Unraveling Lymphoma: A Comprehensive Guide to Its Types and What You Need to Know in 2025
Unraveling Lymphoma: A Comprehensive Guide to Its Types and What You Need to Know in 2025
The human body is an amazing network of systems, all working together to keep us healthy and strong. Among these is the lymphatic system, a vital part of our immune defense, tirelessly fighting off infections and diseases. But what happens when cells within this crucial system go awry? This is where lymphoma enters the picture—a type of cancer that originates in the lymphocytes, a type of white blood cell. Hearing the word "cancer" can be daunting, but understanding what lymphoma is, its different types, and how it's approached in 2025 is a powerful first step toward knowledge and empowerment.
Lymphoma isn't a single disease; it's a complex group of cancers, each with its own unique characteristics, behaviors, and treatment paths. From the less common Hodgkin lymphoma to the diverse landscape of Non-Hodgkin lymphoma, knowing the specifics can help patients and their loved ones navigate the journey ahead. This comprehensive guide aims to demystify lymphoma, breaking down its various forms into understandable terms, exploring symptoms, diagnosis, and the latest treatment insights available today.
Key Takeaways
Lymphoma is a Cancer of the Lymphatic System: It starts in lymphocytes, which are white blood cells crucial for fighting infection, and affects parts of the immune system like lymph nodes, spleen, and bone marrow.
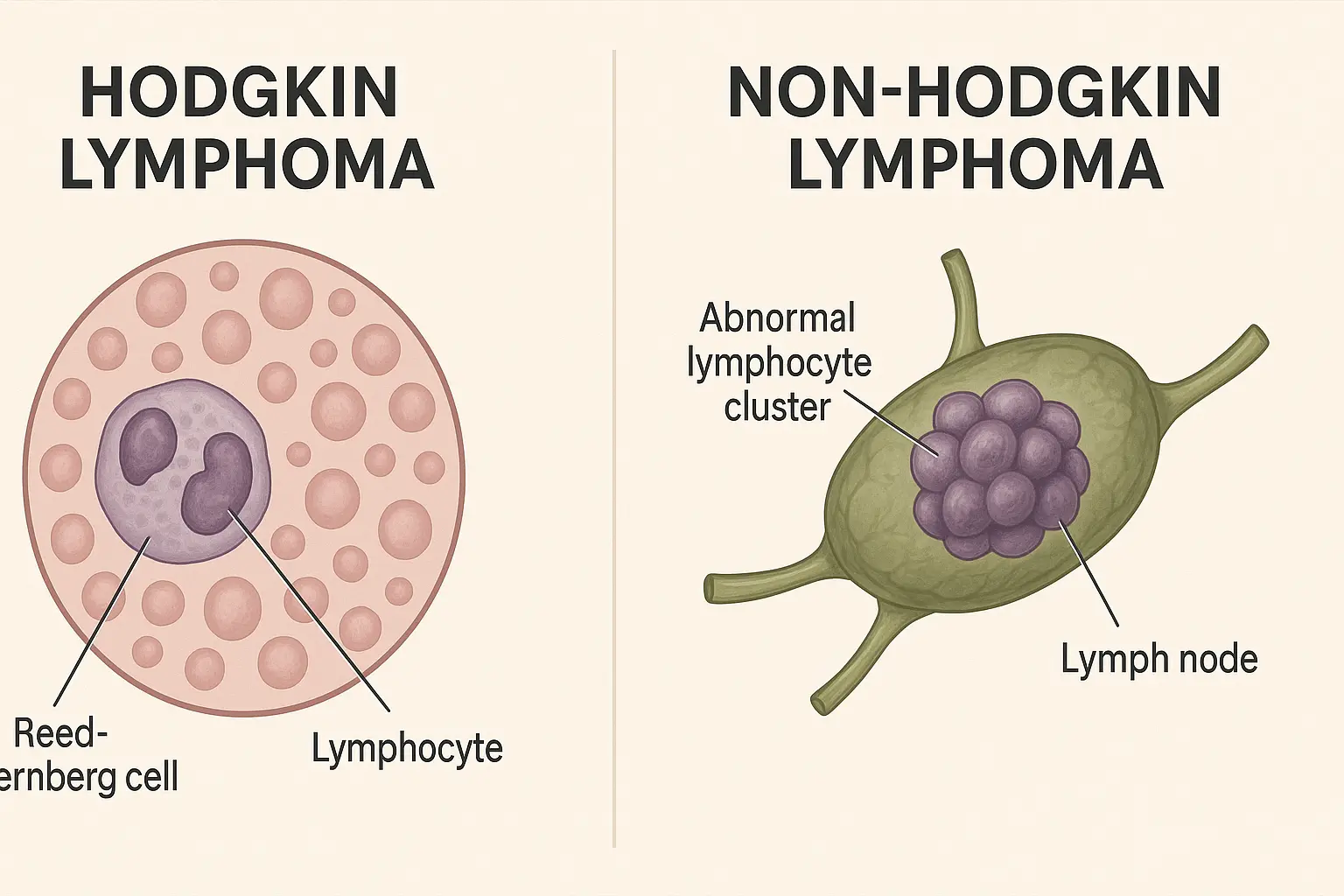
Two Main Categories Exist: Lymphoma is broadly divided into Hodgkin Lymphoma (HL), characterized by the presence of Reed-Sternberg cells, and Non-Hodgkin Lymphoma (NHL), which encompasses a much wider range of subtypes.
Diverse Types Within Each Category: NHL alone has over 70 different subtypes, each behaving differently, ranging from slow-growing (indolent) to fast-growing (aggressive) forms, requiring specific diagnostic and treatment approaches.
Symptoms Vary but Key Signs Include: Swollen, painless lymph nodes, fever, night sweats, unexplained weight loss (known as "B symptoms"), fatigue, and itching are common indicators that warrant medical attention.
Diagnosis and Treatment are Personalized: Identifying the exact type of lymphoma through biopsy is critical, as treatment plans in 2025 are highly tailored, often involving chemotherapy, radiation, immunotherapy, or targeted therapies, guided by the specific subtype, stage, and patient health.
What is Lymphoma? Understanding the Basics
Imagine your body's defense system as a highly organized army. Lymphoma is a cancer that starts in the soldiers of this army—the lymphocytes. These are specialized white blood cells that play a critical role in your immune system, helping to fight off infections and diseases. When these lymphocytes grow out of control, they can form tumors in various parts of the body, most commonly in the lymph nodes.
The lymphatic system is like a network of roads and bases for these immune cells. It includes:
Lymph nodes: Small, bean-shaped glands found throughout your body (neck, armpits, groin) that filter lymph fluid and store lymphocytes.
Spleen: An organ that filters blood, stores white blood cells, and removes old red blood cells.
Thymus: A gland located behind your breastbone that helps mature a specific type of lymphocyte called T-cells.
Bone marrow: The spongy tissue inside your bones where all blood cells, including lymphocytes, are made.
Lymphatic vessels: A network of tiny tubes that carry lymph fluid (a clear fluid containing lymphocytes) throughout the body.
When lymphoma develops, these abnormal lymphocytes can accumulate in any of these areas, leading to swelling and disrupting the normal function of the immune system. The exact cause of lymphoma isn't always clear, but it involves changes (mutations) in the DNA of a lymphocyte, leading it to grow and divide uncontrollably instead of dying off as it should.
🗣️ "Lymphoma is a journey, not a destination. Understanding your specific type is the first step towards charting the best path forward."
Understanding the Lymphatic System: Your Body's Silent Protector
Before diving deeper into the types of lymphoma, it's helpful to have a clearer picture of the lymphatic system itself. This system is often overlooked but is absolutely essential for your health. It's a complex network that works alongside your circulatory system, but instead of carrying blood, it carries a fluid called lymph.
Here’s a closer look at its key components and functions:
Components of the Lymphatic System
Lymph: This clear, watery fluid circulates throughout your body, bathing tissues and carrying waste products, dead cells, and foreign invaders (like bacteria and viruses) away from your tissues. It also transports white blood cells, especially lymphocytes.
Lymphatic Vessels: These are like highways and byways for lymph. They are thin tubes that collect lymph from tissues and transport it back towards the heart, eventually draining into the bloodstream. Unlike blood, lymph is not pumped by the heart; instead, it moves through muscle contractions and one-way valves.
Lymph Nodes: These small, bean-shaped organs are strategically placed along the lymphatic vessels, acting as filtering stations. They contain immune cells, including lymphocytes, that trap and destroy harmful substances like bacteria, viruses, and cancer cells. When you have an infection, your lymph nodes might swell, which is a sign that your immune system is working hard. Common areas for lymph nodes include the neck, armpits, groin, chest, and abdomen.
Spleen: Located on the left side of your abdomen, the spleen is a large lymphatic organ with several critical roles. It filters blood, removes old or damaged red blood cells, stores platelets and white blood cells, and helps produce lymphocytes.
Thymus: Situated behind your breastbone, the thymus is crucial for the development and maturation of T-lymphocytes (T-cells) during childhood and adolescence. While it shrinks after puberty, it still plays a role in immune function.
Bone Marrow: This soft, spongy tissue inside your bones is the birthplace of all blood cells, including red blood cells, white blood cells (like lymphocytes), and platelets.
Tonsils and Adenoids: These are collections of lymphatic tissue located in the throat and nasal cavity. They act as a first line of defense against pathogens entering through the mouth or nose.
Peyer’s Patches: These are small masses of lymphatic tissue found in the lining of the small intestine. They monitor bacteria in the gut and prevent the growth of harmful bacteria.
Functions of the Lymphatic System
The lymphatic system performs several vital functions:
Fluid Balance: It collects excess fluid, proteins, and waste products from tissues and returns them to the bloodstream, preventing swelling (edema).
Immune Defense: It's a cornerstone of your immune system. Lymphocytes patrol the body, identify foreign invaders (pathogens) and abnormal cells (like cancer cells), and launch an immune response to neutralize them.
Fat Absorption: It absorbs fats and fat-soluble vitamins from the digestive system and transports them to the bloodstream.
When lymphoma develops, it disrupts these crucial functions, leading to a range of symptoms and compromising the body's ability to fight off disease. Understanding these basics helps to appreciate why an accurate diagnosis and targeted treatment are so important.
For more information on general health and conditions, you can explore resources like The Minor Surgery Center, which often provides insights into various medical topics.
How Lymphoma Develops: A Closer Look at Cellular Changes
Lymphoma begins when a healthy lymphocyte undergoes a malignant transformation. To understand this, let's briefly review how normal cells work. Our bodies are made of trillions of cells, each with specific jobs. These cells grow, divide, and die in a controlled manner, following instructions encoded in their DNA.
In lymphoma, something goes wrong with the DNA of a lymphocyte. This genetic error, or mutation, can cause the lymphocyte to:
Grow and divide uncontrollably: Instead of stopping when it should, the cell keeps multiplying.
Not die when it should: Normal cells have a built-in process for self-destruction when they are old or damaged (apoptosis). Cancerous cells bypass this process.
Accumulate: These abnormal cells build up, often forming tumors, particularly in lymph nodes, but they can also affect other organs like the spleen, bone marrow, or even the brain.
These cancerous lymphocytes are no longer effective at fighting infections. In fact, they can crowd out healthy cells and weaken the immune system.
What Causes These Mutations?
The exact reasons why these mutations occur are often unknown. However, researchers have identified several factors that can increase the risk of developing lymphoma, which we will discuss later. These include:
Exposure to certain viruses (e.g., Epstein-Barr virus, HIV)
Weakened immune system
Exposure to certain chemicals or radiation
Genetic predispositions
It's important to remember that having a risk factor doesn't mean you will definitely get lymphoma, and many people with lymphoma have no known risk factors. The development of lymphoma is a complex process involving multiple steps and interactions.
The Two Main Categories: Hodgkin Lymphoma vs. Non-Hodgkin Lymphoma
When a doctor diagnoses lymphoma, the very first step is to determine whether it's Hodgkin Lymphoma (HL) or Non-Hodgkin Lymphoma (NHL). This distinction is crucial because these two broad categories behave differently, look different under a microscope, and require distinct treatment approaches.
The primary way to tell them apart is by examining a biopsy sample of the cancerous tissue under a microscope.
Hodgkin Lymphoma (HL)
Defining Feature: The hallmark of Hodgkin lymphoma is the presence of a specific type of abnormal cell called the Reed-Sternberg cell. These are large, distinctive cells with multiple nuclei or a bilobed nucleus, often described as looking like "owl's eyes" 👀.
Prevalence: HL is less common than NHL, accounting for about 10-15% of all lymphomas.
Age Groups: It has a bimodal age distribution, meaning it's most common in two age groups: young adults (especially those in their 20s and 30s) and older adults (over 55).
Spread Pattern: HL typically spreads in an orderly fashion from one group of lymph nodes to adjacent groups. This predictable spread often makes it easier to treat, especially when caught early.
Prognosis: HL is generally considered one of the most curable cancers, with high survival rates, particularly in earlier stages.
Non-Hodgkin Lymphoma (NHL)
Defining Feature: NHL is characterized by the absence of Reed-Sternberg cells. Instead, it encompasses a vast and diverse group of lymphomas that originate from either B-lymphocytes (B-cells) or T-lymphocytes (T-cells).
Prevalence: NHL is far more common, making up about 85-90% of all lymphoma cases.
Age Groups: It can occur at any age but is more common in older adults, with the risk increasing with age.
Spread Pattern: NHL is much more varied in its spread. It can arise in lymph nodes or in organs outside the lymphatic system (extranodal sites) and can spread in an unpredictable manner.
Complexity: There are over 70 different subtypes of NHL, making it a very complex group of diseases. These subtypes vary greatly in their aggressiveness, from slow-growing (indolent) types that may not require immediate treatment to very fast-growing (aggressive) types that need urgent, intensive therapy.
Prognosis: The prognosis for NHL varies widely depending on the specific subtype, stage, and other individual factors. Some types are highly curable, while others are more challenging to treat.
The distinction between HL and NHL is the first, most crucial step in diagnosis because it completely dictates the subsequent diagnostic workup and the entire treatment strategy. Let's delve deeper into each of these main categories.
Hodgkin Lymphoma (HL)
Hodgkin Lymphoma, while less common, is a significant form of cancer that has seen remarkable advances in treatment, leading to high cure rates. Its unique characteristics set it apart from its Non-Hodgkin counterpart.
Characteristics of Hodgkin Lymphoma
The defining feature of Hodgkin Lymphoma, as mentioned, is the presence of Reed-Sternberg cells. These are large, abnormal B-lymphocytes that are typically multinucleated (have more than one nucleus) or have a bilobed nucleus, giving them a distinctive "owl's eyes" appearance under a microscope. While these cells are the hallmark, they often make up only a small percentage of the cells in the affected lymph node; the majority are normal immune cells recruited by the Reed-Sternberg cells.
HL typically originates in a single lymph node region and then spreads in an organized, predictable manner to nearby lymph nodes. This characteristic pattern of spread often makes it easier to stage and treat effectively.
Subtypes of Hodgkin Lymphoma
Hodgkin Lymphoma is further divided into two main categories, each with its own subtypes:
1. Classical Hodgkin Lymphoma (CHL)
This is the most common type, accounting for about 95% of all HL cases. It is characterized by the presence of Reed-Sternberg cells in a specific immune cell environment. CHL has four main subtypes:
Nodular Sclerosis Hodgkin Lymphoma (NSHL):
Prevalence: This is the most common subtype of CHL, making up 70-80% of cases.
Characteristics: It's characterized by fibrous bands (sclerosis) that divide the lymph node tissue into nodules, and distinctive Reed-Sternberg cells (often called lacunar cells due to their appearance).
Affected Groups: Most common in adolescents and young adults, and slightly more prevalent in women.
Prognosis: Generally has an excellent prognosis.
Mixed Cellularity Hodgkin Lymphoma (MCHL):
Prevalence: Accounts for 15-30% of CHL cases.
Characteristics: Contains many Reed-Sternberg cells mixed with various other immune cells (lymphocytes, eosinophils, plasma cells). There's no nodular pattern or sclerosis.
Affected Groups: More common in older adults and in men. Also seen in people with HIV infection.
Prognosis: Good prognosis, though sometimes slightly less favorable than NSHL.
Prevalence: Accounts for about 5% of all HL cases.
Characteristics: Distinct from classical HL, NLPHL is characterized by the presence of "popcorn cells" (LP cells, or lymphocyte-predominant cells), which are variants of Reed-Sternberg cells that look different and express different proteins. It lacks the typical Reed-Sternberg cells of CHL.
Affected Groups: More common in men, usually in their 30s to 50s.
Behavior: NLPHL often behaves more like an indolent (slow-growing) Non-Hodgkin Lymphoma. It typically grows slowly and may recur over time, but it generally has an excellent long-term prognosis. In rare cases, it can transform into an aggressive B-cell NHL.
Treatment: Due to its distinct biology, NLPHL is often treated differently from classical HL, sometimes with less intensive regimens or targeted therapies.
Symptoms of Hodgkin Lymphoma
The symptoms of HL can be varied and often mimic those of less serious conditions. However, persistent or worsening symptoms should always prompt a visit to a doctor. Common symptoms include:
Painless Swelling of Lymph Nodes: This is the most common symptom, often in the neck, armpit, or groin. The swollen nodes are typically firm and rubbery.
B Symptoms: These are a group of systemic symptoms that are important for staging and prognosis:
Unexplained Fever: Fevers that come and go, often in the evening, without an infection.
Drenching Night Sweats: Sweating so profusely at night that clothes and bedding become soaked.
Unexplained Weight Loss: Losing 10% or more of body weight in 6 months without trying.
Fatigue: Persistent and overwhelming tiredness not relieved by rest.
Itching (Pruritus): Severe, generalized itching without a rash.
Alcohol-Induced Pain: Pain in the lymph nodes after drinking alcohol (rare but specific to HL).
Coughing or Shortness of Breath: If lymph nodes in the chest are enlarged, they can press on airways.
Abdominal Pain or Swelling: If the spleen or lymph nodes in the abdomen are affected.
Diagnosis of Hodgkin Lymphoma
Diagnosing HL involves a thorough medical history, physical exam, and several diagnostic tests:
Biopsy: This is the most crucial step. A piece of the enlarged lymph node (excisional biopsy) or other suspicious tissue is removed and examined under a microscope by a pathologist to identify Reed-Sternberg cells and determine the subtype.
Imaging Tests:
CT Scan (Computed Tomography): Used to check for enlarged lymph nodes or tumors in the chest, abdomen, and pelvis.
PET Scan (Positron Emission Tomography): Often combined with a CT scan (PET-CT). This scan uses a radioactive sugar to highlight areas of active cancer cells throughout the body, helping to determine the extent of the disease and monitor treatment response.
MRI (Magnetic Resonance Imaging): Less commonly used for initial staging but may be used if there are concerns about spread to the brain or spinal cord.
Blood Tests: To check blood cell counts, kidney and liver function, and general health.
Bone Marrow Biopsy and Aspiration: While less commonly positive in early-stage HL, it's often done to check for lymphoma cells in the bone marrow, particularly in more advanced stages or certain subtypes.
Lymph Node Mapping (Sentinel Lymph Node Biopsy): Not typically used for Hodgkin lymphoma.
Accurate diagnosis and staging are vital for developing the most effective treatment plan. For concerns about diagnostic procedures or general health inquiries, visiting a reputable clinic can provide valuable guidance and support.
Treatment Approaches for Hodgkin Lymphoma
Treatment for Hodgkin Lymphoma has advanced significantly, leading to high cure rates for most patients. The specific treatment plan depends on the subtype of HL, its stage, the patient's age and overall health, and the presence of "B symptoms."
Common treatment modalities include:
Chemotherapy: This is the cornerstone of HL treatment. It uses powerful drugs to kill cancer cells throughout the body. Common chemotherapy regimens for HL include:
ABVD: A combination of Doxorubicin (Adriamycin), Bleomycin, Vinblastine, and Dacarbazine. This is the most widely used regimen for classical HL.
BEACOPP: A more intensive regimen (Bleomycin, Etoposide, Doxorubicin (Adriamycin), Cyclophosphamide, Vincristine (Oncovin), Procarbazine, and Prednisone) often used for advanced-stage or high-risk HL.
Chemotherapy is usually given in cycles, with periods of treatment followed by periods of rest.
Radiation Therapy: This uses high-energy rays to kill cancer cells in a specific area. It's often used after chemotherapy, particularly for patients with bulky disease (large tumors) or in early stages to target affected lymph node regions. Advances in radiation techniques (e.g., intensity-modulated radiation therapy, IMRT) help to minimize damage to healthy tissues.
Immunotherapy: These treatments harness the body's own immune system to fight cancer.
Checkpoint Inhibitors: Drugs like nivolumab and pembrolizumab block certain proteins (PD-1) on immune cells, essentially taking the brakes off the immune system so it can recognize and attack cancer cells. These are often used for HL that has relapsed (returned) or is refractory (doesn't respond to initial treatment).
Brentuximab Vedotin (Adcetris): This is an antibody-drug conjugate (ADC). It's an antibody that targets a protein called CD30 (found on Reed-Sternberg cells) linked to a chemotherapy drug. The antibody delivers the chemotherapy directly to the cancer cells, minimizing side effects on healthy cells. It's used for relapsed/refractory HL and in some first-line treatments for high-risk patients.
Stem Cell Transplant: For patients whose HL has relapsed or is refractory after initial treatments, a high-dose chemotherapy regimen followed by an autologous stem cell transplant (using the patient's own stem cells) may be an option. Allogeneic stem cell transplant (using donor stem cells) is less common but can be considered in certain situations.
Targeted Therapy: While less prominent than in NHL, some targeted therapies are being explored or used in specific situations for HL, especially those that target specific pathways or proteins found in Reed-Sternberg cells.
Follow-up Care and Survivorship
After treatment, regular follow-up appointments are essential to monitor for recurrence and manage any long-term side effects. Hodgkin lymphoma survivors may face unique challenges, and support groups, mental health resources, and a focus on overall wellness are crucial. Many resources are available to help patients navigate life after lymphoma, including those focused on patient FAQs and general health information.
The prognosis for Hodgkin Lymphoma is generally excellent, especially with modern treatment protocols. Many patients achieve long-term remission or are cured.
Non-Hodgkin Lymphoma (NHL)
Non-Hodgkin Lymphoma is a much more diverse and complex group of cancers compared to Hodgkin Lymphoma. It encompasses a wide spectrum of lymphomas, each originating from different types of lymphocytes and behaving in unique ways. This diversity means that diagnosis and treatment plans for NHL are highly individualized.
Characteristics of Non-Hodgkin Lymphoma
Absence of Reed-Sternberg Cells: This is the defining characteristic that separates NHL from HL.
Origin: NHL can originate from either B-lymphocytes (B-cells) or T-lymphocytes (T-cells), which are the two main types of lymphocytes.
B-cell lymphomas: Account for about 85% of all NHL cases.
T-cell lymphomas: Account for about 15% of all NHL cases.
Diversity: There are over 70 different recognized subtypes of NHL, making it a highly heterogeneous disease.
Spread Pattern: NHL can arise in lymph nodes or in extranodal sites (organs outside the lymphatic system), such as the stomach, skin, brain, or bone. Its spread pattern is often less predictable than HL.
Growth Rate: NHL subtypes are broadly categorized by their growth rate:
Indolent (Slow-Growing) Lymphomas: These tend to grow slowly and may not cause symptoms for a long time. They may not require immediate treatment and can be managed with "watch and wait" approaches, though they are often harder to cure. Examples include Follicular Lymphoma and Marginal Zone Lymphoma.
Aggressive (Fast-Growing) Lymphomas: These grow quickly and cause severe symptoms, requiring prompt and intensive treatment. They are often curable, especially if caught early. Examples include Diffuse Large B-Cell Lymphoma and Burkitt Lymphoma.
Prevalence and Complexity
NHL is more common than HL, with incidence rates generally increasing with age. The complexity of NHL stems from its vast number of subtypes, each with unique genetic mutations, protein expressions, and clinical behaviors. This necessitates a precise diagnosis to determine the exact subtype, as it directly impacts treatment decisions. Pathologists use a combination of microscopic examination, immunohistochemistry (staining for specific proteins), and genetic tests to accurately classify NHL.
Major Types of B-Cell Non-Hodgkin Lymphoma
As B-cell lymphomas are the most common, let's explore some of the key subtypes:
1. Diffuse Large B-Cell Lymphoma (DLBCL)
Prevalence: This is the most common aggressive NHL, accounting for about 1 in 3 cases of NHL.
Characteristics: DLBCL is characterized by large, abnormal B-cells that grow in a diffuse (spread out) pattern throughout the lymph node or affected tissue. It can arise in lymph nodes or in extranodal sites like the gastrointestinal tract, skin, bone, or even the brain.
Behavior: It is a fast-growing, aggressive lymphoma that requires prompt treatment.
Prognosis: Despite its aggressive nature, DLBCL is often curable with modern chemotherapy regimens, with approximately 60-70% of patients achieving long-term remission.
Treatment: The standard treatment is a combination chemotherapy regimen known as R-CHOP: Rituximab (an immunotherapy drug that targets CD20 on B-cells), Cyclophosphamide, Doxorubicin (hydroxydaunorubicin), Vincristine (Oncovin), and Prednisone. Other treatments may include radiation therapy, and for relapsed/refractory cases, CAR T-cell therapy or stem cell transplant.
2. Follicular Lymphoma (FL)
Prevalence: The second most common type of NHL, accounting for about 20-30% of cases.
Characteristics: FL is an indolent (slow-growing) lymphoma that originates from B-cells within the germinal centers of lymph nodes. The cancer cells tend to grow in a clustered, "follicular" pattern. It's often widespread at diagnosis, affecting multiple lymph nodes and sometimes the bone marrow.
Behavior: It's typically slow-growing and may not cause significant symptoms for years. While often not curable in advanced stages, it's highly treatable, and patients can live for many years with good quality of life. It can, however, transform into a more aggressive lymphoma like DLBCL.
Treatment:
"Watch and Wait": For asymptomatic patients with limited disease, observation may be the initial approach.
Rituximab: Often used alone or in combination with chemotherapy.
Chemotherapy: Regimens like R-CVP (Rituximab, Cyclophosphamide, Vincristine, Prednisone) or R-Bendamustine are common.
Radiation Therapy: Can be used for localized disease.
Radioimmunotherapy: Combines a radioactive substance with an antibody.
Newer Therapies: Targeted drugs (e.g., PI3K inhibitors) and immunotherapy agents are emerging.
3. Mantle Cell Lymphoma (MCL)
Prevalence: A less common type, accounting for about 5-10% of NHL cases.
Characteristics: MCL originates from B-cells in the "mantle zone" of lymph nodes. It's often characterized by a specific genetic change called the t(11;14) translocation, which leads to overexpression of the cyclin D1 protein. It often affects lymph nodes, bone marrow, spleen, and the gastrointestinal tract.
Behavior: MCL is generally considered an aggressive lymphoma, though its behavior can vary. It tends to be widespread at diagnosis and can be challenging to treat effectively, with frequent relapses.
Treatment: Often involves intensive chemotherapy regimens, sometimes followed by autologous stem cell transplant for younger, fitter patients. Targeted therapies like Bruton's tyrosine kinase (BTK) inhibitors (e.g., ibrutinib, acalabrutinib) have significantly improved outcomes for MCL patients, particularly in relapsed settings.
4. Marginal Zone Lymphoma (MZL)
Prevalence: Accounts for about 5-10% of NHL cases.
Characteristics: MZL is an indolent (slow-growing) lymphoma that arises from B-cells in the marginal zone of lymphoid tissues. It's categorized into three main subtypes:
Extranodal MZL of Mucosa-Associated Lymphoid Tissue (MALT Lymphoma): The most common type of MZL, often found in organs like the stomach (frequently linked to H. pylori infection), salivary glands, thyroid, or lungs.
Nodal MZL: Affects lymph nodes.
Splenic MZL: Primarily affects the spleen and bone marrow.
Behavior: Generally slow-growing. MALT lymphomas, especially gastric MALT, can sometimes be treated by eradicating the underlying infection (e.g., H. pylori antibiotics).
Treatment: Varies by subtype and location. Can include "watch and wait," antibiotics (for H. pylori-positive gastric MALT), radiation therapy, Rituximab, or chemotherapy.
5. Burkitt Lymphoma (BL)
Prevalence: A rare but highly aggressive type of NHL.
Characteristics: BL is characterized by very fast-growing B-cells. It is strongly associated with the Epstein-Barr virus (EBV) in endemic (African) forms and in immunocompromised individuals. It often has a specific genetic translocation, t(8;14), involving the MYC gene.
Subtypes:
Endemic (African) BL: Common in Africa, often presents as a jaw tumor in children.
Sporadic BL: Occurs worldwide, often presents as an abdominal tumor.
Immunodeficiency-associated BL: Seen in people with HIV/AIDS or organ transplant recipients.
Behavior: Extremely aggressive, requiring immediate and intensive multi-agent chemotherapy.
Prognosis: Despite its aggressiveness, BL is often curable, especially in children and young adults, with appropriate intensive treatment.
Treatment: High-dose, short-cycle chemotherapy regimens are crucial due to its rapid growth.
Characteristics: WM involves lymphocytes that have features of both B-cells and plasma cells. These cells produce a large amount of an abnormal antibody called IgM (a monoclonal gammopathy), which can thicken the blood (hyperviscosity syndrome) and cause various symptoms.
Behavior: Slow-growing.
Treatment: "Watch and wait" for asymptomatic patients. Treatment options include chemotherapy, Rituximab, and targeted therapies (e.g., BTK inhibitors).
7. Primary Mediastinal Large B-Cell Lymphoma (PMBL)
Prevalence: Accounts for about 2-4% of NHL cases.
Characteristics: A distinct type of aggressive B-cell lymphoma that originates in the mediastinum (the area behind the breastbone). It primarily affects young adults, more commonly women. It shares some molecular features with Hodgkin lymphoma.
Behavior: Aggressive, often presenting as a large mass in the chest, which can cause symptoms like shortness of breath and swelling in the face and neck.
Treatment: Intensive chemotherapy regimens (e.g., R-CHOP or dose-adjusted R-EPOCH) often combined with radiation therapy.
Major Types of T-Cell Non-Hodgkin Lymphoma
T-cell lymphomas are less common than B-cell lymphomas but are often more aggressive and challenging to treat.
1. Peripheral T-Cell Lymphoma, Not Otherwise Specified (PTCL-NOS)
Prevalence: This is the most common subtype of mature T-cell lymphoma, but it's a "catch-all" category for T-cell lymphomas that don't fit into other specific classifications.
Characteristics: Highly heterogeneous, meaning it can present in various ways and have diverse features under the microscope.
Behavior: Generally aggressive.
Treatment: Typically involves intensive chemotherapy regimens (e.g., CHOP), sometimes followed by autologous stem cell transplant. Newer agents are being explored due to often poorer outcomes compared to B-cell lymphomas.
2. Anaplastic Large Cell Lymphoma (ALCL)
Prevalence: Accounts for about 1-2% of all NHLs.
Characteristics: ALCL is characterized by large, abnormal T-cells (or sometimes NK cells). It can be further divided based on the presence of a genetic rearrangement called ALK (anaplastic lymphoma kinase).
ALK-positive ALCL: More common in children and young adults, generally has a better prognosis.
ALK-negative ALCL: More common in older adults, often more aggressive.
Behavior: Aggressive.
Treatment: Chemotherapy (e.g., CHOP), often with targeted therapy like Brentuximab Vedotin (which targets CD30, a protein often found on ALCL cells), particularly for ALK-negative or relapsed ALCL.
3. Angioimmunoblastic T-Cell Lymphoma (AITL)
Prevalence: A rare, aggressive T-cell lymphoma.
Characteristics: AITL is characterized by abnormal T-cells that are found in a background of other reactive immune cells and blood vessels. Patients often have systemic symptoms like fever, night sweats, weight loss, skin rashes, and autoimmune phenomena.
Behavior: Aggressive, often with a complex clinical course.
Treatment: Chemotherapy (e.g., CHOP), sometimes followed by stem cell transplant. Newer agents targeting specific pathways are being investigated.
4. Cutaneous T-Cell Lymphoma (CTCL)
Prevalence: A group of rare T-cell lymphomas that primarily affect the skin.
Characteristics: Unlike other lymphomas, CTCL starts in the skin and may or may not spread internally.
Subtypes:
Mycosis Fungoides (MF): The most common type of CTCL. It typically starts as patches or plaques on the skin that can be itchy and scaly, slowly progressing over years or decades. In advanced stages, it can form tumors or spread to lymph nodes and internal organs.
Sézary Syndrome (SS): A more aggressive form of CTCL characterized by widespread red, itchy skin (erythroderma), abnormal T-cells (Sézary cells) in the blood, and enlarged lymph nodes.
Behavior: MF is typically indolent, while SS is aggressive.
Treatment: Varies significantly based on the stage and subtype.
Systemic therapies: Chemotherapy, interferon, retinoids, targeted therapies, immunotherapy, histone deacetylase (HDAC) inhibitors, and sometimes stem cell transplant for advanced cases.
The sheer variety of NHL subtypes underscores the importance of a precise diagnosis. Each subtype demands a tailored approach, relying on the expertise of a multidisciplinary team of medical professionals to formulate the most effective treatment strategy.
Symptoms of Non-Hodgkin Lymphoma
Symptoms of NHL can be very general and often mimic those of other, less serious conditions. However, persistent or worsening symptoms should always be evaluated by a doctor.
General Symptoms (often shared with HL):
Painless Swelling of Lymph Nodes: Most commonly in the neck, armpit, or groin. Unlike HL, NHL can also affect lymph nodes deep inside the body (e.g., in the abdomen or chest), which may not be visible or palpable.
B Symptoms:
Unexplained Fever: Fevers that come and go.
Drenching Night Sweats: Soaking night sweats.
Unexplained Weight Loss: Loss of 10% or more of body weight in 6 months without trying.
Fatigue: Persistent and severe tiredness.
Loss of Appetite: Reduced desire to eat.
Itching (Pruritus): Generalized itching.
Specific Symptoms (depending on where the lymphoma is located):
Abdominal pain or swelling: If lymphoma affects the spleen, stomach, intestines, or abdominal lymph nodes. This can also lead to feeling full quickly or changes in bowel habits.
Chest pain, cough, or shortness of breath: If lymphoma is in the chest (e.g., in the mediastinum or lungs).
Headaches, seizures, or changes in personality: If lymphoma spreads to the brain or spinal cord (central nervous system lymphoma).
Skin rashes, lumps, or itching: For cutaneous lymphomas.
Pain, numbness, or weakness: If lymphoma presses on nerves.
Frequent infections: Due to a weakened immune system.
Diagnosis of Non-Hodgkin Lymphoma
Diagnosing NHL is a multi-step process that requires careful evaluation to identify the specific subtype.
Biopsy: This is the most critical diagnostic test. A sample of the suspected cancerous tissue (lymph node, tumor, or bone marrow) is removed and examined by a pathologist.
Excisional Biopsy: Removal of an entire lymph node is often preferred for a definitive diagnosis.
Core Needle Biopsy: Removal of a tissue sample using a hollow needle.
Bone Marrow Biopsy and Aspiration: Often performed to check for lymphoma cells in the bone marrow.
Lumbar Puncture (Spinal Tap): If there's a suspicion of central nervous system involvement, a sample of cerebrospinal fluid is taken.
Pathology Review: The pathologist not only looks for cancer cells but also performs specialized tests:
Immunohistochemistry: Stains are used to detect specific proteins on the surface of the lymphoma cells (e.g., CD20 for B-cells, CD3 for T-cells), which helps classify the lymphoma.
Flow Cytometry: Analyzes cell surface markers.
Cytogenetics and FISH (Fluorescence In Situ Hybridization): Looks for specific chromosomal abnormalities or genetic translocations (e.g., t(14;18) in follicular lymphoma, t(8;14) in Burkitt lymphoma).
Gene Expression Profiling: Can provide a deeper understanding of the molecular characteristics of the lymphoma, particularly for DLBCL.
Imaging Tests:
CT Scan: To find enlarged lymph nodes or tumors in the chest, abdomen, and pelvis.
PET Scan (PET-CT): Used to identify areas of active cancer throughout the body and help with staging.
MRI: May be used for detailed imaging of specific areas, such as the brain or spinal cord.
Blood Tests: To check blood counts, kidney and liver function, and levels of certain proteins (e.g., LDH, beta-2 microglobulin) that can be elevated in lymphoma.
Endoscopy/Colonoscopy: If gastrointestinal lymphoma is suspected.
The extensive diagnostic workup ensures that the exact subtype of NHL is identified, which is paramount for guiding treatment decisions.
Treatment Approaches for Non-Hodgkin Lymphoma
Given the vast number of NHL subtypes, treatment is highly individualized. The choice of therapy depends on:
The specific subtype of NHL (indolent vs. aggressive).
The stage of the lymphoma.
The patient's age and overall health.
Location of the lymphoma (e.g., CNS involvement).
Genetic and molecular features of the lymphoma cells.
Common treatment modalities include:
Chemotherapy: The primary treatment for aggressive NHLs. It uses drugs to kill cancer cells, often in combination.
R-CHOP: (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisone) is the standard regimen for DLBCL and some other aggressive B-cell lymphomas.
Other regimens like R-EPOCH, Hyper-CVAD, or Bendamustine-Rituximab are used for specific subtypes (e.g., Burkitt, MCL, Follicular).
Immunotherapy: These treatments boost the body's immune system or use lab-made immune system components to fight cancer.
Monoclonal Antibodies:
Rituximab: Targets the CD20 protein on B-cells, leading to their destruction. It has revolutionized the treatment of B-cell NHLs.
Obinutuzumab (Gazyva): Another anti-CD20 antibody, sometimes used for FL.
Brentuximab Vedotin (Adcetris): Targets CD30, used for some T-cell lymphomas (ALCL).
Checkpoint Inhibitors: (e.g., nivolumab, pembrolizumab) Can be used for certain relapsed/refractory NHLs.
CAR T-Cell Therapy (Chimeric Antigen Receptor T-cell Therapy): A groundbreaking treatment where a patient's own T-cells are genetically modified in a lab to recognize and attack lymphoma cells, then infused back into the patient. It's approved for certain types of relapsed/refractory aggressive B-cell NHLs (DLBCL, MCL, PMBL) and offers hope for patients who have exhausted other options.
Targeted Therapy: These drugs specifically target vulnerabilities in cancer cells, often with fewer side effects than traditional chemotherapy.
BTK Inhibitors: (e.g., ibrutinib, acalabrutinib, zanubrutinib) Used for MCL, MZL, and WM.
PI3K Inhibitors: (e.g., idelalisib, duvelisib, copanlisib) Used for FL and MZL.
BCL-2 Inhibitors: (e.g., venetoclax) Used for certain types of aggressive B-cell lymphomas.
Radiation Therapy: Uses high-energy rays to kill cancer cells in a localized area. It can be used as a primary treatment for early-stage indolent lymphomas, or to treat bulky disease, reduce pain, or treat lymphoma in specific sites (e.g., brain).
Stem Cell Transplant:
Autologous Stem Cell Transplant: Uses the patient's own stem cells. High-dose chemotherapy is given to kill cancer cells, followed by infusion of the stored stem cells to restore bone marrow function. Often used for relapsed/refractory aggressive NHLs.
Allogeneic Stem Cell Transplant: Uses donor stem cells. Less common for NHL but may be considered for certain high-risk or relapsed cases.
"Watch and Wait" (Active Surveillance): For some indolent lymphomas that are asymptomatic and slow-growing (e.g., early-stage Follicular Lymphoma, some MZLs), immediate treatment may not be necessary. Patients are closely monitored, and treatment is initiated only if symptoms develop or the disease progresses.
The field of lymphoma treatment is rapidly evolving, with new therapies and clinical trials continually emerging. Patients are encouraged to discuss all available options, including participation in clinical trials, with their healthcare team. For more information on current treatment options and patient care, exploring a dedicated blog or conditions page can be beneficial.
Staging of Lymphoma: Understanding the Extent of the Disease
Staging is a critical process that helps doctors determine the extent to which lymphoma has spread in the body. This information is vital for selecting the most appropriate treatment plan and predicting the prognosis. The most widely used system for staging both Hodgkin Lymphoma and Non-Hodgkin Lymphoma is the Ann Arbor Staging System, sometimes with modifications (like the Lugano Classification).
The Ann Arbor system divides lymphoma into four main stages (I to IV), often with additional letters to provide more detail:
Ann Arbor Staging System
Stage I (I): The lymphoma is found in only one lymph node region or in a single extralymphatic organ (IE).
Example: Swollen lymph nodes in only the left side of the neck.
Stage II (II): The lymphoma is found in two or more lymph node regions on the same side of the diaphragm (either above or below). Or, it's in a single extralymphatic organ and nearby lymph nodes on the same side of the diaphragm (IIE).
Example: Swollen lymph nodes in the left armpit and left groin (both above the diaphragm).
Example: Lymphoma in the stomach and nearby abdominal lymph nodes.
Stage III (III): The lymphoma is found in lymph node regions on both sides of the diaphragm (above and below). It may also involve the spleen (IIIS) or an extralymphatic organ (IIIE or IIIE+S).
Example: Swollen lymph nodes in the neck and groin.
Stage IV (IV): This is the most advanced stage. The lymphoma has spread widely to one or more extralymphatic organs (organs outside the lymphatic system) in a diffuse or widespread manner, or to the bone marrow or central nervous system.
Example: Lymphoma cells found in the bone marrow or liver.
Additional Modifiers
In addition to the Roman numerals, doctors use letters to further describe the lymphoma:
A or B: This indicates the absence or presence of "B symptoms."
A: No B symptoms (no unexplained fever, night sweats, or significant weight loss).
B: Presence of B symptoms. The presence of B symptoms usually indicates more widespread disease and can affect prognosis and treatment choices.
E (Extralymphatic): Indicates that the lymphoma is found in an organ outside the lymphatic system.
Example: Stage IIE would mean lymphoma in lymph nodes on one side of the diaphragm and also in a nearby extralymphatic organ.
S (Spleen): Indicates involvement of the spleen.
Example: Stage IIIS would mean lymphoma on both sides of the diaphragm, plus spleen involvement.
X (Bulky Disease): This is sometimes used, especially for Hodgkin Lymphoma, to indicate a large tumor mass (often defined as >10 cm in diameter or a chest mass >1/3 the chest width). Bulky disease can sometimes require more intensive treatment.
Why Staging Matters
Staging helps the healthcare team:
Determine Prognosis: Generally, lower stages (I and II) have a better prognosis than higher stages (III and IV).
Plan Treatment: Treatment for early-stage lymphoma might involve localized radiation or fewer cycles of chemotherapy, while advanced stages often require more intensive systemic therapy.
Compare Results: Staging allows researchers and clinicians to compare the effectiveness of different treatments across patient groups.
Understanding your lymphoma's stage is a crucial piece of information in your treatment journey. Your doctor will explain your specific stage and what it means for your personalized care plan.
Risk Factors for Lymphoma: Who is at Risk?
While the exact cause of lymphoma is often unknown, research has identified several factors that can increase a person's risk of developing the disease. It's important to remember that having one or more risk factors does not mean you will definitely get lymphoma, and many people who develop lymphoma have no known risk factors.
Here are some of the common risk factors for both Hodgkin Lymphoma (HL) and Non-Hodgkin Lymphoma (NHL):
General Risk Factors for Both HL and NHL
Age:
HL: Has a bimodal distribution, meaning it's most common in young adults (ages 15-40) and older adults (over 55).
NHL: Risk generally increases with age, with most cases occurring in people over 60.
Gender:
HL: Slightly more common in men than women.
NHL: Slightly more common in men than women overall, though some subtypes may show different patterns.
Weakened Immune System: People with compromised immune systems are at a higher risk. This includes:
HIV/AIDS: The human immunodeficiency virus (HIV) significantly increases the risk of certain aggressive NHLs, particularly DLBCL and Burkitt lymphoma.
Organ Transplant Recipients: People who have received organ transplants and are on immunosuppressive drugs to prevent rejection have an increased risk.
Autoimmune Diseases: Conditions like rheumatoid arthritis, Sjögren's syndrome, and lupus are associated with a slightly increased risk of NHL.
Inherited Immunodeficiency Syndromes: Rare genetic conditions that impair immune function.
Risk Factors Specific to Hodgkin Lymphoma
Epstein-Barr Virus (EBV) Infection: Prior infection with EBV (the virus that causes mononucleosis) is linked to an increased risk of some types of classical HL, particularly mixed cellularity HL. However, most people infected with EBV do not develop HL.
Family History: Having a first-degree relative (parent, sibling, child) with HL slightly increases your risk.
Socioeconomic Status: Some studies suggest a higher incidence of HL in people from higher socioeconomic backgrounds, though the reasons are not fully understood.
Risk Factors Specific to Non-Hodgkin Lymphoma
Certain Infections:
Helicobacter pylori (H. pylori): This bacterium, which causes stomach ulcers, is a significant risk factor for gastric MALT lymphoma. Treating the infection can sometimes resolve the lymphoma.
Hepatitis C Virus (HCV): Chronic HCV infection is linked to an increased risk of certain NHLs, especially marginal zone lymphoma.
Human T-cell Lymphotropic Virus-1 (HTLV-1): This virus is associated with adult T-cell leukemia/lymphoma, particularly in certain geographic regions.
Epstein-Barr Virus (EBV): In addition to HL, EBV is linked to some types of NHL, such as Burkitt lymphoma (especially endemic forms) and post-transplant lymphoproliferative disorder (PTLD).
Exposure to Certain Chemicals and Toxins:
Pesticides and Herbicides: Some studies have linked exposure to certain agricultural chemicals (e.g., glyphosate) to an increased risk of NHL, though this remains an area of active research and debate.
Benzene: Exposure to benzene (a chemical found in gasoline and industrial settings) may increase risk.
Chemotherapy and Radiation Therapy: Previous treatment for other cancers with chemotherapy or radiation can slightly increase the risk of developing a secondary lymphoma years later.
Breast Implants: A rare type of T-cell lymphoma called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) has been linked to certain types of textured breast implants.
Obesity: Some studies suggest a link between obesity and an increased risk of certain NHLs.
It's important to understand that most people with these risk factors will never develop lymphoma, and many people who get lymphoma have no known risk factors. If you are concerned about your risk, discussing it with your doctor is always a good idea. They can provide personalized advice and discuss any preventive measures that might be appropriate. For general information on various conditions, including those related to immune health, it's always helpful to consult reliable medical resources.
Common Symptoms of Lymphoma: What to Look For
Recognizing the symptoms of lymphoma can be challenging because many of them are vague and can be caused by much more common and less serious conditions. However, being aware of persistent or worsening symptoms is crucial for early detection, which can significantly improve outcomes.
Here are the most common symptoms associated with lymphoma:
1. Swollen Lymph Nodes (Lymphadenopathy) 🎈
Description: This is often the most noticeable symptom. Lymph nodes become enlarged, usually feeling firm, rubbery, and typically painless.
Location: Most commonly found in the neck (above the collarbone), armpits, or groin. Lymphoma can also cause swelling of lymph nodes deep inside the chest or abdomen, which may not be visible or palpable but can cause symptoms by pressing on nearby organs.
Key Point: Unlike swollen lymph nodes due to an infection (which are often painful and tender), lymphoma-related lymph nodes are usually painless. If a swollen lymph node persists for more than a few weeks, especially without signs of infection, it should be evaluated by a doctor.
2. "B Symptoms" (Systemic Symptoms) 🥵💦📉
These three symptoms are particularly important for lymphoma diagnosis and staging, and their presence (or absence) is denoted by the "B" (or "A") modifier in the Ann Arbor staging system.
Unexplained Fever:
Description: Fevers that are persistent or recurrent, often occurring in the evenings or at night, without any clear infection. They may come and go over several days or weeks.
Drenching Night Sweats:
Description: Sweating so heavily at night that clothes and bedding become completely soaked, often requiring a change of pajamas or sheets. This is not just feeling warm; it's significant, drenching perspiration.
Unexplained Weight Loss:
Description: Losing 10% or more of your body weight within a 6-month period without trying to diet or increase exercise. This is significant and unintentional weight loss.
3. Fatigue 😴
Description: Persistent and overwhelming tiredness that doesn't improve with rest. This isn't just feeling sleepy; it's a profound exhaustion that can interfere with daily activities.
Cause: Can be due to the body fighting cancer, anemia (low red blood cell count) caused by lymphoma affecting the bone marrow, or the release of certain chemicals by cancer cells.
4. Itching (Pruritus) 🐾
Description: Generalized, often severe, and persistent itching all over the body, without a rash.
Cause: The exact cause is not fully understood, but it's thought to be related to substances released by the lymphoma cells.
Other Symptoms (Depending on the Location of Lymphoma)
The specific location of lymphoma can lead to a variety of other symptoms:
Chest:
Cough, shortness of breath, chest pain, or pressure (if lymphoma is in the mediastinum or lungs).
Swelling of the face and neck, sometimes with headaches and dizziness (superior vena cava syndrome), if a large tumor presses on the superior vena cava.
Abdomen:
Abdominal pain, swelling, feeling full quickly after eating small amounts, nausea, vomiting, or changes in bowel habits (if lymphoma affects the stomach, intestines, spleen, or abdominal lymph nodes).
Bone:
Bone pain, fractures (if lymphoma affects the bones).
Skin:
Rashes, red or purple patches, lumps, or tumors on the skin (especially with cutaneous lymphomas).
Brain/Spinal Cord (Central Nervous System):
Headaches, seizures, weakness, numbness, changes in sensation, balance problems, personality changes, or vision problems (rare but serious).
Loss of Appetite: Reduced desire to eat, contributing to weight loss.
Frequent Infections: A weakened immune system due to lymphoma can make you more susceptible to infections.
🗣️ "Listen to your body. While many symptoms are common, persistent changes, especially swollen lymph nodes or B symptoms, warrant a conversation with your doctor."
It's crucial to consult a healthcare professional if you experience any of these symptoms, especially if they are persistent, worsening, or occur in combination. Early diagnosis is key for effective treatment and better outcomes. If you have concerns about your health, don't hesitate to contact us for guidance.
The Diagnostic Journey: How Lymphoma is Identified
When a doctor suspects lymphoma based on symptoms and a physical exam, a series of diagnostic tests are initiated to confirm the diagnosis, determine the specific type, and assess the extent of the disease (staging). This comprehensive journey is critical for developing an effective, personalized treatment plan.
1. Medical History and Physical Exam
Medical History: The doctor will ask about your symptoms, how long you've had them, any family history of cancer, past infections, and other medical conditions.
Physical Exam: The doctor will carefully check for swollen lymph nodes in the neck, armpits, and groin, and examine the spleen and liver for enlargement. They will also look for other signs of lymphoma, such as skin changes or signs of infection.
2. Biopsy: The Gold Standard for Diagnosis
A biopsy is the most important test for diagnosing lymphoma. It involves removing a tissue sample for examination by a pathologist.
Excisional Biopsy: This is often preferred, especially for initial diagnosis of a swollen lymph node. The entire lymph node (or a significant part of a tumor) is surgically removed. This provides the pathologist with enough tissue to perform all necessary tests.
Core Needle Biopsy: A hollow needle is used to remove a small cylinder of tissue. This is less invasive than an excisional biopsy but may not provide enough tissue for a complete diagnosis in all cases.
Bone Marrow Biopsy and Aspiration: Samples of liquid bone marrow (aspiration) and a small piece of bone (biopsy) are taken, usually from the hip bone. This checks if lymphoma cells have spread to the bone marrow, which is crucial for staging.
Lumbar Puncture (Spinal Tap): If lymphoma is suspected in the brain or spinal cord (e.g., central nervous system lymphoma), a small amount of cerebrospinal fluid (CSF) is collected from the spinal canal for examination.
Pleural or Peritoneal Fluid Biopsy: If there's fluid buildup around the lungs (pleural effusion) or in the abdomen (ascites), a sample of the fluid can be taken and checked for lymphoma cells.
3. Pathological Examination and Special Tests
Once the biopsy sample is obtained, pathologists perform a series of sophisticated tests:
Microscopic Examination: The tissue is stained and examined under a microscope to identify abnormal cells, such as Reed-Sternberg cells for Hodgkin lymphoma, or the specific characteristics of Non-Hodgkin lymphoma cells.
Immunohistochemistry (IHC): Special stains are used to detect specific proteins (markers) on the surface of the lymphoma cells. These markers help determine if the lymphoma is of B-cell or T-cell origin and can help identify specific subtypes (e.g., CD20 for B-cell lymphomas, CD30 for ALCL and HL).
Flow Cytometry: This technique analyzes cells in a fluid sample (like blood or bone marrow) to identify specific cell surface markers, helping to classify the type of lymphoma.
Cytogenetics and FISH (Fluorescence In Situ Hybridization): These tests look for specific chromosomal abnormalities or genetic changes within the lymphoma cells (e.g., translocations like t(14;18) in follicular lymphoma or t(8;14) in Burkitt lymphoma). These genetic signatures are vital for accurate subtyping and guiding treatment.
Gene Expression Profiling: Newer techniques can analyze the activity of many genes in lymphoma cells, providing a deeper molecular understanding, particularly useful for aggressive lymphomas like DLBCL.
4. Imaging Tests: Visualizing the Extent of Disease
Imaging tests help determine where the lymphoma is located and how far it has spread.
CT Scan (Computed Tomography): Uses X-rays to create detailed cross-sectional images of the body. It's used to check for enlarged lymph nodes or tumors in the chest, abdomen, and pelvis.
PET Scan (Positron Emission Tomography): Often combined with a CT scan (PET-CT). A small amount of radioactive sugar is injected into the bloodstream. Cancer cells, which are highly active, absorb more sugar and "light up" on the scan, revealing the location and metabolic activity of tumors throughout the body. This is crucial for staging and assessing treatment response.
MRI (Magnetic Resonance Imaging): Uses powerful magnets and radio waves to create detailed images. It's particularly useful for imaging the brain and spinal cord if CNS involvement is suspected, or for soft tissues.
Ultrasound: May be used to examine superficial lymph nodes or organs in the abdomen.
5. Blood Tests
Various blood tests provide important information about your general health and can indirectly support a lymphoma diagnosis:
Complete Blood Count (CBC): Checks the number of red blood cells, white blood cells, and platelets. Lymphoma can sometimes affect blood counts.
Blood Chemistry Panel: Checks kidney and liver function, and levels of electrolytes.
Lactate Dehydrogenase (LDH): Elevated LDH levels can indicate aggressive lymphoma or a higher tumor burden.
Beta-2 Microglobulin: Another protein that can be elevated in lymphoma, sometimes used as a prognostic marker.
ESR (Erythrothrocyte Sedimentation Rate): Can be elevated in inflammatory conditions, including lymphoma.
Viral Tests: Tests for viruses like HIV, Hepatitis B, Hepatitis C, and EBV may be done, as these can be risk factors or co-existing conditions influencing treatment.
The diagnostic journey for lymphoma is thorough and relies on a combination of clinical assessment and advanced laboratory and imaging techniques. This comprehensive approach ensures an accurate diagnosis and staging, which are fundamental to developing an effective treatment strategy. If you have questions about specific diagnostic procedures or your overall health, our team of medical professionals is here to provide guidance and support.
Navigating Treatment Options: A General Overview
Once lymphoma is diagnosed, classified, and staged, the healthcare team will work with the patient to develop a personalized treatment plan. This plan is highly individualized and considers many factors, including:
The specific type and subtype of lymphoma (e.g., DLBCL, Follicular, Hodgkin).
The stage of the disease (how far it has spread).
The patient's age and overall health (performance status).
The presence of B symptoms.
Certain genetic markers or protein expressions on the lymphoma cells.
Patient preferences and potential side effects.
Treatment for lymphoma is often complex and may involve a combination of therapies.
1. "Watch and Wait" (Active Surveillance)
When Used: Primarily for asymptomatic, slow-growing (indolent) lymphomas, such as early-stage Follicular Lymphoma or some Marginal Zone Lymphomas.
Approach: Instead of immediate treatment, the patient is closely monitored with regular check-ups, physical exams, and imaging scans. Treatment is initiated only if the disease progresses, symptoms develop, or there's a risk of organ damage.
Benefit: Avoids unnecessary side effects of treatment for a period, maintaining quality of life.
2. Chemotherapy
Mechanism: Uses powerful anti-cancer drugs, usually given intravenously (IV) or orally, to kill rapidly dividing cells throughout the body.
Role: It's the cornerstone of treatment for most aggressive lymphomas (e.g., DLBCL, Burkitt, aggressive HL) and often used for indolent lymphomas when treatment is needed.
Regimens: Drugs are often given in combinations (e.g., R-CHOP for DLBCL, ABVD for HL) and in cycles, allowing the body to recover between treatments.
Side Effects: Can include fatigue, nausea, hair loss, mouth sores, increased risk of infection, and nerve damage, depending on the specific drugs.
3. Radiation Therapy
Mechanism: Uses high-energy X-rays or other particles to kill cancer cells in a targeted area.
Role: Can be used:
As a primary treatment for early-stage localized lymphoma.
After chemotherapy for bulky disease or residual disease.
To relieve symptoms (palliative radiation) like pain from a tumor.
For specific types like gastric MALT lymphoma.
Side Effects: Primarily localized to the treated area, such as skin irritation, fatigue, and potential long-term effects depending on the area irradiated.
4. Immunotherapy
Mechanism: These treatments harness the body's immune system to fight cancer or use lab-made immune components.
Types:
Monoclonal Antibodies: Drugs like Rituximab (targets CD20 on B-cells) are commonly used for B-cell lymphomas, often combined with chemotherapy. Brentuximab Vedotin (targets CD30) is used for HL and ALCL.
Checkpoint Inhibitors: (e.g., nivolumab, pembrolizumab) Block proteins that prevent immune cells from attacking cancer. Used for relapsed/refractory HL and some NHLs.
CAR T-Cell Therapy (Chimeric Antigen Receptor T-cell Therapy): A revolutionary treatment where a patient's own T-cells are collected, genetically modified to recognize and kill lymphoma cells, and then re-infused. Approved for certain relapsed/refractory aggressive B-cell NHLs (DLBCL, MCL, PMBL) in 2025.
Bispecific Antibodies: A newer type of immunotherapy that binds to both a lymphoma cell and a T-cell, bringing them together to allow the T-cell to kill the lymphoma cell.
5. Targeted Therapy
Mechanism: Drugs designed to attack specific vulnerabilities (molecular targets) within cancer cells, minimizing harm to healthy cells.
Role: Increasingly important, especially for certain NHL subtypes.
Examples:
BTK Inhibitors: (e.g., ibrutinib) for MCL, MZL, WM.
PI3K Inhibitors: for FL, MZL.
BCL-2 Inhibitors: (e.g., venetoclax) for certain lymphomas.
HDAC Inhibitors: for CTCL.
6. Stem Cell Transplant (Bone Marrow Transplant)
Mechanism: High doses of chemotherapy are given to destroy cancer cells (and healthy bone marrow), followed by infusion of healthy blood-forming stem cells to restore the bone marrow.
Types:
Autologous Transplant: Uses the patient's own stem cells, collected and stored before high-dose chemo. Often used for relapsed/refractory aggressive NHL and for some high-risk HL.
Allogeneic Transplant: Uses stem cells from a matched donor. Less common for lymphoma but may be considered for certain high-risk or relapsed cases, especially T-cell lymphomas.
Role: Can offer a chance for long-term remission or cure for patients who have relapsed or have high-risk disease.
7. Clinical Trials
Mechanism: Research studies that test new treatments, new combinations of existing treatments, or new ways to use current treatments.
Role: Offer access to cutting-edge therapies before they are widely available.
Consideration: Patients should discuss with their care team if a clinical trial is a suitable option for them.
Multidisciplinary Team Approach
Lymphoma treatment is managed by a multidisciplinary team, which typically includes:
Hematologist-Oncologist: A doctor specializing in blood cancers.
Radiation Oncologist: A doctor specializing in radiation therapy.
Pathologist: Analyzes tissue samples.
Radiologist: Interprets imaging scans.
Oncology Nurses: Provide care and support.
Social Workers, Nutritionists, Psychologists: Offer comprehensive supportive care.
This team approach ensures that all aspects of the patient's physical and emotional well-being are addressed throughout the treatment journey. For more information on patient care and support, visiting a comprehensive clinic or reviewing their FAQs can be very helpful.
Living with Lymphoma: Support and Resources
A diagnosis of lymphoma, regardless of its type, can be life-altering. Beyond the medical treatments, living with lymphoma involves managing physical side effects, addressing emotional challenges, and navigating the complexities of survivorship. In 2025, there are more resources and support systems available than ever before to help patients and their families cope.
Managing Physical Side Effects
Treatment for lymphoma can cause a range of side effects, both short-term and long-term.
Short-term: Fatigue, nausea, hair loss, mouth sores, nerve pain (neuropathy), and increased risk of infection are common during chemotherapy.
Long-term: Depending on the type of treatment, survivors might experience issues like heart problems, lung damage, secondary cancers, infertility, or cognitive changes ("chemo brain").
Managing these side effects requires close collaboration with your healthcare team. They can recommend medications, lifestyle adjustments, and supportive therapies (e.g., physical therapy, nutritional counseling) to alleviate discomfort and improve quality of life.
Addressing Emotional and Mental Health
The emotional toll of a cancer diagnosis is significant. Patients may experience:
Anxiety and Fear: About the future, treatment, and recurrence.
Depression: Feelings of sadness, hopelessness, and loss of interest.
Grief: For the loss of health, normal routine, or future plans.
Body Image Issues: Due to physical changes from treatment.
It's crucial to acknowledge these feelings and seek support.
Support Groups: Connecting with others who understand your experience can be incredibly validating and provide practical advice. Many organizations offer in-person and online support groups.
Counseling/Therapy: A mental health professional specializing in oncology can help patients and families process emotions, develop coping strategies, and manage stress.
Mindfulness and Relaxation Techniques: Practices like meditation, deep breathing, and yoga can help reduce stress and improve well-being.
Survivorship and Life After Treatment
For many, lymphoma is a treatable and often curable disease. However, the journey doesn't end when active treatment stops. Survivorship care focuses on:
Regular Follow-up: To monitor for recurrence and manage late effects of treatment.
Healthy Lifestyle: Emphasis on balanced nutrition, regular exercise, and avoiding smoking and excessive alcohol.
Screening for Secondary Cancers: Due to increased risk from previous treatments.
Financial and Practical Support: Addressing work-related issues, insurance, and daily living challenges.
Patient Advocacy and Information
Empowerment comes from knowledge. Patients and their families should feel comfortable asking questions and seeking information.
Reputable Websites: Organizations dedicated to lymphoma research and patient support provide vast amounts of reliable information.
Healthcare Team: Your doctors and nurses are your primary source of personalized information and guidance.
Patient Navigators: Some cancer centers offer patient navigators who can help coordinate care and connect you with resources.
🗣️ "You don't have to face lymphoma alone. A strong support system, both personal and professional, is a vital part of the healing process."
Living with lymphoma, whether during or after treatment, is a testament to resilience. By leveraging available support systems and actively participating in their care, patients can navigate this challenging time with greater strength and hope. For general information about our commitment to patient care and resources, please visit The Minor Surgery Center.
Emerging Research and Future Prospects in Lymphoma Treatment
The landscape of lymphoma treatment is continually evolving, driven by intensive research and a deeper understanding of the disease's biology. In 2025, patients have access to innovative therapies that were unimaginable just a decade ago, and the future holds even more promise.
1. Advanced Immunotherapies
Immunotherapy continues to be a rapidly expanding field in lymphoma:
CAR T-Cell Therapy Expansion: While already approved for several aggressive NHLs, research is ongoing to expand CAR T-cell therapy to more lymphoma subtypes (e.g., indolent lymphomas, T-cell lymphomas) and to improve its efficacy and reduce side effects. New "off-the-shelf" allogeneic CAR T-cell therapies (using donor cells) are also being investigated to make the treatment more accessible.
Bispecific Antibodies: These novel antibodies are designed to bring lymphoma cells and the patient's own T-cells together, enabling the T-cells to attack the cancer. Several bispecific antibodies are showing promising results in clinical trials for various NHLs, particularly for relapsed/refractory B-cell lymphomas.
Next-Generation Checkpoint Inhibitors: Further research into combination strategies with checkpoint inhibitors (e.g., combining them with chemotherapy or other immunotherapies) aims to enhance their effectiveness in more patients and subtypes.
2. Novel Targeted Therapies
As scientists uncover more about the specific genetic mutations and signaling pathways that drive different lymphoma subtypes, new targeted drugs are being developed:
BTK Inhibitors: Newer, more selective BTK inhibitors with improved side effect profiles are under investigation.
PI3K, EZH2, and SYK Inhibitors: These targeted drugs, already in use or clinical trials, block specific enzymes or pathways involved in lymphoma cell growth and survival. Research is exploring their use in combination or for specific patient populations.
Antibody-Drug Conjugates (ADCs): Like Brentuximab Vedotin, new ADCs are being developed that target different proteins on lymphoma cells, delivering chemotherapy directly to the cancer with fewer systemic side effects.
3. Precision Medicine and Biomarkers
The goal of precision medicine is to tailor treatment to the individual patient based on the specific molecular characteristics of their lymphoma.
Biomarker Identification: Researchers are actively identifying new biomarkers (measurable indicators of disease) that can predict which patients will respond best to certain therapies or indicate a higher risk of relapse. This allows for more personalized treatment selection.
Liquid Biopsies: Advanced blood tests (liquid biopsies) are being developed to detect circulating tumor DNA (ctDNA) or circulating tumor cells. These non-invasive tests can potentially help monitor disease response, detect minimal residual disease (MRD) after treatment, and identify early signs of relapse, guiding treatment adjustments in real-time.
4. Combination Therapies
Many current lymphoma treatments involve combinations of drugs. Future research is focused on optimizing these combinations, including:
Integrating new targeted agents and immunotherapies into standard chemotherapy regimens.
Developing chemotherapy-free regimens for certain subtypes, potentially reducing toxicity while maintaining efficacy.
Sequencing different therapies to maximize patient benefit and overcome resistance.
5. Early Detection and Risk Stratification
Improved Diagnostic Tools: Continued advancements in imaging (e.g., advanced PET techniques) and pathology (e.g., artificial intelligence-assisted diagnosis) aim to provide even more accurate and earlier diagnoses.
Risk Prediction Models: Better tools to identify individuals at higher risk for certain lymphoma types or those likely to have more aggressive disease can lead to earlier intervention or tailored preventive strategies.
The journey of lymphoma research is one of continuous discovery and innovation. These advancements offer tremendous hope for improved outcomes, reduced side effects, and ultimately, a better quality of life for individuals affected by lymphoma in 2025 and beyond. Patients seeking more information on the latest advancements or clinical trial opportunities can often find valuable resources and insights on a dedicated blog or by speaking with their care team.
The Importance of Early Detection and Awareness
In the fight against any cancer, early detection is a powerful weapon, and lymphoma is no exception. Catching lymphoma in its early stages often means that the disease is localized and has not spread extensively, making it more treatable and increasing the chances of a successful outcome.
Why Early Detection Matters:
Better Prognosis: For many types of lymphoma, especially Hodgkin Lymphoma and some aggressive Non-Hodgkin Lymphomas, early-stage diagnosis is associated with significantly higher cure rates.
Less Intensive Treatment: Early-stage disease may require less aggressive treatment (e.g., fewer cycles of chemotherapy, localized radiation), leading to fewer side effects and a better quality of life during and after treatment.
Prevention of Complications: Detecting lymphoma before it causes significant tumor growth or spreads to vital organs can prevent serious complications and organ damage.
Raising Awareness:
Because lymphoma symptoms can be vague and easily mistaken for common ailments, awareness is key.
Know the Symptoms: Familiarize yourself with the common signs, especially persistent swollen lymph nodes (painless), unexplained fevers, drenching night sweats, and significant unintentional weight loss (B symptoms).
Don't Dismiss Persistent Symptoms: If symptoms like persistent fatigue, itching, or swollen glands don't resolve within a few weeks, or if you experience B symptoms, don't hesitate to seek medical advice.
Regular Check-ups: Maintain regular visits with your primary care physician, who can monitor your overall health and address any concerns.
When to Seek Medical Advice 🩺
It's important to remember that most people who experience one or more of these symptoms do not have lymphoma. However, it is always best to consult a doctor if you experience:
A swollen lymph node that is painless, grows larger, or persists for more than a few weeks.
Any combination of B symptoms (unexplained fever, drenching night sweats, or unexplained weight loss).
Persistent fatigue that is overwhelming and not relieved by rest.
Any other concerning or persistent symptoms that are new or unusual for you.
Your doctor can evaluate your symptoms, conduct a physical examination, and order appropriate tests to determine the cause. Early evaluation is crucial for peace of mind and, if necessary, for prompt diagnosis and treatment. For any health concerns, reaching out to a healthcare provider is the best course of action. You can always visit our contact page to connect with medical professionals who can guide you.
Conclusion
Lymphoma is a diverse and complex group of cancers affecting the lymphatic system, a vital component of our immune defense. From the distinct characteristics of Hodgkin Lymphoma to the vast array of Non-Hodgkin Lymphoma subtypes, understanding these differences is paramount for effective diagnosis and treatment. In 2025, advancements in medical science offer a wide spectrum of personalized therapies, including chemotherapy, radiation, immunotherapy, targeted drugs, and stem cell transplants, leading to improved outcomes for many patients.
While the journey with lymphoma can be challenging, knowledge is power. Recognizing common symptoms, understanding the diagnostic process, and being aware of the various treatment options are crucial steps. Moreover, the importance of a strong support system, mental well-being, and continuous research cannot be overstated. By staying informed and working closely with a dedicated healthcare team, individuals affected by lymphoma can navigate their path with confidence and hope.