Do I need treatment now, or can we watch it?
What are my treatment options?
What are the risks and benefits of each option?
How long is the recovery period?
Will there be a scar?
What's the chance of recurrence?
Are there preventive measures I should take?
When should I schedule follow-up?
Photos and Documentation:
Take photos showing size and appearance
Note any changes over time
Document symptoms in a journal
Bring list of questions and concerns
Red Flags: Never Ignore These Signs
Certain symptoms indicate serious complications requiring immediate attention:
Critical Warning Signs:
Rapid spread: Infection expanding visibly over hours
Systemic toxicity: Feeling severely ill, confused, or weak
Breathing difficulty: May indicate spreading infection
Facial swelling: Especially around eyes or nose
Inability to drain: Abscess not responding to I&D
Necrotizing infection: Skin turning dark or developing blisters
Septic appearance: Very ill, low blood pressure, rapid pulse
Diabetic patient with abscess: Higher risk of complications
Cost Considerations and Insurance
Understanding financial aspects helps with planning:
Lipoma Removal:
May be considered cosmetic if asymptomatic
Insurance often covers symptomatic or large lipomas
Documentation of symptoms improves coverage likelihood
Costs range from $500-$3,000 depending on size and location
Pathology fees additional
Abscess Treatment:
Generally covered as medically necessary
I&D typically $200-$800 in office setting
Emergency department treatment significantly more expensive
Antibiotics usually covered with copay
Follow-up visits may require additional copays
Prior Authorization: Some insurance plans require pre-approval for:
Lipoma excision (especially if cosmetic)
Specialist referrals
Advanced imaging
Surgical procedures
Check with your insurance provider before scheduling elective procedures.
Telemedicine Options
Virtual consultations may be appropriate for:
Initial assessment of small, non-painful lumps
Follow-up after in-person treatment
Discussion of treatment options
Monitoring stable lipomas
Post-procedure questions
Limitations:
Cannot perform physical examination
No hands-on procedures possible
May require in-person follow-up
Not appropriate for urgent abscesses
For comprehensive information on various skin conditions and when to seek care, the blog resources provide valuable educational content.
Understanding when to seek medical care in the lipoma vs abscess comparison ensures timely, appropriate intervention, preventing complications and achieving optimal outcomes. When in doubt, err on the side of caution and consult a healthcare professional.
Living with Lipomas and Preventing Abscesses 🛡️
Managing existing lipomas and preventing abscess formation requires understanding long-term strategies and lifestyle modifications. While the lipoma vs abscess comparison highlights their different natures, both conditions benefit from informed self-care and preventive measures.
Living with Lipomas
For individuals diagnosed with lipomas who choose observation over removal, several management strategies can help:
Monitoring for Changes: Regular self-examination helps detect concerning developments:
Monthly checks: Assess size, texture, and mobility
Measure dimensions: Use ruler or measuring tape for objective tracking
Photo documentation: Take periodic photos for comparison
Symptom journal: Note any pain, tenderness, or functional changes
Annual professional examination: Healthcare provider assessment
When to Reconsider Treatment: Initially asymptomatic lipomas may eventually require removal if they:
Grow beyond 2 inches (5 cm)
Develop pain or tenderness
Limit movement or function
Cause cosmetic distress
Show rapid growth
Change in texture or firmness
Psychological Impact: Visible lipomas can affect self-esteem and quality of life:
Clothing choices: May avoid styles that reveal lipomas
Social anxiety: Self-consciousness in public situations
Body image: Impact on self-perception
Support resources: Counseling or support groups may help
Cosmetic camouflage: Makeup or clothing strategies
Managing Multiple Lipomas: Individuals with familial multiple lipomatosis face unique challenges:
Prioritize removal: Focus on symptomatic or visible lipomas
Staged procedures: Remove several lipomas over multiple sessions
Monitoring: Regular follow-up to assess effectiveness
Risks: Antibiotic resistance, side effects
Alternative: Reserved for severe cases
Special Populations
Certain groups require tailored prevention strategies:
Athletes:
Shower immediately after practice or competition
Avoid sharing towels, razors, or equipment
Cover wounds before participating
Clean equipment regularly
Report infections to coaches promptly
Healthcare Workers:
Hand hygiene: Frequent washing and sanitizing
Personal protective equipment: Use appropriately
Wound coverage: Keep cuts covered
Occupational health: Report exposures
Immunocompromised Individuals:
Enhanced hygiene: Meticulous skin care
Prompt treatment: Address minor wounds immediately
Prophylactic measures: Discuss with healthcare provider
Regular monitoring: Frequent medical follow-up
For individuals in the Greater Toronto Area seeking specialized care for skin conditions, centers offering services in Barrie provide accessible options.
Long-Term Outlook
Lipoma Prognosis:
Benign condition with excellent prognosis
No malignant transformation (extremely rare)
Successful removal has low recurrence
Quality of life impact primarily cosmetic
No life-threatening complications
Abscess Prognosis:
Excellent with prompt treatment
Recurrence preventable with proper hygiene
Rare serious complications with early intervention
Underlying conditions require ongoing management
Prevention strategies highly effective
Understanding these long-term management and prevention strategies in the lipoma vs abscess comparison empowers individuals to take control of their health, minimize recurrence risk, and maintain optimal skin health throughout their lives.
Conclusion: Making Informed Decisions About Lipoma vs Abscess
Understanding the fundamental differences between lipoma vs abscess is essential for anyone who discovers an unexpected lump beneath their skin. While both conditions manifest as palpable masses, their distinct characteristics—from causes and symptoms to treatment approaches—require different management strategies and levels of urgency.
Lipomas represent benign fatty tumors that develop gradually over months or years, typically causing no symptoms beyond cosmetic concerns. These soft, mobile, painless growths pose no serious health threat and can often be safely monitored without treatment. When removal becomes necessary due to size, symptoms, or aesthetic preferences, surgical excision provides a definitive solution with excellent outcomes and low recurrence rates.
Abscesses, in contrast, demand prompt medical attention as active bacterial infections that can lead to serious complications if left untreated. These painful, warm, fluctuant collections of pus require incision and drainage, often supplemented with antibiotics, to eliminate infection and promote healing. Unlike lipomas, abscesses cannot be safely ignored or managed with observation alone.
The key differentiators in the lipoma vs abscess comparison include:
Timeline: Gradual development (lipoma) versus sudden onset (abscess)
Texture: Soft and doughy (lipoma) versus firm and fluctuant (abscess)
Mobility: Freely movable (lipoma) versus fixed (abscess)
Pain: Usually painless (lipoma) versus painful and tender (abscess)
Skin changes: Normal appearance (lipoma) versus red, warm, inflamed (abscess)
Urgency: Elective treatment (lipoma) versus urgent intervention (abscess)
Actionable Next Steps
If you've discovered a lump under your skin, take these important steps:
Assess the characteristics: Note the size, texture, mobility, pain level, and any skin changes
Consider the timeline: Determine whether it appeared gradually or suddenly
Monitor for warning signs: Watch for fever, spreading redness, or increasing pain
Seek appropriate care:
Lipomas: Schedule routine appointment with primary care or dermatologist
Abscesses: Seek urgent evaluation within 24 hours
Emergency symptoms: Go to emergency department immediately
Document changes: Take photos and keep a symptom journal
Practice prevention: Implement hygiene measures to prevent future abscesses
Follow through with treatment: Complete prescribed antibiotics and attend follow-up appointments
When Professional Evaluation Is Essential
Don't hesitate to seek medical care if you experience:
Any new lump that you're uncertain about
Rapid growth or changes in an existing lump
Pain, fever, or systemic symptoms
Multiple lumps developing
Recurrent abscesses
Concerns about appearance or function
Professional evaluation provides accurate diagnosis, appropriate treatment, and peace of mind. Specialized centers with expertise in skin conditions and minor surgical procedures offer comprehensive care for both lipomas and abscesses, ensuring optimal outcomes and patient satisfaction.
Empowering Your Health Decisions
Knowledge about the lipoma vs abscess distinction empowers you to:
Make informed treatment decisions based on accurate information
Communicate effectively with healthcare providers
Implement prevention strategies to reduce abscess risk
Manage expectations about treatment and recovery
Advocate for appropriate care when needed
Remember that while this information provides valuable guidance, it cannot replace professional medical evaluation. Each individual's situation is unique, and personalized assessment by a qualified healthcare provider ensures the most appropriate diagnosis and treatment plan.
By understanding these fundamental differences and taking proactive steps toward evaluation and treatment when needed, you can confidently manage skin lumps and maintain optimal health. Whether dealing with a benign lipoma or an infected abscess, appropriate care leads to excellent outcomes and resolution of concerns.
[3] Salam GA. Lipoma excision. American Family Physician. 2002;65(5):901-904.
[4] Rydholm A, Berg NO. Size, site and clinical incidence of lipoma. Factors in the differential diagnosis of lipoma and sarcoma. Acta Orthopaedica Scandinavica. 1983;54(6):929-934.
[5] Singer AJ, Talan DA. Management of skin abscesses in the era of methicillin-resistant Staphylococcus aureus. New England Journal of Medicine. 2014;370(11):1039-1047.
[6] Talan DA, Mower WR, Krishnadasan A, et al. Trimethoprim-sulfamethoxazole versus placebo for uncomplicated skin abscess. New England Journal of Medicine. 2016;374(9):823-832.
[7] Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2014;59(2):147-159.
[8] Duong M, Markwell S, Peter J, Barenkamp S. Randomized, controlled trial of antibiotics in the management of community-acquired skin abscesses in the pediatric patient. Annals of Emergency Medicine. 2010;55(5):401-407.
[9] Mentzel T, Fletcher CD. Lipomatous tumours of soft tissues: an update. Virchows Archiv. 1995;427(4):353-363.
[10] Sandberg AA. Updates on the cytogenetics and molecular genetics of bone and soft tissue tumors: lipoma. Cancer Genetics and Cytogenetics. 2004;150(2):93-115.
[11] Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. New England Journal of Medicine. 2006;355(7):666-674.
[12] Silistreli OK, Durmuş EU, Ulusal BG, Oztan Y, Görgü M. What should be the treatment modality in giant cutaneous lipomas? Review of the literature and report of 4 cases. British Journal of Plastic Surgery. 2005;58(3):394-398.
[13] Llera JL, Levy RC. Treatment of cutaneous abscess: a double-blind clinical study. Annals of Emergency Medicine. 1985;14(1):15-19.
[14] Fritz SA, Hogan PG, Hayek G, et al. Household versus individual approaches to eradication of community-associated Staphylococcus aureus in children: a randomized trial. Clinical Infectious Diseases. 2012;54(6):743-751.