Hibernoma — rare brown fat tumor vs. lipoma is a common diagnostic question when a fatty lump does not look like a routine lipoma on exam or imaging. A hibernoma is a rare, benign tumor made of brown fat, while a lipoma is a common, benign tumor made of white fat. Hibernomas are usually not cancerous, but they can look active on PET scans and can mimic more serious soft-tissue tumors, so imaging, biopsy, or specialist review may be needed.
Clinical note: Most soft, movable fatty lumps are lipomas, not hibernomas. The concern rises when a “fatty” lump is deep, unusually vascular, rapidly enlarging, or has atypical imaging features.
A hibernoma is a rare, benign soft-tissue tumor made from brown fat, while a lipoma is a common, benign tumor made from white fat. The key difference is that brown fat is more metabolically active and often more vascular, so hibernomas can look more complex on imaging than a typical lipoma.
Brown fat helps produce heat. In adults, small amounts of brown fat may remain in areas such as the neck, shoulder, back, chest, and around deeper tissues. A hibernoma forms when brown fat cells grow into a mass.
A lipoma is different. It forms from white fat, which stores energy. Lipomas are far more common and often appear as soft, rubbery, mobile lumps under the skin.
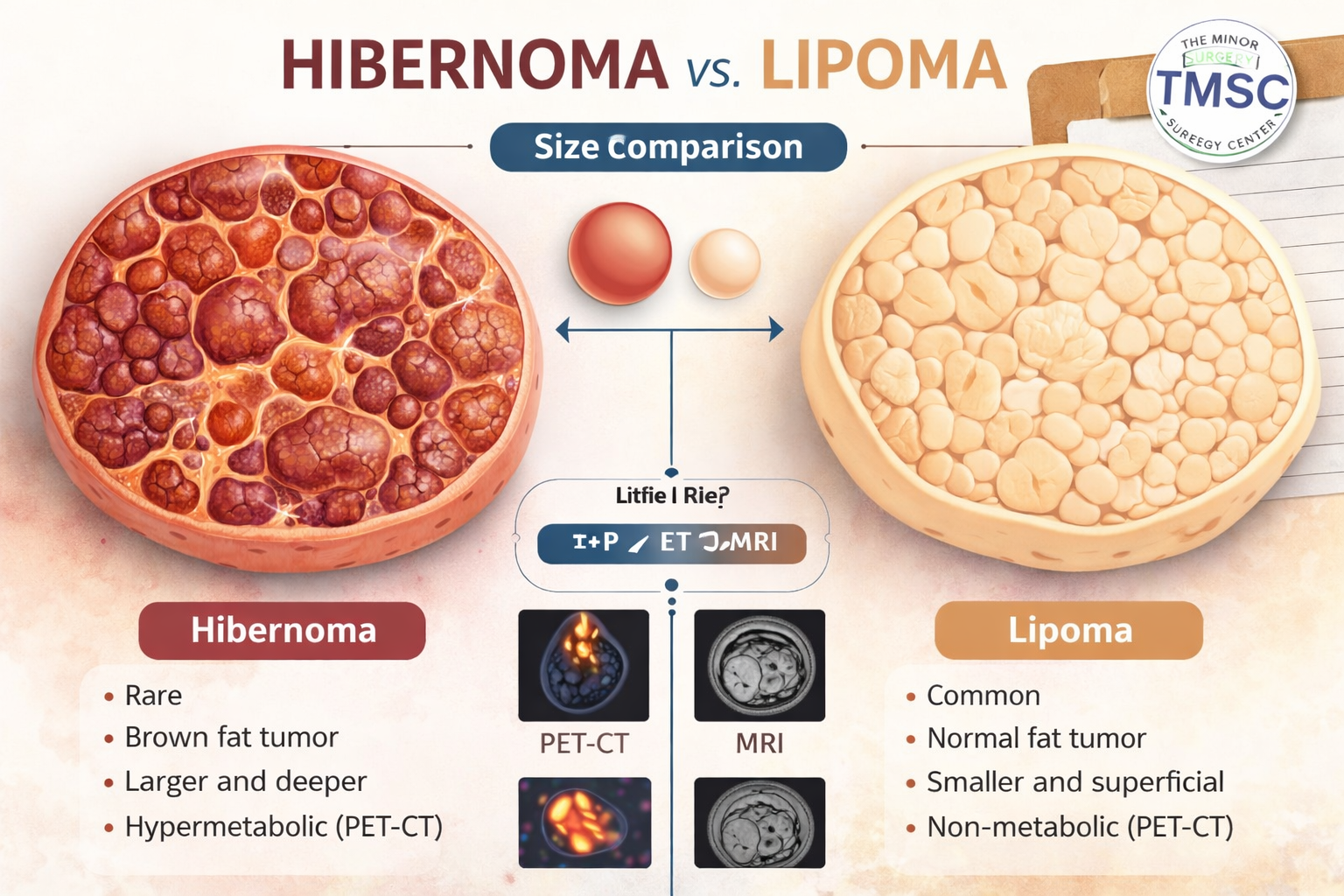
Hibernoma — rare brown fat tumor vs. lipoma can be understood as “active brown fat lump” versus “common white fat lump.” Both are usually benign, but hibernomas are less familiar, more vascular, and more likely to need imaging or biopsy before removal.
FeatureHibernomaLipomaTissue typeBrown fatWhite fatFrequencyRareCommonUsual behaviorBenign, slow-growingBenign, slow-growingFeelMay be firm or deepOften soft and movableImagingMore vascular, mixed fat signalSmooth, homogeneous fat signalPET/CTMay be FDG-avidUsually not FDG-avidTreatmentExcision if symptomatic, growing, or uncertainObservation or removal if bothersome
Decision rule: Choose medical assessment sooner if a presumed lipoma is deep, growing, painful, fixed, larger than expected, or different from previous lumps.
For patients who already know they have a likely lipoma, TMSC offers information on lipoma removal options, including how surgical assessment and removal are commonly approached.
Hibernoma is very rare compared with lipoma. Published reviews describe hibernoma as a small fraction of benign fatty tumors, while lipoma is one of the most common benign soft-tissue lumps seen in clinical practice [1][2].
A large Armed Forces Institute of Pathology review cited in recent literature described 170 hibernoma cases, with typical hibernoma making up most cases and the thigh being a frequent location [1]. Other reports note that hibernoma accounts for roughly 1% to 2% of benign lipomatous tumors, depending on the series and definitions used [1][2].
Hibernomas often appear in adults, with many cases diagnosed in the third or fourth decade of life. A slight male predominance has been reported in some series [1]. Common sites include:
Lipomas, by contrast, can occur almost anywhere fat exists. They are often found on the trunk, shoulders, arms, neck, and thighs.
The most common mistake is treating every soft-tissue lump as a simple lipoma without checking for red flags. Most are harmless, but deep or unusual masses should be reviewed.
A lump deserves further assessment when it is:
For a broader guide to distinguishing fatty tumors from other masses, see TMSC’s article on differentiating lipomas from other soft-tissue masses.
Most hibernomas and lipomas are painless, slow-growing lumps. Symptoms are more likely when the mass is deep, large, pressing on nearby structures, or located where movement causes irritation.
A typical lipoma may feel:
A hibernoma may feel similar, but it may also be:
Hibernomas can be found incidentally during imaging done for another reason. A 2025 case report described an incidental FDG-avid hibernoma in the subscapularis muscle that mimicked metastatic disease before biopsy confirmed the diagnosis [7].
Pain does not automatically mean cancer. A benign lipoma can hurt if it presses on a nerve, sits under tight tissue, or gets irritated by pressure. A hibernoma can also cause discomfort because of its size or location.
Decision rule: Choose prompt assessment if pain is paired with growth, firmness, deep location, weakness, numbness, or limited movement.
Some hibernomas occur in deeper sites, including the mediastinum, which is the central part of the chest. These cases are uncommon and can be mistaken for more serious tumors because of location and imaging activity. Multidisciplinary review may be needed when the mass is near major blood vessels, nerves, or organs.
Doctors diagnose hibernoma vs. lipoma using clinical exam, imaging, and sometimes biopsy. A simple superficial lipoma may be diagnosed by exam, but suspected hibernoma usually needs imaging because it can overlap with other fatty tumors.
The diagnostic path often follows this order:
Hibernoma — rare brown fat tumor vs. lipoma often becomes clear on imaging when the mass is not a smooth, simple fatty lump. Hibernomas may show incomplete fat suppression, thin internal septa, prominent vessels, and hypervascularity, while lipomas are usually homogeneous and less vascular [1].
On MRI, hibernomas are often described as:
Lipomas are usually:
Hibernoma can show high FDG uptake because brown fat uses glucose. Recent literature describes hibernoma SUVmax values that may be higher than values reported for some liposarcomas, which can create diagnostic concern [7][10].
Common mistake: A high SUV on PET/CT should not be treated as proof of cancer. Hibernoma is a benign reason for high FDG uptake, but biopsy may still be needed when imaging overlaps with malignancy.
Yes, hibernoma can be confused with atypical lipomatous tumor, well-differentiated liposarcoma, or other soft-tissue tumors. Imaging can narrow the diagnosis, but pathology is the final answer when the features are unclear.
The key concern is not usually hibernoma versus lipoma alone. The bigger clinical question is whether an unusual fatty mass could be a liposarcoma or another tumor that needs a different treatment plan.
Atypical lipomatous tumor and well-differentiated liposarcoma may show:
Hibernoma may show:
Other diagnoses may enter the discussion depending on imaging and location:
Decision rule: Choose biopsy or specialist referral when imaging shows thick septa, nodules, marked vascularity, deep muscle involvement, rapid growth, or unclear margins.
Patients concerned about cancer risk can also read TMSC’s guide on whether a lipoma can turn into cancer. The short answer is that ordinary lipomas do not become cancer, but some malignant tumors can resemble lipomas at first.
Pathology confirms hibernoma by showing brown fat cells with multiple small fat vacuoles and granular cytoplasm. Lipoma pathology shows mature white fat cells that look more uniform.
Under the microscope, hibernoma cells are often described as multivacuolated brown fat cells. The tumor may also contain a rich blood supply. This microscopic appearance helps distinguish hibernoma from ordinary lipoma and from malignant fatty tumors.
A major pathology review cited in recent literature classifies hibernomas into several subtypes [1]:
The lipoma-like subtype can be especially confusing because it may resemble a standard lipoma more closely. This is one reason pathology matters when the imaging or surgical findings are not typical.
Even when a lump seems benign, sending tissue for pathology can confirm the diagnosis. Pathology can:
Common mistake: Skipping pathology after removal of an atypical fatty mass may miss important information. A routine superficial lipoma may be low concern, but deep or unusual masses should be documented carefully.
Hibernoma treatment is usually surgical excision when the tumor is symptomatic, enlarging, deep, cosmetically bothersome, or diagnostically uncertain. Observation may be reasonable in select confirmed benign cases, but many hibernomas are removed because imaging can overlap with other tumors.
Surgery for hibernoma is different from simple lipoma removal when the mass is deep or vascular. Hibernomas may have more blood supply, so surgical planning matters.
SituationUsual approachSmall, classic superficial lipomaObservation or local excisionPainful or bothersome lipomaOffice-based or minor surgical removal when appropriateDeep fatty massMRI and specialist reviewSuspected hibernomaMRI, possible biopsy, planned excisionVascular or complex hibernomaSurgical planning, possible embolization in select casesConcern for liposarcomaReferral to appropriate specialist team
A January 2026 case report described an intermuscular thigh hibernoma with an associated arteriovenous malformation that was managed with preoperative embolization before surgery [6]. That type of case is not the norm, but it shows why vascularity matters.
Surgical removal may include:
For straightforward lipomas, care may be simpler. TMSC provides surgical care for common benign lumps through clinics such as the Whitby Mole, Cyst, Lipoma & Carpal Tunnel Surgery Center and the Toronto Mole, Cyst, Lipoma & Carpal Tunnel Surgery Center.
Choose minor surgery clinic assessment if the lump is likely a superficial lipoma, bothersome, growing slowly, and not attached to deep structures.
Choose advanced imaging or specialist referral if the mass is deep, vascular, recurrent, fast-growing, or suspicious for a non-lipoma diagnosis.
For patients comparing approaches, TMSC also explains when to see a dermatologist or general surgeon for lipoma removal.
Recovery depends on the size, depth, location, and complexity of the lump. A small superficial lipoma often has a simpler recovery, while a deep hibernoma may require more planning, a larger incision, and a longer return to full activity.
Most patients can expect some swelling, bruising, tightness, or tenderness after fatty tumor removal. The surgical team should provide wound care instructions, activity limits, and warning signs.
Follow the surgeon’s instructions, but these principles are common:
Scarring depends on incision length, location, skin tension, genetics, and wound care. Board-certified surgeons plan incisions to remove the mass safely while respecting cosmetic outcomes where possible.
TMSC’s article on before and after lipoma removal explains what patients commonly want to know about appearance, healing, and expectations after removal.
Heavy lifting or stretching too soon can increase swelling, bleeding, wound tension, or fluid collection. This is especially relevant when a mass was deep or located near a muscle group.
Decision rule: Return to activity only after the surgeon confirms that the incision and deeper tissues can tolerate movement.
The cost and timeline depend on whether the lump is a simple lipoma or a suspected hibernoma needing imaging, biopsy, or specialist coordination. Simple lipoma assessment and removal may be faster, while deep or atypical masses take longer because safety planning comes first.
A hibernoma workup may involve several steps:
A simple lipoma may require fewer steps, especially when it is superficial and clinically typical. However, a lump that looks like a lipoma but behaves differently should not be rushed.
Costs may vary based on:
Because fees and coverage rules vary, patients should request a clear quote after assessment. TMSC’s minor skin surgery FAQ is a useful starting point for common questions about booking, procedures, and what to expect.
Timeline may be shorter when:
Timeline may be longer when:
Decision rule: Speed should not override diagnostic accuracy. A short delay for MRI or biopsy is often safer than removing an unclear deep mass without a plan.
A patient should see a specialist when a fatty lump is deep, enlarging, painful, recurrent, vascular, or unclear on imaging. Specialist assessment is also appropriate when the lump is near nerves, blood vessels, joints, or important cosmetic areas.
Hibernoma — rare brown fat tumor vs. lipoma is not always a bedside diagnosis. A board-certified surgeon can decide whether the lump looks like a routine lipoma or needs imaging, biopsy, or referral.
Seek medical assessment if a lump:
TMSC is best suited for patients seeking expedited specialist assessment of common benign skin and soft-tissue concerns, including lipomas, cysts, moles, and related lesions. Complex deep tumors may need imaging, biopsy, or referral pathways based on clinical findings.
Patients can review TMSC’s broader list of benign and malignant skin conditions to understand what types of lesions are commonly assessed and treated.
Hospital-based care may be more appropriate when:
Common mistake: Choosing removal based only on convenience. The safest setting is the one that matches the mass, not the calendar.
No. A hibernoma is considered a benign tumor of brown fat. Published reviews cited in recent literature report no malignant transformation [1].
Hibernoma is not known to turn into liposarcoma. The concern is that hibernoma can mimic liposarcoma on imaging, so biopsy may be needed when features overlap.
No. A lipoma is made of white fat, while a hibernoma is made of brown fat. Lipomas are common; hibernomas are rare.
Hibernoma can show FDG uptake because brown fat is metabolically active and uses glucose. This can make a benign hibernoma look concerning on PET/CT [7][10].
The thigh, shoulder, and back are commonly reported sites. Hibernoma can also occur in deeper locations, including intermuscular areas [1][2].
Not always, but many are removed because they are symptomatic, enlarging, or difficult to distinguish from other tumors. The decision depends on imaging, biopsy results, location, and patient factors.
Ultrasound may show a fatty or vascular mass, but it usually cannot confirm hibernoma with certainty. MRI and pathology are often more helpful for atypical or deep lesions.
It can be. Hibernomas may be deeper and more vascular than routine lipomas, so surgical planning is important.
No reliable evidence shows that diet or exercise can shrink a hibernoma. The same is generally true for established lipomas.
A painful lipoma may be removed if it causes discomfort, pressure, cosmetic concern, or diagnostic uncertainty. A clinician should first confirm that the lump is likely benign.
Hibernoma is rare, benign, and often treatable, but it deserves careful attention because it can look like a lipoma, an atypical fatty tumor, or even cancer on imaging. Lipoma is far more common and usually straightforward, but the safest path depends on the lump’s depth, growth pattern, symptoms, and imaging features.
Actionable next steps:
For a likely lipoma, patients can begin with TMSC’s guide to lipoma removal. For an atypical mass, the right first step is a careful assessment that protects both diagnosis and outcome.
[1] S2210261224010101 - https://www.sciencedirect.com/science/article/pii/S2210261224010101
[2] academic.oup - https://academic.oup.com/jscr/article/2023/5/rjad309/7185490
[3] 24149 Hibernoma - https://my.clevelandclinic.org/health/diseases/24149-hibernoma
[4] Paperinformation - https://www.scirp.org/journal/paperinformation?paperid=33970
[5] S11552 014 9726 7 - https://journals.sagepub.com/doi/10.1007/s11552-014-9726-7
[6] 448935 Intermuscular Hibernoma Of The Thigh A Diagnostic And Surgical Challenge Managed With Preoperative Embolization - https://www.cureus.com/articles/448935-intermuscular-hibernoma-of-the-thigh-a-diagnostic-and-surgical-challenge-managed-with-preoperative-embolization
[7] Pmc12659797 - https://pmc.ncbi.nlm.nih.gov/articles/PMC12659797/
[8] Pmc6711274 - https://pmc.ncbi.nlm.nih.gov/articles/PMC6711274/
[9] 136425 Rare Cases Of Hibernomas Associated With Bilateral Pheochromocytoma A Report Of Two Cases - https://www.cureus.com/articles/136425-rare-cases-of-hibernomas-associated-with-bilateral-pheochromocytoma-a-report-of-two-cases
[10] Ajr.07 - https://ajronline.org/doi/10.2214/AJR.07.3061
Last updated: April 28, 2026



