Last updated: February 25, 2026
When a soft lump appears under the skin, the first question is often "What is it?" and the second is "How do we know for sure?" Lipoma imaging explained starts with understanding that not every lump needs a scan, but when imaging is necessary, choosing the right type matters. Ultrasound, MRI, and CT scans each reveal different details about lipomas—those benign fatty tumors that affect roughly 1-2% of the population—and knowing what each test can and cannot tell you helps avoid unnecessary procedures, costs, and anxiety.
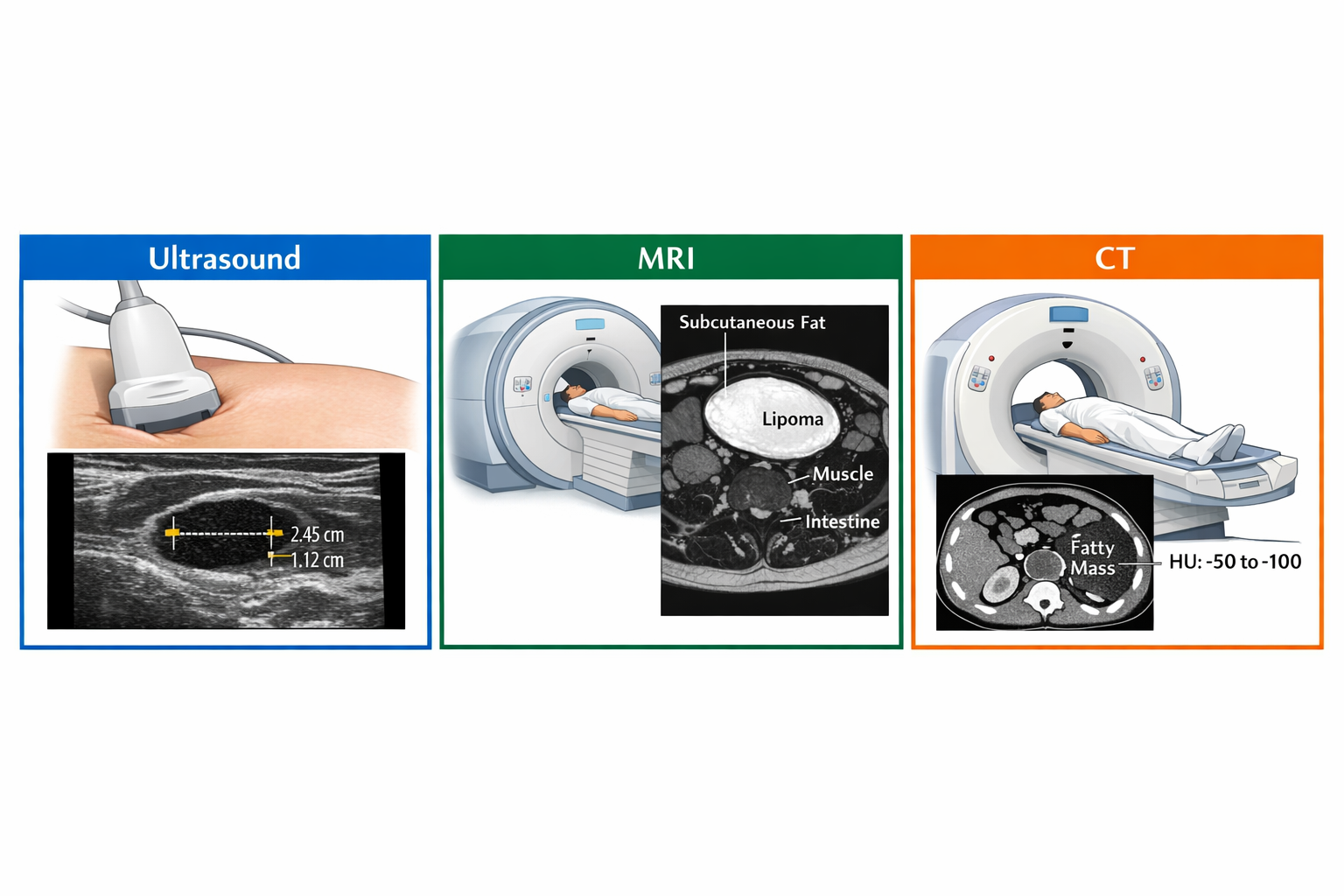
Lipoma imaging explained in simple terms: ultrasound is usually the first and often only imaging test needed for suspected lipomas, confirming the fatty composition and measuring size in about 15-30 minutes. MRI becomes necessary when the lipoma is deep, large (over 5 cm), painful, or shows atypical features that raise concern for liposarcoma. CT scans are rarely used specifically for lipoma diagnosis but may incidentally detect them during imaging for other conditions. Most small, superficial lipomas diagnosed by physical exam alone don't require any imaging at all.
A lipoma is a benign (non-cancerous) tumor made of fat cells that grows slowly in the soft tissue layer between the skin and underlying muscle. Most lipomas can be diagnosed through physical examination alone without any imaging tests. Doctors can typically identify lipomas by their characteristic feel: soft, doughy, mobile lumps that move easily under the skin when pressed.
Imaging becomes necessary when:
Common mistake: Assuming every soft tissue lump needs imaging. This leads to unnecessary costs and radiation exposure (in the case of CT scans). If your doctor can confidently diagnose a typical lipoma by examination, imaging may add little value.
For more information about lipoma characteristics and diagnosis, see our guide on how lipomas are diagnosed.
Ultrasound is the preferred first-line imaging test for suspected lipomas because it's non-invasive, radiation-free, relatively inexpensive, and highly effective at distinguishing fatty tissue from other soft tissue masses. The test uses high-frequency sound waves that bounce off tissues and create real-time images on a monitor.
Typical ultrasound process:
Choose ultrasound if: The lipoma is superficial (within 1-2 inches of skin surface), you need quick results, cost is a concern, or you want to avoid radiation exposure.
Learn more about differentiating lipomas from other soft tissue masses.
MRI (Magnetic Resonance Imaging) provides the most comprehensive and detailed view of lipomas and surrounding tissues, making it the gold standard when there's any concern about malignancy or when surgical planning requires precise anatomical information. MRI uses powerful magnets and radio waves to create detailed cross-sectional images without radiation.
AspectDetailsDuration30-60 minutes depending on area scannedPreparationRemove all metal objects; may require fasting if contrast dye is usedContrastSometimes gadolinium contrast is injected to better visualize blood vessels and suspicious areasPositioningMust remain completely still inside the MRI tubeResultsTypically available within 2-3 business days
Choose MRI if: The lipoma is deep-seated, larger than 5 cm, rapidly growing, painful, located near critical structures, or shows any atypical features on physical exam or ultrasound.
Common mistake: Ordering MRI as the first test for every lipoma. This drives up healthcare costs unnecessarily when ultrasound would suffice for straightforward cases.
For information about lipoma removal after imaging confirms diagnosis, see our guide on lipoma removal surgery recovery.
CT (Computed Tomography) scans are rarely the first choice for lipoma evaluation but can provide valuable information in specific situations. CT uses X-rays to create detailed cross-sectional images and is particularly good at showing the relationship between soft tissues and bone.
CT imaging for lipomas typically occurs in these scenarios:
Choose CT if: You're already getting a CT scan for another reason, the lipoma is in a deep body cavity, or MRI is contraindicated.
Avoid CT if: The lipoma is superficial, you're concerned about radiation exposure, or MRI is available and appropriate.
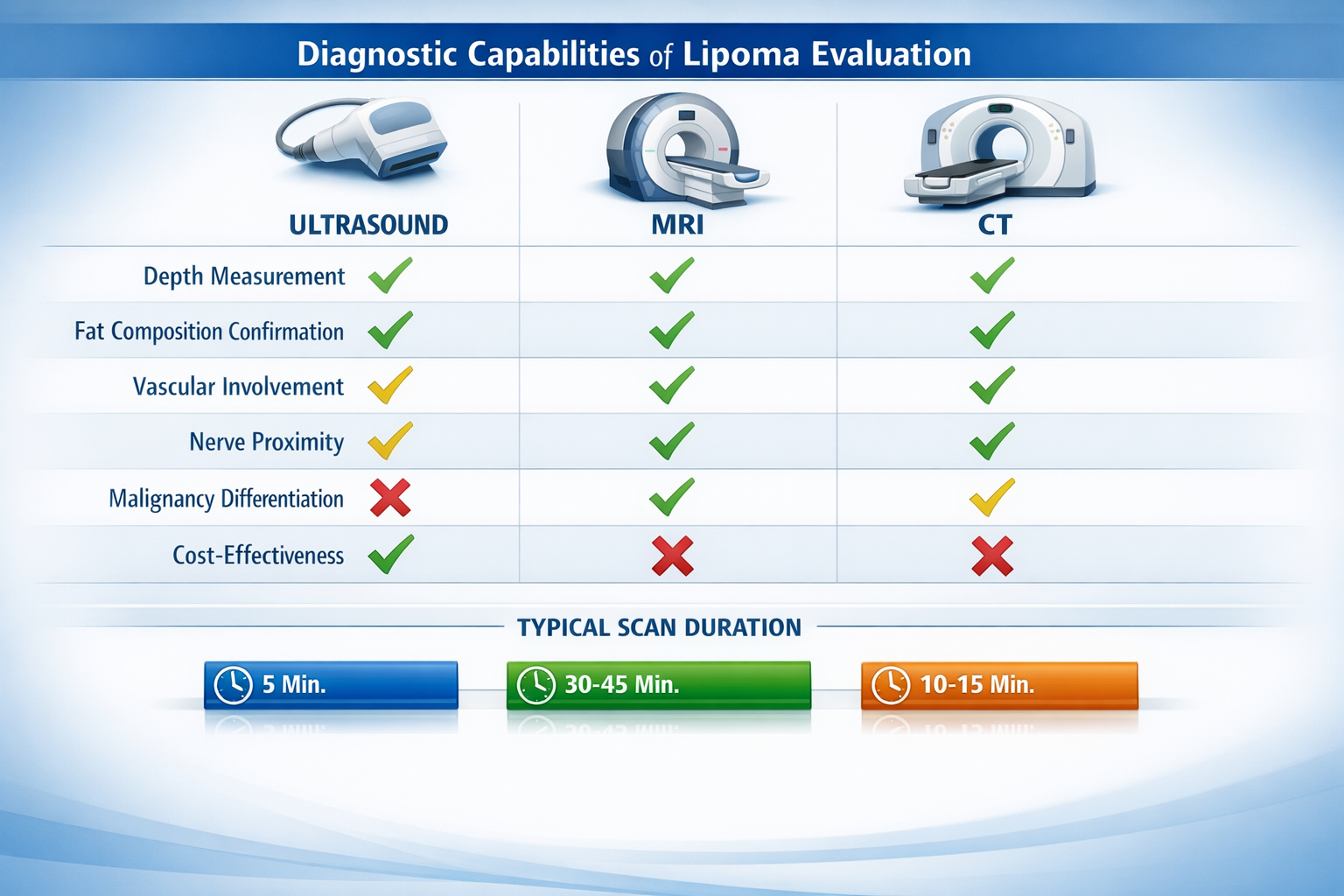
Understanding the strengths and weaknesses of each imaging type helps you and your doctor make informed decisions. The choice depends on lipoma location, size, symptoms, and what specific questions need answering.
FeatureUltrasoundMRICTBest forSuperficial lipomasDeep or suspicious lipomasDeep body cavity lipomasRadiationNoneNoneYesCost$ ($200-500)$$$ ($1,000-3,000)$$ ($500-1,500)Duration15-30 minutes30-60 minutes5-15 minutesSoft tissue detailGoodExcellentFairReal-time imagingYesNoNoClaustrophobia concernNoYesMinimalAvailabilityWidely availableLess availableWidely availableMalignancy detectionFairExcellentFair
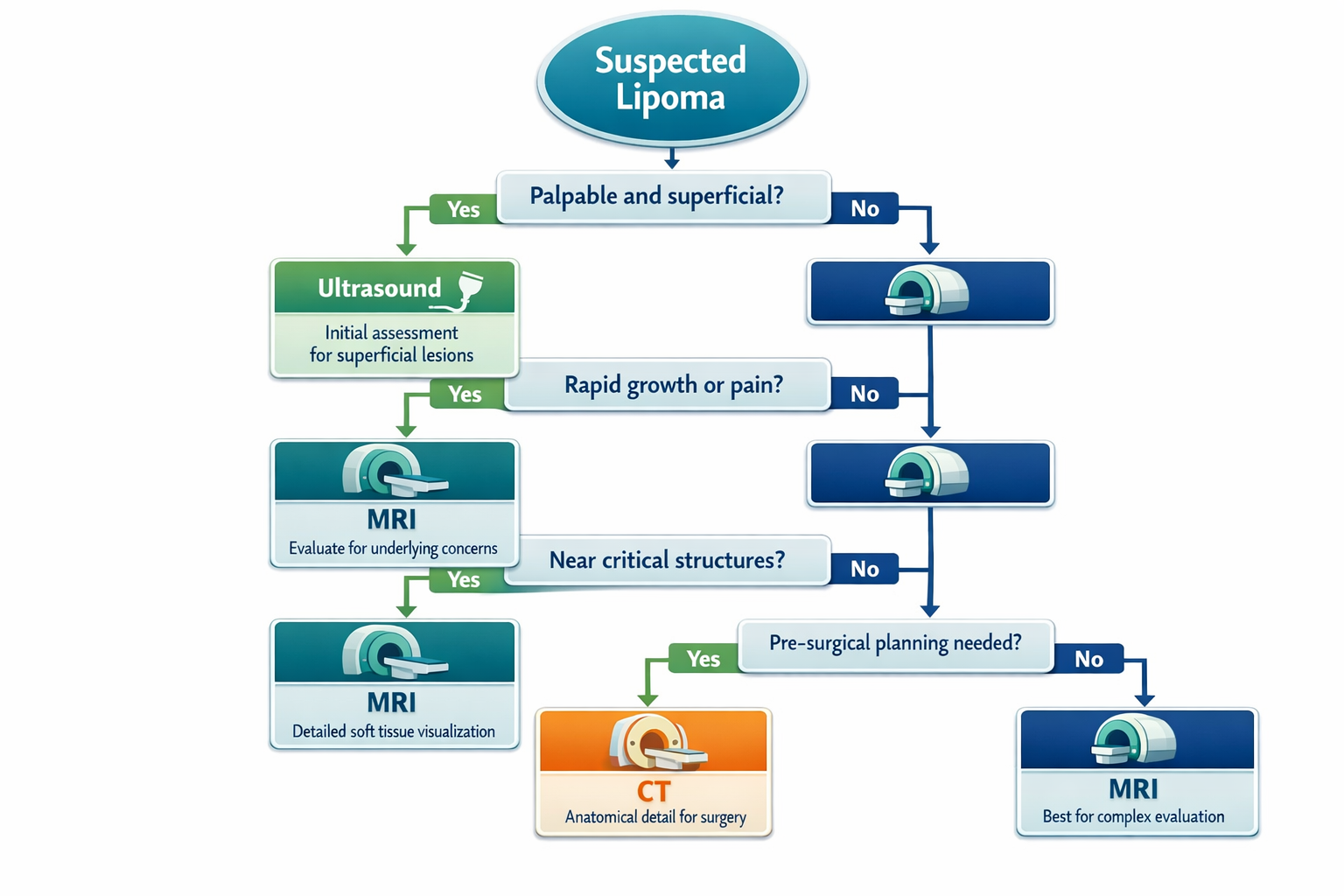
Start with ultrasound when:
Move to MRI when:
Consider CT when:
For more context on lipoma characteristics, visit our comprehensive lipoma information page.
While most lipomas are completely harmless, certain imaging characteristics raise concern for liposarcoma—a malignant fatty tumor that requires different treatment. Radiologists look for specific "red flags" that warrant further investigation.
Size matters: Lipomas larger than 5 cm have a higher likelihood of being liposarcomas, though most large fatty masses are still benign.
Thick septations: Benign lipomas may have thin dividing walls (less than 2 mm), but thick, irregular septations suggest malignancy.
Nodular or solid components: Any area within the fatty mass that doesn't look like pure fat tissue raises concern.
Infiltrative borders: Benign lipomas have well-defined edges, while liposarcomas often have irregular borders that infiltrate surrounding tissue.
Increased vascularity: Excessive blood flow detected on Doppler ultrasound or contrast-enhanced MRI suggests a more aggressive tumor.
Rapid growth: Any fatty mass that doubles in size within months rather than years needs immediate evaluation.
Deep location: Intramuscular or retroperitoneal (behind the abdominal cavity) fatty masses have higher malignancy rates than superficial ones.
If imaging reveals concerning features, the next steps typically include:
Important note: Even when imaging looks suspicious, many masses turn out to be benign variants or other non-cancerous conditions. Imaging provides guidance, not definitive diagnosis.
Learn about the relationship between lipomas and cancer in our article on whether lipomas can turn into cancer.
Cost varies significantly based on imaging type, geographic location, facility (hospital vs. independent imaging center), and insurance coverage. Understanding the financial aspect helps you make informed decisions and avoid surprise bills.
Ultrasound: $200-500 without insurance
MRI: $1,000-3,000 without insurance
CT scan: $500-1,500 without insurance
Medical necessity is key: Insurance typically covers imaging when it's medically necessary—meaning the lipoma has concerning features, symptoms, or requires pre-surgical evaluation.
Prior authorization: Many insurance plans require pre-approval for MRI and CT scans. Your doctor's office usually handles this process, which can take 2-5 business days.
Cosmetic concerns don't qualify: If you want imaging purely because you're considering removal for cosmetic reasons, insurance may deny coverage.
Documentation requirements: Your doctor needs to document why imaging is necessary (size, symptoms, location, atypical features) for insurance approval.
Common mistake: Getting imaging at a hospital when an independent center would cost half as much and provide identical quality.
No, imaging is not always necessary before lipoma removal. Many small, superficial lipomas can be safely removed based on clinical examination alone. However, certain situations make pre-operative imaging valuable or essential.
Large lipomas (over 5 cm): Imaging helps the surgeon understand depth, involvement of surrounding structures, and plan the appropriate surgical approach.
Deep or intramuscular lipomas: The surgeon needs to know the relationship to nerves, blood vessels, and muscle layers to avoid complications.
Lipomas near critical structures: Facial lipomas, neck lipomas, or those near major nerves benefit from detailed anatomical mapping.
Atypical features: If the mass feels firm, fixed, or has grown rapidly, imaging helps rule out malignancy before surgery.
Multiple lipomas: When removing several lipomas in one session, imaging can identify additional masses not obvious on examination.
Previous failed removal: If a lipoma has recurred after prior surgery, imaging helps identify residual tissue and plan complete excision.
Small superficial lipomas (under 3 cm): Typical soft, mobile lumps in the subcutaneous layer can often be removed without imaging.
Clearly benign characteristics: Slow-growing, painless, soft masses with classic lipoma features may not require pre-operative scans.
Experienced surgeon: A surgeon familiar with lipoma removal may feel confident proceeding based on clinical assessment alone.
Patient preference: Some patients prefer to avoid imaging costs if the surgeon is comfortable proceeding without it.
Pre-operative imaging provides surgeons with:
For more information about the removal process, see our guide on how long lipoma removal surgery takes.
Lipoma location significantly affects imaging decisions because different anatomical areas present unique challenges and risks. Some locations require more detailed imaging than others.
Facial lipomas need careful evaluation because of:
Recommended imaging: MRI is typically preferred to map nerve locations and plan minimal-access surgical approaches.
Learn more about facial lipomas and removal options.
Neck lipomas require imaging because:
Recommended imaging: MRI or CT with contrast to visualize vascular structures.
Lipomas within muscle tissue need imaging because:
Recommended imaging: MRI is essential for surgical planning.
Breast lipomas present unique challenges:
Recommended imaging: Ultrasound first, followed by MRI if features are atypical.
Read more about breast lipomas.
These lipomas occur over the sacrum (lower back) and often cause back pain:
Recommended imaging: MRI to assess nerve involvement and rule out other spinal conditions.
Learn about episacral lipomas.
Yes, most typical lipomas can be diagnosed through physical examination alone. Doctors identify lipomas by their characteristic soft, doughy, mobile feel under the skin. Imaging becomes necessary only when the mass has atypical features, causes symptoms, or requires surgical planning.
Ultrasound is highly accurate (85-95%) for identifying typical superficial lipomas and confirming fatty composition. However, it's less reliable for distinguishing benign lipomas from well-differentiated liposarcomas, which is why MRI is recommended when there's any concern about malignancy.
Imaging can identify suspicious features that suggest malignancy, but it cannot definitively diagnose cancer. Only tissue biopsy and pathology examination can confirm whether a fatty mass is benign or malignant. MRI is the best imaging test for detecting concerning features.
Contrast dye is not always necessary. For ultrasound, no contrast is used. For MRI, gadolinium contrast may be added if there's concern about malignancy or if detailed vascular mapping is needed. For CT scans, contrast helps visualize blood vessels and distinguish the lipoma from surrounding structures.
Ultrasound results typically take 24-48 hours. MRI and CT results usually take 2-3 business days. Urgent cases can sometimes be read the same day. Your doctor will receive a formal radiology report and then discuss the findings with you.
Imaging before removal can help ensure complete excision by showing the lipoma's full extent and depth. However, imaging cannot predict recurrence. Recurrence rates are low (1-5%) when lipomas are completely removed, and this depends more on surgical technique than pre-operative imaging.
A single CT scan involves low radiation exposure (equivalent to several months of natural background radiation). The risk is minimal for a one-time scan, but repeated CT scans should be avoided when alternatives like ultrasound or MRI are available. The benefits of necessary imaging typically outweigh the small radiation risk.
You can discuss imaging preferences with your doctor, but the choice should be based on medical appropriateness. Insurance companies require medical justification for imaging orders, so your doctor needs to document why a specific test is necessary. Cost concerns and radiation exposure are valid factors to discuss.
If imaging reveals features that don't match a typical lipoma, your doctor will recommend next steps, which may include biopsy, referral to a specialist, or additional imaging. Many "unexpected" findings turn out to be benign variants or other non-cancerous conditions, so try not to panic before getting complete evaluation.
Not necessarily. A single MRI or ultrasound can often evaluate multiple lipomas in the same body region. If you have lipomas in different areas (arm and leg, for example), separate imaging sessions may be needed. Discuss the most efficient approach with your doctor.
No. Exercise and diet do not reliably shrink lipomas, so they won't eliminate the need for imaging if imaging is medically indicated. Lipomas are not caused by diet or lifestyle factors, and they don't respond to weight loss or exercise programs.
For more information, see our article on whether exercise or diet can shrink lipomas.
If your lipoma is small, stable, painless, and has typical characteristics on examination, imaging is usually unnecessary even if you're aware of it. Many people live with lipomas for years without any imaging or treatment. Imaging becomes appropriate if the lipoma changes, grows, or develops symptoms.
Lipoma imaging explained comes down to matching the right test to the specific clinical situation. Ultrasound serves as the workhorse for most superficial lipomas, providing quick, affordable confirmation of fatty composition without radiation exposure. MRI becomes the gold standard when deeper detail is needed—for large masses, deep-seated lipomas, pre-surgical planning, or when there's any concern about malignancy. CT scans play a limited but valuable role for deep body cavity lipomas or when MRI isn't available.
The key takeaway: not every lipoma needs imaging, and not every imaging test provides the same information. Work with your doctor to determine whether imaging is necessary for your specific situation, and if so, which type will answer the relevant clinical questions most effectively.
If you have a suspected lipoma:
For comprehensive information about lipoma diagnosis, treatment options, and removal procedures, visit The Minor Surgery Center's lipoma resource page or explore our detailed guide on lipoma removal complications.
Remember that imaging is a tool to guide decisions, not an end in itself. The goal is to provide you with accurate diagnosis, appropriate treatment recommendations, and peace of mind—using the most efficient and cost-effective approach for your individual situation.



