Dermatofibroma vs Dermatofibrosarcoma Protuberans: Understanding the Critical Differences
When a firm bump appears on your skin, it's natural to wonder what it could be. While most skin growths are harmless, understanding the difference between dermatofibroma vs dermatofibrosarcoma protuberans can be crucial for your health. These two conditions may sound similar, but they represent vastly different diagnoses—one is a common benign growth, while the other is a rare form of skin cancer that requires immediate medical attention.
This comprehensive guide will help you understand the key distinctions between these two skin conditions, recognize warning signs, and know when to seek professional medical evaluation. Whether you've noticed a new skin lesion or have been referred for further testing, this information will empower you to make informed decisions about your skin health.
Key Takeaways
🔍 Dermatofibromas are common, benign (non-cancerous) skin nodules that typically appear on the legs and are harmless, while dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing skin cancer that requires aggressive surgical treatment.
📏 Size and growth patterns are critical distinguishing factors: dermatofibromas remain small (usually under 1 cm) and stable, whereas DFSP lesions progressively enlarge over months to years and can reach several centimeters.
🩺 Definitive diagnosis requires a skin biopsy with histopathological examination, as visual inspection alone cannot reliably differentiate between these conditions.
⚕️ Treatment approaches differ dramatically: dermatofibromas often need no treatment unless bothersome, while DFSP requires wide surgical excision or Mohs surgery to prevent recurrence.
⏱️ Early detection of DFSP significantly improves treatment outcomes and reduces the risk of recurrence, making professional evaluation of any suspicious or changing skin lesion essential.
What Is a Dermatofibroma?
A dermatofibroma (also called a fibrous histiocytoma) is one of the most common benign skin growths that dermatologists encounter. These small, firm nodules develop within the dermis—the middle layer of skin—and are composed primarily of fibroblasts (cells that produce collagen) and histiocytes (immune cells).
Characteristics of Dermatofibromas
Dermatofibromas present with several distinctive features that help identify them:
Physical Appearance:
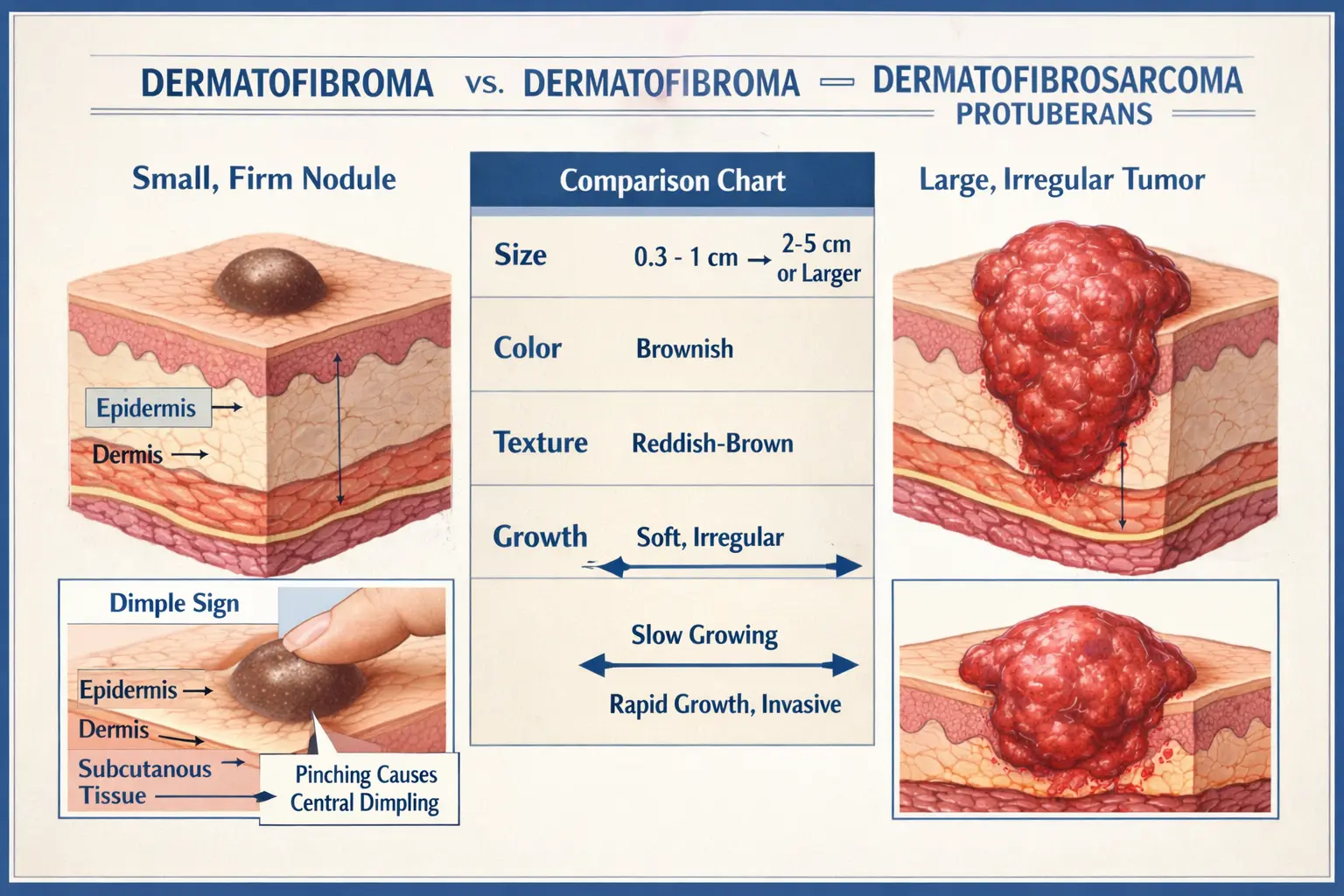
Size: Typically 0.5 to 1.5 cm in diameter (about the size of a pencil eraser)
Color: Range from pink, red, or brown to gray or black
Texture: Firm, hard nodules that feel like a small button beneath the skin
Location: Most commonly appear on the lower legs, though they can occur anywhere on the body
Surface: Usually smooth, though some may have a slightly rough or scaly surface
The Dimple Sign 🔬
One of the most characteristic features of a dermatofibroma is the "dimple sign" or "Fitzpatrick's sign." When you squeeze the sides of the lesion between your thumb and forefinger, a dermatofibroma will typically dimple or indent inward. This occurs because the fibrous tissue is tethered to the overlying skin. This simple test can help distinguish dermatofibromas from other skin lesions, though it's not 100% reliable.
Causes and Risk Factors
The exact cause of dermatofibromas remains unclear, but several theories exist:
Minor trauma: Many people report that their dermatofibroma appeared after a minor injury, insect bite, or splinter
Immune response: The lesion may represent an exaggerated healing response to minor skin trauma
Genetic factors: Some individuals may be more predisposed to developing these growths
Who Gets Dermatofibromas?
More common in women than men
Typically appear in young to middle-aged adults (20-40 years old)
Can occur in people of all skin types and ethnicities
Multiple dermatofibromas are less common but can occur
Symptoms and Behavior
Most dermatofibromas are asymptomatic, meaning they cause no symptoms. However, some people may experience:
Mild tenderness when pressed
Occasional itching
Sensitivity to touch or pressure (especially if located where clothing rubs)
Cosmetic concern, particularly on visible areas
Important characteristics:
Slow or no growth: Dermatofibromas typically remain stable in size or grow very slowly
Permanent: They rarely disappear on their own
No cancer risk: Dermatofibromas do not transform into cancer
Multiple lesions: Some people develop several dermatofibromas over time
For more information about various types of benign skin lesions, visit our comprehensive guide on 25 types of skin lesions.
What Is Dermatofibrosarcoma Protuberans (DFSP)?
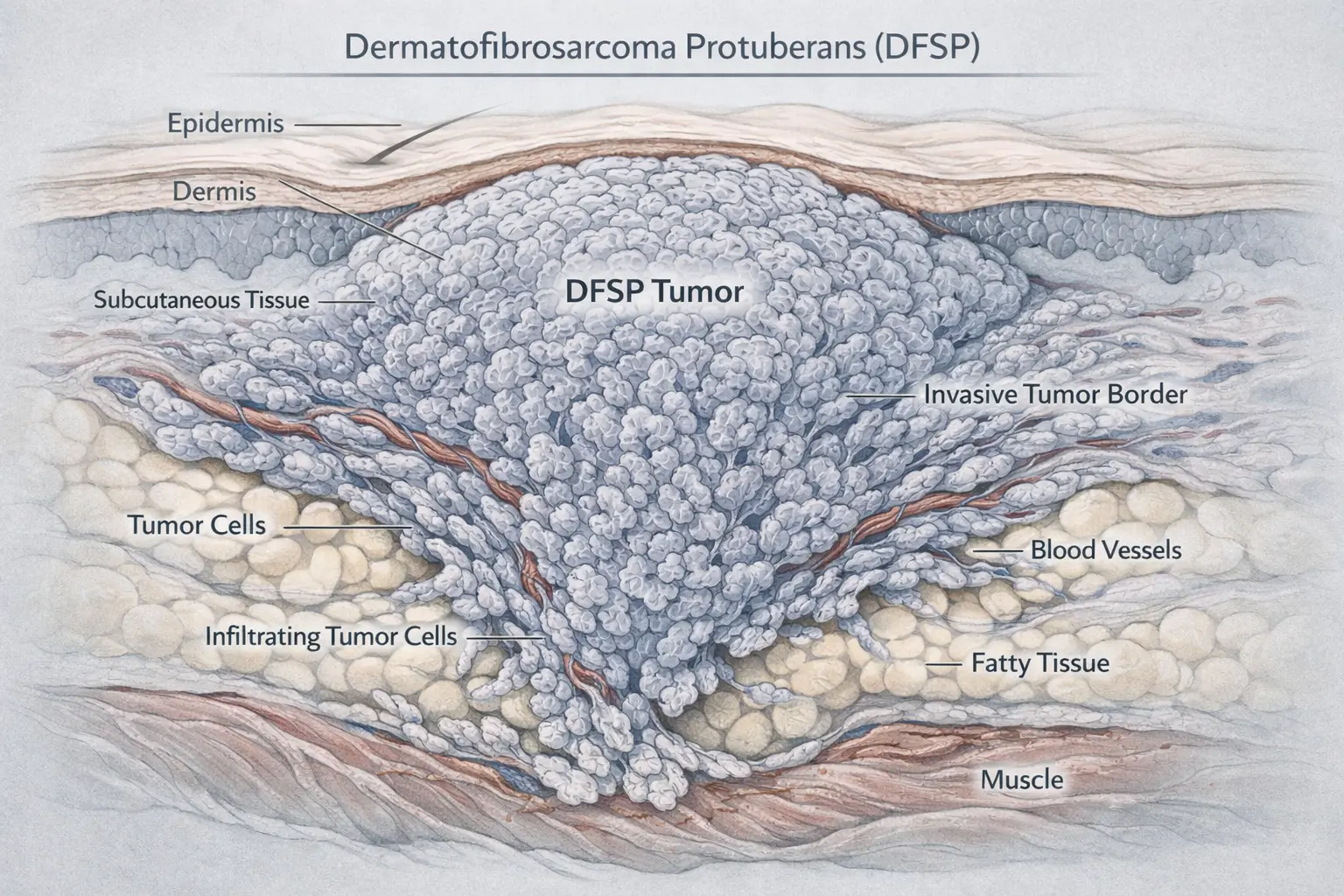
Dermatofibrosarcoma protuberans (DFSP) is a rare, slow-growing skin cancer that develops in the connective tissue of the dermis. Unlike dermatofibromas, DFSP is a malignant tumor that requires aggressive treatment. The term "protuberans" refers to the tumor's tendency to protrude or bulge from the skin surface as it grows.
Characteristics of DFSP
DFSP presents quite differently from benign dermatofibromas:
Physical Appearance:
Size: Usually larger than dermatofibromas, ranging from 1 to 5 cm or more
Color: Typically reddish-brown, purple, or flesh-colored
Texture: Initially firm and flat, later becoming raised and nodular
Location: Most commonly appears on the trunk (chest, back, abdomen), followed by extremities and head/neck
Surface: May appear as a plaque-like thickening initially, later developing into nodules
Growth Pattern 📈
DFSP exhibits a characteristic growth pattern that distinguishes it from benign lesions:
Initial phase: Appears as a flat or slightly raised, firm plaque
Progressive enlargement: Slowly grows over months to years
Nodular development: Eventually forms one or more protruding nodules
Infiltrative growth: Extends tentacle-like projections deep into surrounding tissue
Epidemiology and Risk Factors
DFSP is considered a rare malignancy with specific demographic patterns:
Incidence:
Accounts for less than 0.1% of all malignant tumors
Approximately 1,000 new cases diagnosed annually in the United States[1]
Represents about 1-2% of all soft tissue sarcomas
Risk Factors:
Age: Most commonly diagnosed between ages 20-50
Gender: Slightly more common in males
Race: Higher incidence in Black individuals compared to other racial groups
Previous trauma: Some cases report a history of trauma to the affected area
Genetic factors: Associated with chromosomal translocation t(17;22) creating the COL1A1-PDGFB fusion gene[2]
Clinical Behavior and Prognosis
Understanding how DFSP behaves is crucial for appropriate management:
Growth Characteristics:
Slow progression: Can take years to reach a noticeable size
Local aggression: Invades surrounding tissue with finger-like projections
Low metastatic potential: Rarely spreads to distant organs (less than 5% of cases)[3]
High local recurrence: Without adequate surgical margins, recurrence rates can exceed 50%
Metastatic Potential:
While DFSP is technically a low-grade sarcoma with minimal metastatic potential, certain factors increase risk:
Fibrosarcomatous transformation: Occurs in 10-15% of cases and increases metastatic risk
Multiple recurrences: Each recurrence may increase aggressive behavior
Large tumor size: Tumors larger than 5 cm carry higher risk
Deep invasion: Extension into muscle or bone indicates more aggressive disease
To learn more about different types of skin cancer and their characteristics, explore our resource on 4 types of skin cancer.
Dermatofibroma vs Dermatofibrosarcoma Protuberans: Key Differences
Understanding the critical distinctions between dermatofibroma vs dermatofibrosarcoma protuberans can be lifesaving. While these conditions share some superficial similarities, they differ fundamentally in their nature, behavior, and required treatment.
Comparison Table
FeatureDermatofibromaDermatofibrosarcoma ProtuberansNatureBenign (non-cancerous)Malignant (cancerous)Typical Size0.5-1.5 cm1-5+ cmGrowth RateStable or very slowProgressive enlargementColorPink, brown, red, grayReddish-brown, purple, flesh-coloredTextureFirm noduleInitially flat, later nodularDimple SignUsually positiveNegativeCommon LocationLower legsTrunk, extremitiesAge of Onset20-40 years20-50 yearsGender PreferenceMore common in womenSlightly more common in menSymptomsUsually noneUsually none initiallyMetastatic RiskNone (benign)Low but present (<5%)Recurrence After RemovalRareHigh without adequate marginsTreatmentOften none neededWide surgical excision required
Clinical Differences
Appearance Evolution:
Dermatofibroma:
Appears relatively suddenly (though may follow minor trauma)
Remains stable in size and appearance for years
Color may darken slightly over time
Rarely changes significantly
DFSP:
Develops gradually over months to years
Continuously enlarges, though slowly
May evolve from flat plaque to raised nodules
Progressive change is the hallmark
Location Patterns:
While both conditions can theoretically occur anywhere on the body, their typical locations differ:
Dermatofibroma preferences:
🦵 Lower legs (most common)
Arms
Upper back
Rarely on face or hands
DFSP preferences:
🫁 Trunk (40-50% of cases)
Proximal extremities (30-40%)
Head and neck (10-15%)
Distal extremities (less common)
Microscopic Differences
Under the microscope, these lesions look completely different:
Dermatofibroma histology:
Well-circumscribed but not encapsulated
Composed of spindle-shaped fibroblasts and histiocytes
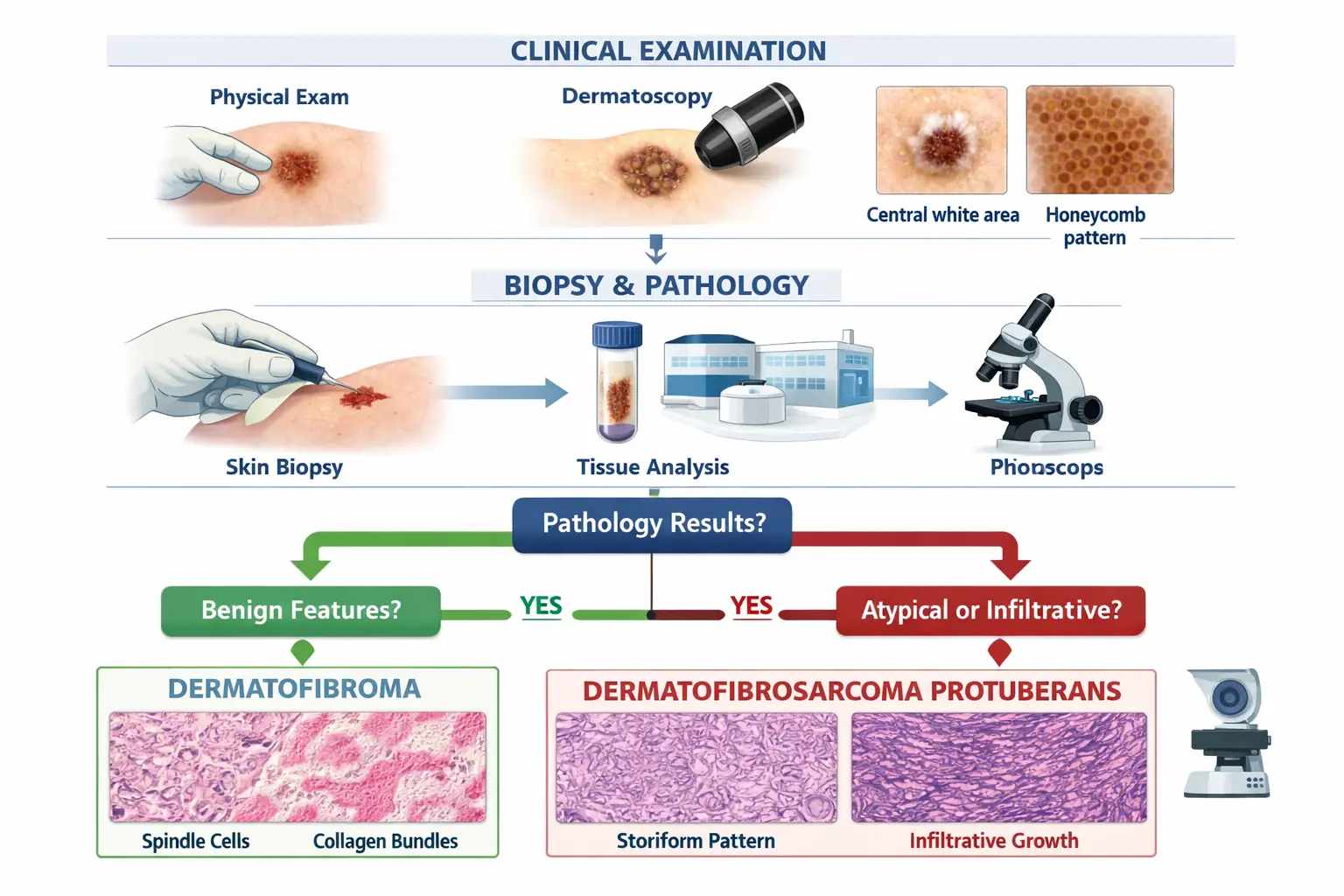
Collagen bundles arranged in a storiform (cartwheel) pattern
Overlying epidermal hyperplasia (thickening)
Hemosiderin deposits (iron pigment) often present
Trapped collagen at the periphery
DFSP histology:
Infiltrative growth pattern extending into subcutaneous fat
Uniform spindle cells arranged in tight storiform pattern
"Honeycomb" pattern when invading fat
High cellularity with minimal atypia
Positive for CD34 marker (important diagnostic feature)
COL1A1-PDGFB fusion gene detectable in most cases
Behavioral Differences
The most critical difference lies in how these lesions behave:
Dermatofibroma behavior: ✅ Remains localized ✅ Does not invade deeply ✅ Cannot spread to other organs ✅ Does not transform into cancer ✅ May persist indefinitely but causes no harm
DFSP behavior: ⚠️ Invades surrounding tissue aggressively ⚠️ Extends deep projections into subcutaneous tissue ⚠️ Can recur locally if not completely removed ⚠️ Rare but possible metastasis to lungs or lymph nodes ⚠️ Requires definitive treatment to prevent progression
"The key to distinguishing dermatofibroma from dermatofibrosarcoma protuberans lies not just in appearance, but in growth behavior. Any skin lesion that progressively enlarges over months warrants professional evaluation and possible biopsy." - Dermatology Clinical Guidelines
Diagnosis: How to Tell Them Apart
Accurate diagnosis is essential when evaluating dermatofibroma vs dermatofibrosarcoma protuberans. While clinical examination provides important clues, definitive diagnosis requires histopathological examination.
Dermoscopy (also called dermatoscopy) uses a specialized magnifying device to examine skin lesions in detail:
Dermatofibroma dermoscopic features:
Central white scar-like area
Peripheral delicate pigment network
Vascular pattern may be present
Homogeneous appearance
DFSP dermoscopic features:
Less specific patterns
May show irregular vascular structures
Heterogeneous appearance
No characteristic diagnostic pattern
Biopsy Techniques
When clinical examination raises suspicion, a biopsy is necessary for definitive diagnosis:
Types of Biopsy:
Punch Biopsy
Uses a circular blade to remove a cylindrical core of tissue
Typically 3-6 mm in diameter
Provides full-thickness sample
Most common initial diagnostic approach
May miss diagnosis if DFSP is sampled at periphery
Incisional Biopsy
Removes a portion of larger lesions
Useful for large or deep tumors
Provides tissue for diagnosis before definitive surgery
Preferred when DFSP is suspected
Excisional Biopsy
Removes entire lesion with small margin
Both diagnostic and potentially therapeutic
Appropriate for small lesions
May be inadequate for DFSP if margins are insufficient
Biopsy Considerations:
For suspected dermatofibroma:
Biopsy often not necessary if clinical diagnosis is clear
May be performed if appearance is atypical
Punch biopsy usually sufficient
For suspected DFSP:
Biopsy is mandatory
Should include sufficient depth
Multiple biopsies may be needed for large lesions
Incisional biopsy preferred over punch biopsy
Histopathological Analysis
The pathologist examines the biopsy specimen microscopically:
Standard Staining:
Hematoxylin and eosin (H&E) staining reveals cellular architecture
Identifies cell types and growth patterns
Assesses invasion depth
Immunohistochemistry:
CD34: Strongly positive in DFSP (90-95% of cases), negative in dermatofibroma
Factor XIIIa: Positive in dermatofibroma, negative in DFSP
Stromelysin-3: Positive in dermatofibroma
Apolipoprotein D: Positive in dermatofibroma
Molecular Testing:
FISH (Fluorescence In Situ Hybridization): Detects COL1A1-PDGFB fusion gene in DFSP
RT-PCR: Confirms fusion transcript
Particularly useful in ambiguous cases
Imaging Studies
While not routinely necessary for dermatofibromas, imaging may be valuable for DFSP:
MRI (Magnetic Resonance Imaging):
Best modality for assessing DFSP extent
Defines depth of invasion
Identifies involvement of underlying structures
Helps plan surgical approach
Recommended before surgical treatment of DFSP
Ultrasound:
Can assess lesion depth
Distinguishes solid from cystic lesions
Less detailed than MRI
May be useful for initial evaluation
CT Scan:
Less commonly used for soft tissue tumors
May be ordered if metastatic disease is suspected
Useful for detecting lung metastases in advanced cases
For expert evaluation of suspicious skin lesions, consider visiting a specialized skin cancer clinic where comprehensive diagnostic services are available.
Treatment Options
The treatment approaches for dermatofibroma vs dermatofibrosarcoma protuberans differ dramatically, reflecting their fundamentally different natures.
Treatment of Dermatofibroma
Since dermatofibromas are benign, treatment is optional and based on patient preference:
Observation (Watchful Waiting) 👁️
Most dermatofibromas require no treatment:
Monitor for any changes in size, color, or symptoms
Photograph lesion for comparison
Annual skin examinations
Reassurance about benign nature
Indications for treatment:
Cosmetic concerns
Symptomatic lesions (pain, itching, tenderness)
Frequent irritation from clothing or shaving
Patient anxiety despite reassurance
Diagnostic uncertainty
Surgical Excision:
When removal is desired, options include:
Simple Excision
Removes entire lesion with small margin
Performed under local anesthesia
Typically leaves a linear scar
Scar may be more noticeable than original lesion
Recurrence is rare
Shave Excision
Removes raised portion of lesion
Leaves deep component behind
Less scarring than full excision
Higher recurrence rate (up to 20%)
May be preferred for cosmetic reasons
Non-Surgical Options:
Cryotherapy
Freezing with liquid nitrogen
May flatten lesion but rarely eliminates it completely
Multiple treatments often needed
Can cause hypopigmentation (lightening of skin)
Best for small, minimally raised lesions
Laser Therapy
Various laser types have been tried
Limited evidence of effectiveness
May improve appearance but rarely eliminates lesion
Expensive and not typically covered by insurance
Intralesional Corticosteroid Injection
May flatten prominent lesions
Temporary effect
Risk of skin atrophy and depigmentation
Not commonly used
Important Considerations:
The scar from surgical removal may be more noticeable than the original dermatofibroma
Patients should have realistic expectations about cosmetic outcomes
Treatment is elective, not medically necessary
Insurance may not cover removal for purely cosmetic reasons
Treatment of Dermatofibrosarcoma Protuberans
DFSP requires definitive surgical treatment due to its malignant nature and tendency for local recurrence:
Surgical Treatment (Primary Approach) ✂️
Surgery is the cornerstone of DFSP treatment:
Wide Local Excision (WLE)
Standard surgical approach
Removes tumor with wide margins (typically 2-4 cm)
Excision extends to deep fascia or muscle
Recurrence rate: 10-20% with adequate margins[4]
May require skin grafting or flap reconstruction
Mohs Micrographic Surgery
Specialized technique with highest cure rates
Sequential removal and microscopic examination of tissue layers
Preserves maximum healthy tissue
Allows real-time margin assessment
Recurrence rate: 0-6.7% (lowest of all surgical techniques)[5]
Preferred for tumors on head, neck, or areas where tissue conservation is important
Mohs Surgery Advantages:
Highest cure rate
Tissue-sparing (important for cosmetic and functional outcomes)
Same-day margin assessment
Lower recurrence rates
Preferred by many experts for DFSP
Surgical Considerations:
Tumor location affects surgical approach
Reconstructive surgery often necessary
Multidisciplinary team may be involved
Functional preservation important (especially for extremities)
Radiation Therapy:
Radiation may be used in specific situations:
Adjuvant radiation (after surgery):
For tumors with positive or close margins when re-excision is not feasible
May reduce recurrence risk
Typical dose: 50-60 Gy over 5-6 weeks
Primary radiation (instead of surgery):
For inoperable tumors
When surgery would cause unacceptable functional or cosmetic outcomes
Less effective than surgery as sole treatment
Recurrence rates higher than with surgery
Palliative radiation:
For metastatic disease
Symptom control
Pain management
Medical Therapy:
Imatinib (Gleevec) 💊
A targeted therapy that has revolutionized treatment of advanced DFSP:
Mechanism: Inhibits PDGFB receptor activated by the fusion gene Indications:
Unresectable tumors
Metastatic disease
Recurrent disease not amenable to surgery
Neoadjuvant use (before surgery to shrink tumor)
Efficacy:
Response rates: 40-50% in advanced disease
May convert inoperable tumors to operable
Allows less extensive surgery in some cases
Generally well-tolerated
Dosing: Typically 400-800 mg daily
Duration: Continued until disease progression or unacceptable toxicity
Side effects:
Fluid retention and edema
Nausea and diarrhea
Muscle cramps
Fatigue
Generally manageable
Neoadjuvant Imatinib:
Given before surgery
May shrink large tumors
Allows more conservative surgery
Particularly useful for tumors in challenging locations
Typical duration: 2-6 months before surgery
Other Systemic Therapies:
For imatinib-resistant disease:
Other tyrosine kinase inhibitors
Chemotherapy (limited effectiveness)
Clinical trials of novel agents
Follow-Up and Surveillance
After Dermatofibroma Removal:
No specific follow-up needed
Routine skin examinations as appropriate
Monitor excision site for normal healing
After DFSP Treatment:
Intensive surveillance is essential due to recurrence risk:
Follow-up schedule:
Years 1-3: Every 3-6 months
Years 4-5: Every 6 months
After 5 years: Annually
Each visit should include:
Physical examination of surgical site
Palpation for local recurrence
Regional lymph node examination
Assessment for symptoms
Imaging surveillance:
MRI of surgical site at 6-12 months post-surgery
Additional imaging if recurrence suspected
Chest imaging annually for high-risk cases (fibrosarcomatous variant, recurrent disease)
Patient education:
Self-examination techniques
Warning signs of recurrence
Importance of long-term follow-up
Sun protection and general skin care
For comprehensive skin lesion evaluation and treatment, The Minor Surgery Center offers specialized services with experienced dermatological surgeons.
When to See a Doctor
Knowing when to seek professional evaluation is crucial for both conditions. While dermatofibromas are harmless, DFSP requires early detection and treatment for optimal outcomes.
Warning Signs Requiring Immediate Evaluation ⚠️
Seek prompt medical attention if you notice:
Changes in Existing Lesions:
Rapid growth over weeks to months
Change in color (especially darkening or multiple colors)
Change in shape or borders (becoming irregular)
Bleeding without trauma
Ulceration or crusting
Pain or tenderness that develops suddenly
Increase in size beyond 1 cm
New Lesions:
Any new firm nodule that continues to grow
Lesions that feel fixed or attached to underlying tissue
Painless lumps that progressively enlarge
Skin changes over the lesion (thinning, shininess, color change)
Red Flags for DFSP: 🚩 Progressive enlargement over months 🚩 Firm plaque or nodule on trunk or proximal extremities 🚩 Lesion larger than 2 cm 🚩 Reddish-brown or violaceous color 🚩 History of slow growth over years 🚩 Lesion that doesn't fit typical dermatofibroma pattern
Risk Assessment
Low-risk scenarios (likely dermatofibroma):
Small (under 1 cm), stable nodule
Located on lower leg
Positive dimple sign
No change over months to years
Typical appearance
High-risk scenarios (concerning for DFSP or other malignancy):
Progressive growth
Large size (over 2 cm)
Location on trunk
Atypical appearance
Negative dimple sign
Age over 40 with new lesion
Questions to Ask Your Doctor
When consulting a healthcare provider about a skin lesion, consider asking:
Diagnostic Questions:
What do you think this lesion is?
How certain are you of the diagnosis?
Do I need a biopsy?
What type of biopsy would be most appropriate?
How long will it take to get biopsy results?
Treatment Questions:
What are my treatment options?
What happens if I don't treat it?
What are the risks and benefits of each treatment?
What will the scar look like?
What is the likelihood of recurrence?
Follow-up Questions:
How often should I be monitored?
What changes should I watch for?
When should I schedule a follow-up appointment?
What are signs of complications?
Choosing the Right Healthcare Provider
Different specialists may be involved in diagnosis and treatment:
For more information about various skin conditions and their management, explore our comprehensive blog resources covering a wide range of dermatological topics.
Living with These Conditions
Understanding how to live with either condition can reduce anxiety and improve quality of life.
Living with Dermatofibroma
Psychological Impact:
While dermatofibromas are medically harmless, they can affect quality of life:
Common concerns:
Cosmetic appearance, especially on visible areas
Self-consciousness about lumps or bumps
Anxiety about cancer despite reassurance
Frustration with persistent lesions
Coping strategies:
Education about benign nature
Realistic expectations about treatment outcomes
Cosmetic camouflage if desired
Support groups or counseling if anxiety persists
Focus on overall health rather than individual lesions
Practical Management:
For symptomatic dermatofibromas:
Avoid trauma or irritation to the area
Choose clothing that doesn't rub the lesion
Use moisturizer if skin is dry or itchy
Apply ice if tender after injury
Consider padding if pressure causes discomfort
For cosmetic concerns:
Makeup can camouflage discoloration
Clothing choices can minimize visibility
Hair removal techniques should be gentle around lesions
Discuss removal options with dermatologist if bothersome
When multiple dermatofibromas are present:
Document all lesions with body map
Monitor for changes in any lesion
Discuss pattern with dermatologist
Consider underlying conditions if numerous (rare)
Living with DFSP
Emotional and Psychological Support:
A cancer diagnosis, even of a low-grade malignancy, can be emotionally challenging:
Common emotional responses:
Anxiety about cancer and recurrence
Fear of disfigurement from surgery
Stress about treatment and recovery
Uncertainty about prognosis
Concern about impact on family
Support resources:
Cancer support groups
Individual counseling or therapy
Patient advocacy organizations
Online communities for sarcoma patients
Family and friends support network
Managing Treatment Side Effects:
After surgery:
Pain management as prescribed
Wound care and monitoring for infection
Physical therapy if function is affected
Scar management strategies
Compression garments if recommended
During imatinib therapy:
Stay hydrated to reduce fluid retention
Eat small, frequent meals if nauseous
Report side effects to oncologist
Don't discontinue medication without medical guidance
Monitor for signs of complications
Reconstruction and Recovery:
Surgical reconstruction:
May involve skin grafts or flaps
Multiple procedures sometimes necessary
Healing takes time (weeks to months)
Final cosmetic result may take a year
Physical therapy may be needed
Scar management:
Silicone sheets or gels
Massage techniques
Sun protection of scars
Makeup camouflage
Acceptance and adaptation
Quality of Life Considerations:
Physical function:
Most patients return to normal activities
Some may have limitations depending on tumor location
Rehabilitation helps optimize function
Adaptive equipment if needed
Gradual return to exercise and activities
Body image:
Scars may be extensive, especially after wide excision
Counseling can help with adjustment
Support groups connect with others who understand
Focus on survival and health rather than appearance
Reconstructive options may improve cosmesis
Long-term Surveillance:
Adhering to follow-up:
Schedule appointments in advance
Keep a health diary
Report new symptoms promptly
Bring questions to appointments
Maintain open communication with healthcare team
Managing scanxiety (anxiety before scans):
Relaxation techniques
Distraction strategies
Support from loved ones
Professional counseling if severe
Mindfulness and meditation
Family and Social Considerations
Communicating with family:
Share diagnosis and treatment plan
Explain what support you need
Involve family in decision-making as appropriate
Address children's concerns age-appropriately
Maintain open dialogue
Work and daily life:
Discuss time off needs with employer
Understand disability benefits if applicable
Plan for recovery period
Communicate limitations to colleagues
Maintain normalcy when possible
Financial considerations:
Understand insurance coverage
Explore financial assistance programs
Plan for out-of-pocket costs
Consider travel expenses for specialized care
Investigate disability benefits if unable to work
Frequently Asked Questions
Can a dermatofibroma turn into dermatofibrosarcoma protuberans?
No. Dermatofibromas are benign lesions that do not transform into DFSP or any other cancer. These are two completely separate conditions with different cellular origins. A dermatofibroma will remain a dermatofibroma throughout its existence. However, if a lesion initially diagnosed as a dermatofibroma begins to grow or change significantly, it should be re-evaluated, as the initial diagnosis may have been incorrect.
How can I tell if my skin bump is serious?
Warning signs that warrant medical evaluation include:
Progressive growth over weeks to months
Size larger than 1 cm (about the size of a pencil eraser)
Irregular borders or multiple colors
Bleeding, ulceration, or crusting
Pain or tenderness
Firmness or attachment to underlying tissue
Any lesion that looks or feels different from your other moles or spots
When in doubt, have it checked out. Early evaluation of concerning lesions leads to better outcomes.
Is DFSP hereditary?
DFSP is not typically hereditary. Most cases occur sporadically without family history. The chromosomal translocation that causes DFSP (creating the COL1A1-PDGFB fusion gene) is acquired, not inherited. However, extremely rare familial cases have been reported. Having a family member with DFSP does not significantly increase your risk, unlike some other cancers.
What is the survival rate for DFSP?
The prognosis for DFSP is excellent when treated appropriately:
Overall survival: Greater than 99% with adequate surgical treatment
Local recurrence: 10-20% with wide excision, less than 7% with Mohs surgery
Metastasis: Rare, occurring in less than 5% of cases
Disease-specific mortality: Less than 1%
The key to excellent outcomes is complete surgical excision with adequate margins. Even recurrent disease can usually be successfully treated with re-excision or imatinib therapy.
Should I remove my dermatofibroma?
Removal of a dermatofibroma is a personal choice based on:
Reasons to consider removal:
Cosmetic concerns
Symptomatic (painful, itchy, tender)
Frequent irritation from clothing or activities
Persistent anxiety despite reassurance
Diagnostic uncertainty
Reasons to leave it alone:
Completely benign with no health risk
Removal leaves a scar that may be more noticeable than the lesion
Small, stable, asymptomatic lesions often best left alone
No medical necessity for removal
Discuss your specific situation with a dermatologist to make an informed decision.
How quickly does DFSP grow?
DFSP is characterized by slow growth over months to years. Typical growth patterns include:
May be present for years before diagnosis
Average growth rate: 1-2 cm per year (highly variable)
Some tumors remain stable for long periods then accelerate
Fibrosarcomatous variants may grow more rapidly
Growth is usually continuous but slow
This slow growth often leads to delayed diagnosis, as patients may dismiss the lesion as a harmless bump. Any skin lesion that continues to grow, even slowly, should be evaluated.
Can DFSP spread to other parts of the body?
DFSP has low metastatic potential but can spread in rare cases:
Local invasion: Common, extending into surrounding tissue
Distant metastasis: Rare, occurring in less than 5% of cases
Most common sites: Lungs, followed by bone and lymph nodes
Risk factors for metastasis: Fibrosarcomatous transformation, multiple recurrences, large tumor size
The vast majority of DFSP cases remain localized, and the main concern is local recurrence rather than distant spread.
What's the difference between DFSP and other sarcomas?
DFSP is a specific type of soft tissue sarcoma with unique characteristics:
Compared to other sarcomas:
Lower grade: DFSP is typically low-grade (slow-growing, less aggressive)
Better prognosis: Higher survival rates than most sarcomas
Lower metastatic rate: Less likely to spread than other sarcomas
Specific genetics: COL1A1-PDGFB fusion gene is characteristic
Skin-based: Arises in dermis, unlike many sarcomas that originate deeper
DFSP is considered one of the more "favorable" sarcomas in terms of prognosis and treatment options.
Conclusion
Understanding the distinction between dermatofibroma vs dermatofibrosarcoma protuberans is crucial for appropriate management and peace of mind. While these conditions may appear similar at first glance, they represent fundamentally different diagnoses with vastly different implications.
Dermatofibromas are common, benign skin nodules that pose no health risk and require treatment only if they cause symptoms or cosmetic concerns. Most people can safely live with these harmless bumps indefinitely. The key is accurate diagnosis and appropriate reassurance.
Dermatofibrosarcoma protuberans (DFSP), in contrast, is a rare skin cancer that requires aggressive surgical treatment to prevent local recurrence. While it has low metastatic potential and excellent survival rates with proper treatment, early detection and complete excision are essential for optimal outcomes.
Key Points to Remember
✅ Dermatofibromas are benign, common, and require no treatment unless symptomatic ✅ DFSP is a rare skin cancer requiring surgical excision with wide margins ✅ Clinical examination provides clues, but biopsy is necessary for definitive diagnosis ✅ Progressive growth is the most important warning sign requiring evaluation ✅ Early detection of DFSP significantly improves treatment outcomes ✅ Mohs surgery offers the highest cure rates and lowest recurrence for DFSP ✅ Long-term surveillance is essential after DFSP treatment ✅ Prognosis for DFSP is excellent with appropriate treatment
Take Action Today
If you have a stable, small skin bump:
Monitor for any changes in size, color, or symptoms
Photograph it to track changes over time
Schedule routine skin examinations with a dermatologist
Don't panic—most skin lesions are benign
If you notice a growing skin lesion:
Schedule an appointment with a dermatologist promptly
Don't delay evaluation of progressively enlarging lesions
Request a biopsy if there's any diagnostic uncertainty
Seek a second opinion if you're unsure about the diagnosis
If you've been diagnosed with DFSP:
Consult with a specialist experienced in treating this condition
Understand all your treatment options, including Mohs surgery
Commit to long-term surveillance and follow-up
Connect with support resources and patient communities
Maintain a positive outlook—outcomes are generally excellent
If you've had treatment for DFSP:
Adhere to your surveillance schedule religiously
Perform regular self-examinations of the surgical site
Report any new lumps or concerns immediately
Maintain healthy lifestyle habits
Stay informed about advances in treatment
Your Skin Health Partner
At The Minor Surgery Center, we understand the anxiety that comes with discovering a new or changing skin lesion. Our experienced team of dermatological specialists provides comprehensive evaluation, accurate diagnosis, and expert treatment for all types of skin conditions, from benign dermatofibromas to skin cancers like DFSP.
Whether you need a simple skin examination, a biopsy for diagnosis, or specialized surgical treatment, we offer state-of-the-art care in a comfortable, patient-centered environment. Don't let uncertainty about a skin lesion keep you awake at night—schedule a consultation today and get the answers and care you deserve.
Remember: Your skin is your body's largest organ and deserves expert attention. When it comes to the difference between dermatofibroma vs dermatofibrosarcoma protuberans, professional evaluation is the only way to know for certain. Early diagnosis, appropriate treatment, and regular monitoring are your best strategies for optimal skin health and peace of mind in 2026 and beyond.
Take charge of your skin health today. Your future self will thank you.
References
[1] Kreicher KL, et al. "Incidence and Survival of Primary Dermatofibrosarcoma Protuberans in the United States." Dermatologic Surgery. 2016;42 Suppl 1:S24-31.
[2] Simon MP, et al. "Deregulation of the platelet-derived growth factor B-chain gene via fusion with collagen gene COL1A1 in dermatofibrosarcoma protuberans and giant-cell fibroblastoma." Nature Genetics. 1997;15(1):95-98.
[3] Bowne WB, et al. "Dermatofibrosarcoma protuberans: A clinicopathologic analysis of patients treated and followed at a single institution." Cancer. 2000;88(12):2711-2720.
[4] Gloster HM Jr. "Dermatofibrosarcoma protuberans." Journal of the American Academy of Dermatology. 1996;35(3 Pt 1):355-374.
[5] Snow SN, et al. "Dermatofibrosarcoma protuberans: a report on 29 patients treated by Mohs micrographic surgery with long-term follow-up and review of the literature." Cancer. 2004;101(1):28-38.