Mohs Surgery: The Gold Standard for Skin Cancer Treatment
Facing a skin cancer diagnosis can be a scary and uncertain time. You might be wondering about the best treatment options, how effective they are, and what the recovery process looks like. Among the many available treatments, Mohs Micrographic Surgery stands out as a highly effective and precise method, often referred to as the "gold standard" for certain types of skin cancer. But what exactly is Mohs surgery, and why is it so highly regarded?
This comprehensive guide will take you through everything you need to know about Mohs surgery, from its unique process to what you can expect before, during, and after the procedure. Our goal is to provide clear, understandable information to help you feel more informed and prepared for this important treatment.
Key Takeaways
Precision & High Cure Rate: Mohs surgery is unique because it removes skin cancer layer by layer and examines each layer under a microscope immediately. This precision allows surgeons to remove all cancer cells while saving as much healthy tissue as possible, leading to cure rates of up to 99% for certain skin cancers. 🎯
Tissue-Sparing: Unlike traditional surgery, Mohs minimizes the amount of healthy tissue removed. This is especially important for cancers on the face, hands, feet, or other areas where preserving appearance and function is key. ✨
Same-Day Results & Reconstruction: The entire Mohs procedure, including cancer removal and immediate microscopic examination, happens in one day. Once the cancer is confirmed to be fully removed, reconstruction of the wound can often begin immediately. 🩹
Specialized Expertise: Mohs surgery is performed by specially trained dermatologists who have expertise in dermatology, pathology, and reconstructive surgery. This specialized training ensures the highest level of care. 💪
Ideal for Specific Cancers: Mohs is most commonly used for basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), particularly those that are large, aggressive, recurrent, or located in sensitive areas.
What is Mohs Micrographic Surgery?
Mohs Micrographic Surgery, often simply called Mohs surgery, is a specialized surgical technique used to treat common types of skin cancer, including basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Developed by Dr. Frederic Mohs in the 1930s, this procedure has evolved significantly and is now recognized as the most effective treatment for many skin cancers.
What makes Mohs surgery unique is its meticulous and precise approach. It involves removing skin cancer layer by layer and examining each layer under a microscope immediately after it's removed. This allows the surgeon to identify and remove all cancer cells while preserving as much healthy surrounding tissue as possible. Imagine it like a highly detailed mapping process, where every edge and depth of the cancer is checked in real-time.
A Brief History of Precision
Dr. Frederic Mohs first developed this technique using a chemical fixative, which was later refined into the fresh tissue technique commonly used today. His innovation was revolutionary because, for the first time, surgeons could visually confirm that all cancer cells were removed during the surgery, not days later after a lab report. This real-time analysis dramatically improved cure rates and reduced the amount of healthy tissue that needed to be removed. Over the decades, Mohs surgery has become a cornerstone of dermatologic surgery, continually refined with advanced mapping and microscopic techniques.
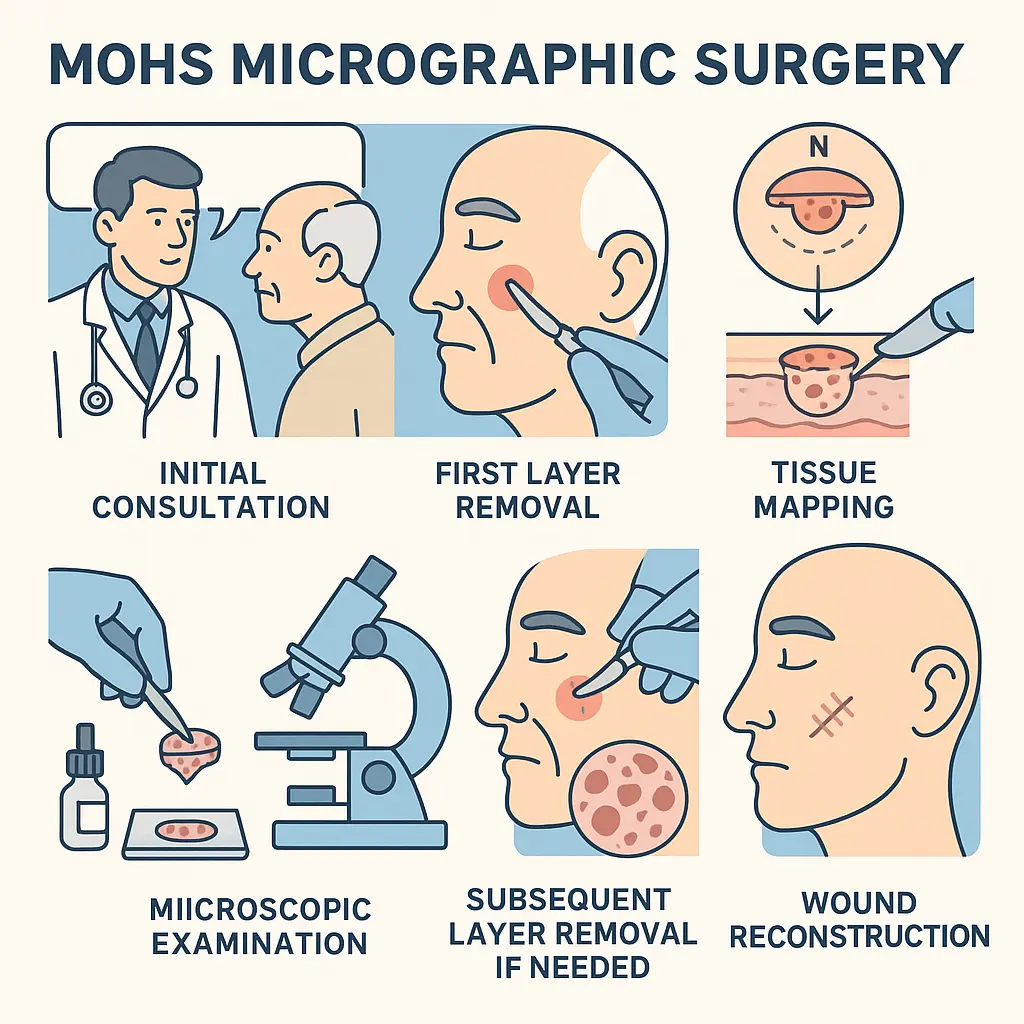
How Does Mohs Surgery Work? The Step-by-Step Process
Understanding the detailed steps of Mohs surgery can help ease any worries you might have. It's a precise process that combines surgery and pathology in one setting.
Step 1: Initial Consultation and Preparation 🤔
Before the actual surgery, you'll have an initial consultation with your Mohs surgeon. This is a crucial step where the surgeon will:
Review your diagnosis: Confirm the type and location of your skin cancer.
Discuss your medical history: Go over any medications you're taking, especially blood thinners, and any allergies. You might be advised to stop certain medications temporarily.
Explain the procedure: Detail what to expect on the day of surgery, including the number of layers, potential reconstruction, and recovery.
Answer your questions: This is your chance to voice any concerns or ask for clarification. Don't hesitate to ask about anything from the procedure itself to the recovery timeline.
It's a good idea to prepare a list of questions beforehand. On the day of the surgery, you should wear comfortable clothing, have a light meal, and arrange for someone to drive you home, especially if the surgery is on your face or involves sedation (though most Mohs surgeries use local anesthesia).
Step 2: The First Layer Removal (Excision) ✂️
On the day of the surgery, you'll arrive at the clinic. The area around the skin cancer will be cleaned and numbed using a local anesthetic. This means you'll be awake but won't feel any pain during the procedure. The Mohs surgeon then carefully removes a very thin layer of visible cancerous tissue, along with a small margin of surrounding skin. This first layer is removed with extreme precision, often in a saucer-like shape.
Step 3: Mapping and Marking the Tissue 🗺️
Once the tissue is removed, it's immediately marked with dyes to create a precise "map" that corresponds to the exact location on your skin. This map is critical because it allows the surgeon to know exactly where the cancer cells are located if they are still present. Think of it like a highly accurate GPS for your skin. The tissue is then carefully oriented and transferred to the on-site lab.
This is where the magic of Mohs truly happens. While you wait comfortably in the waiting room, the removed tissue is processed by a specialized Mohs histotechnician. They rapidly freeze the tissue, cut it into ultra-thin sections, and stain them. These stained sections are then placed on microscope slides.
Step 5: Microscopic Examination by the Surgeon 🧐
The Mohs surgeon, who is also a trained dermatopathologist, examines 100% of the margins (edges and underside) of the removed tissue under a microscope. This is the key difference from traditional pathology, where only a small sample of the margins might be checked. By examining all margins, the surgeon can see if any cancer cells remain.
If no cancer cells are found: Great news! The cancer has been completely removed.
If cancer cells are found: The surgeon identifies the exact location of the remaining cancer cells on the map.
Step 6: Subsequent Layer Removal (If Needed) 🔄
If cancer cells are still present, the surgeon goes back to the specific area on your skin where those cells were found (guided by the map) and removes another very thin layer of tissue only from that precise spot. This process is repeated – removal, mapping, lab analysis, microscopic examination – until no cancer cells are seen under the microscope. Each "stage" or "layer" typically takes about 45 minutes to an hour for processing and examination.
"The beauty of Mohs surgery lies in its ability to precisely target cancer cells while leaving healthy tissue untouched. It's truly a testament to medical precision."
Step 7: Reconstruction (Repair) of the Wound 🩹
Once the surgeon confirms that all cancer cells have been removed, the next step is to repair the wound. The method of reconstruction depends on the size and location of the wound, as well as your overall health and cosmetic goals. Options include:
Primary Closure: The wound edges are simply stitched together.
Skin Graft: Healthy skin is taken from another part of your body (donor site) and used to cover the wound.
Skin Flap: Tissue from an adjacent area is moved to cover the wound, maintaining its own blood supply.
Secondary Intention Healing: The wound is left to heal naturally over time. This is sometimes preferred for smaller wounds or in areas where a good cosmetic outcome can be achieved without stitches.
Your Mohs surgeon will discuss the best reconstruction option with you. Sometimes, a plastic surgeon or another specialist might be called in for more complex reconstructions, though often the Mohs surgeon performs the reconstruction themselves.
Why is Mohs Surgery Preferred? The Benefits
Mohs surgery offers several significant advantages that make it the preferred treatment for many skin cancers, especially those in sensitive or cosmetically important areas.
Highest Cure Rate 🏆
Mohs surgery boasts the highest cure rate among all skin cancer treatments, often reaching up to 99% for new basal cell and squamous cell carcinomas, and 95% for recurrent cancers. This extremely high success rate is due to the meticulous, real-time microscopic examination of 100% of the tumor margins. This ensures that every root and extension of the cancer is identified and removed.
Maximum Preservation of Healthy Tissue ✨
Because the surgeon only removes cancerous tissue and a minimal margin of healthy skin, Mohs surgery spares as much healthy tissue as possible. This is particularly important for cancers located on the face (nose, eyelids, lips, ears), hands, feet, and genitals, where preserving function and appearance is crucial. Minimizing tissue removal also leads to smaller scars and better cosmetic outcomes.
Real-Time Results ⏰
Unlike traditional excisions where you might wait days for lab results to confirm clear margins, with Mohs, the microscopic examination happens on-site during the surgery. This means you'll know on the same day that your cancer has been completely removed. This eliminates the anxiety of waiting and often allows for immediate reconstruction.
Cost-Effectiveness (in the long run) 💰
While the initial cost of Mohs surgery might seem higher than some other treatments, its high cure rate often makes it more cost-effective in the long run. By minimizing the chance of recurrence, it reduces the need for repeat surgeries, follow-up treatments, and the associated costs and emotional burden. For more information on skin cancer conditions and treatments, you can visit https://www.theminorsurgerycenter.com/conditions.
One-Day Procedure 🗓️
The entire process, from cancer removal to confirmation of clear margins and often reconstruction, typically happens in a single visit. This convenience saves patients multiple appointments and travel time.
Conditions Treated by Mohs Surgery
Mohs surgery is primarily used for common types of skin cancer, but its application can extend to certain rarer forms as well.
Basal Cell Carcinoma (BCC)
Basal cell carcinoma is the most common type of skin cancer. It often appears as a pearly bump, a sore that doesn't heal, or a flat, flesh-colored lesion. While BCC rarely spreads to other parts of the body, it can grow deep and wide if not treated, causing significant local tissue damage. Mohs surgery is highly effective for BCC, especially for:
Large BCCs: Tumors larger than 2 centimeters (about 0.8 inches).
BCCs in High-Risk Areas: These include the central face (nose, eyelids, lips, ears), scalp, neck, hands, and feet.
Aggressive Subtypes: Certain types of BCC, such as infiltrative, morpheaform, or micronodular, which have ill-defined borders and can be more challenging to remove completely.
Recurrent BCCs: Cancers that have returned after previous treatment.
Squamous Cell Carcinoma (SCC)
Squamous cell carcinoma is the second most common type of skin cancer. It often looks like a firm, red nodule, a scaly patch, or a sore that doesn't heal. SCC has a higher risk of spreading (metastasizing) than BCC, though this is still relatively rare. Mohs surgery is an excellent option for SCC, particularly for:
Large SCCs: Similar to BCCs, larger SCCs benefit from Mohs' precision.
SCCs in High-Risk Areas: Cancers on the lips, ears, eyelids, nose, or genitals, where preservation of tissue is critical.
Aggressive SCC Subtypes: Tumors that are poorly differentiated, rapidly growing, or have invaded nerves.
Recurrent SCCs: Cancers that have recurred after prior treatment.
SCCs in Immunosuppressed Patients: Individuals with weakened immune systems are at higher risk for aggressive SCCs.
Other Less Common Conditions
While BCC and SCC are the primary targets, Mohs surgery may also be considered for certain other skin conditions, including:
Melanoma in situ (Lentigo Maligna): A non-invasive form of melanoma that is confined to the top layer of the skin. Mohs can be an option for large or ill-defined lesions, especially on the face.
Dermatofibrosarcoma Protuberans (DFSP): A rare, slow-growing tumor that tends to recur locally.
Merkel Cell Carcinoma: A rare, aggressive skin cancer, though Mohs is typically used in conjunction with other treatments for this type.
Atypical Fibroxanthoma (AFX): A rare tumor that can resemble SCC.
The decision to use Mohs surgery for these less common conditions is made on a case-by-case basis, considering the tumor's characteristics and location.
When is Mohs Surgery Recommended?
The recommendation for Mohs surgery isn't arbitrary; it's based on specific criteria that highlight its benefits over other treatment methods.
The Mohs Surgeon's Expertise
A Mohs surgeon isn't just any dermatologist. They undergo highly specialized training that makes them uniquely qualified to perform this intricate procedure.
Specialized Training and Board Certification 🎓
After completing medical school and a dermatology residency, a Mohs surgeon typically completes an additional one to two-year fellowship training program approved by the American College of Mohs Surgery (ACMS) or an equivalent recognized body. This fellowship provides extensive, hands-on experience in:
Dermatologic Surgery: Advanced techniques for removing skin lesions.
Pathology: In-depth training in interpreting tissue slides under a microscope, specifically for skin cancers.
Reconstructive Surgery: Skills to repair surgical wounds, from simple closures to complex flaps and grafts.
This triple expertise in surgery, pathology, and reconstruction within a single individual is what sets Mohs surgeons apart. It allows them to act as surgeon, pathologist, and reconstructive surgeon all in one visit, ensuring seamless and precise care. When choosing a surgeon, look for one who is board-certified in dermatology and has completed an ACMS fellowship. You can learn more about the team at https://www.theminorsurgerycenter.com/team.
Preparing for Mohs Surgery
Proper preparation can make your Mohs surgery experience smoother and less stressful.
Before Your Appointment 📋
Medication Review: Inform your surgeon about ALL medications you are taking, including prescriptions, over-the-counter drugs, supplements, and herbal remedies. Special attention will be given to blood thinners (like aspirin, ibuprofen, warfarin, clopidogrel) as they can increase bleeding. Your surgeon will advise if you need to stop or adjust any medications.
Alcohol and Smoking: Avoid alcohol for at least 24-48 hours before surgery, as it can thin the blood. If you smoke, try to reduce or stop before surgery, as smoking can impair healing.
Arrange Transportation: While Mohs surgery is usually performed under local anesthesia, it's wise to have someone drive you home, especially if the surgery is on your face or if you anticipate discomfort.
Comfortable Clothing: Wear loose, comfortable clothing that allows easy access to the surgical site. If the surgery is on your head or neck, avoid tight collars.
Eat a Light Meal: Unless otherwise instructed, eat a light breakfast or lunch before your arrival.
Bring Entertainment: Mohs surgery can be a lengthy process with waiting periods between stages. Bring a book, magazine, tablet, or headphones to help pass the time.
Hydrate: Drink plenty of water in the days leading up to your surgery.
Questions: Write down any questions or concerns you have so you don't forget to ask them during your consultation or on the day of surgery. For common questions, you might find answers at https://www.theminorsurgerycenter.com/faqs.
The Day of Mohs Surgery ☀️
On the day of your surgery, arrive at the clinic well-rested. You will be greeted by the surgical team who will guide you through the process. The procedure room is typically a comfortable, outpatient setting. The focus is on making you feel at ease throughout the day.
What Happens During the Procedure? A Deeper Dive
Let's expand on the steps to give you an even clearer picture of what to expect during the actual surgery.
Numbing the Area 💉
The first step on the operating table is the administration of a local anesthetic around the tumor. This is typically done with a very fine needle, and you might feel a slight sting, similar to a dental injection. Once the area is numb, you won't feel any pain during the excision. The surgeon will test the area to ensure it's completely numb before proceeding.
The First Surgical Excision 🔪
Using a scalpel, the surgeon carefully removes the visible tumor along with a very thin margin of surrounding skin. This initial layer is typically very shallow and saucer-shaped, designed to minimize the size of the final defect. The goal is to remove as little healthy tissue as possible while getting the bulk of the tumor.
Dressing and Waiting 🛋️
After the first layer is removed, a temporary bandage will be placed over the wound. You will then be escorted to a comfortable waiting area. This is the period where the tissue is processed in the lab. The waiting time can vary, but typically ranges from 45 minutes to an hour per stage. Some patients bring snacks, drinks, and entertainment to make this time more pleasant.
The Mohs Lab: A Closer Look 🧪
The tissue removed is immediately taken to an on-site laboratory. Here, a specially trained technician (histotechnician) prepares the tissue.
Freezing: The tissue is flash-frozen to make it firm enough to slice.
Sectioning: It's then cut into extremely thin slices (microns thick) using a cryostat (a special microtome in a freezer).
Staining: These slices are placed on glass slides and stained with special dyes that make cancer cells visible under a microscope.
Mounting: The slides are then prepared for microscopic examination.
This rapid processing allows for immediate analysis, which is the cornerstone of Mohs.
Microscopic Examination and Decision Making 🎯
Your Mohs surgeon, armed with their pathology expertise, meticulously examines every single edge and the deep surface of the tissue on the slides. They are looking for any remaining cancer cells.
If no cancer cells are found: The surgeon confirms that the area is clear. The procedure for cancer removal is complete, and attention turns to wound repair.
If cancer cells are found: The surgeon pinpoints the exact location of the remaining cancer cells on the tissue map. This map is then used to guide the next excision.
Subsequent Stages (If Necessary) 🔁
If cancer cells are still present, the surgeon returns to the precise area on your skin indicated by the map. They will numb the area again if needed and remove only the small portion of skin where cancer cells remain. This minimizes the wound size and protects healthy tissue. This process of removal, mapping, lab processing, and microscopic examination is repeated until all margins are clear. It's not uncommon for patients to require two or three stages, though some complex or aggressive tumors may require more.
Reconstruction After Mohs Surgery
Once the Mohs surgeon confirms that all cancer cells have been removed, the next crucial step is to repair the surgical wound. The goal of reconstruction is to restore the skin's appearance and function as much as possible.
Factors Influencing Reconstruction Choice:
Size and Depth of the Wound: Larger and deeper wounds require more complex repair.
Location of the Wound: Wounds on the face, especially around the eyes, nose, or mouth, require careful consideration to preserve delicate structures and cosmetic appearance.
Skin Laxity: The looseness or tightness of the surrounding skin impacts how easily the wound can be closed.
Your Overall Health: Underlying health conditions can influence healing.
Cosmetic Goals: Your preferences and expectations for the final appearance.
Common Reconstruction Options:
Primary Closure (Stitching Together) 🧵:
Description: This is the simplest and most common method for smaller wounds or those in areas with enough loose skin. The surgeon carefully brings the edges of the wound together and stitches them closed.
Benefits: Often results in a fine, linear scar. Quick healing.
Best for: Small to medium-sized wounds, areas with good skin elasticity (e.g., forehead, cheek).
Secondary Intention Healing (Natural Healing) 🌱:
Description: In some cases, especially for shallow wounds or those in concave areas (like the inner corner of the eye or parts of the ear), the wound is left open to heal naturally. The body fills in the wound with new tissue.
Benefits: Avoids additional incisions, can result in very good cosmetic outcomes in specific areas, especially if the wound is small and circular.
Best for: Small, shallow wounds, areas where skin can contract well, or areas where a graft/flap might look worse.
Skin Graft (Patch of Skin) 🧩:
Description: A thin piece of healthy skin is taken from another part of your body (the "donor site," often behind the ear, collarbone, or upper arm) and transferred to cover the wound. The graft does not have its own blood supply initially; it relies on the wound bed for nutrients until new blood vessels grow into it.
Types:
Split-Thickness Graft: Involves only the top layers of skin.
Full-Thickness Graft: Includes all layers of skin, providing a better cosmetic match but requiring a larger donor site.
Benefits: Can close larger defects where primary closure isn't possible.
Considerations: Two wounds (surgical site and donor site) need to heal. The graft may look slightly different in color or texture from the surrounding skin.
Skin Flap (Moving Tissue) 🔄:
Description: A flap involves moving a section of skin and underlying tissue (which retains its own blood supply) from an area adjacent to the surgical wound to cover the defect.
Benefits: Provides excellent color and texture match because the tissue is local. Can be used to fill deeper defects and restore contours.
Considerations: More complex than grafts, may involve an additional incision to create the flap, and can temporarily distort the surrounding skin.
Who Performs the Reconstruction?
Often, the Mohs surgeon themselves performs the reconstruction immediately after confirming clear margins. Their extensive training in reconstructive techniques allows them to handle a wide range of closures. For very large or complex defects, especially those involving critical structures or requiring specialized plastic surgery, the Mohs surgeon may collaborate with or refer you to a plastic surgeon or another specialist (e.g., oculoplastic surgeon for eyelid defects).
The decision about reconstruction is a shared one between you and your surgeon, taking into account the best functional and cosmetic outcome for your specific situation.
Recovery After Mohs Surgery
The recovery process after Mohs surgery is generally straightforward, but proper wound care is essential for optimal healing and scar appearance.
Immediate Post-Procedure Care 🩹
Pressure Dressing: A pressure dressing is often applied to the wound immediately after reconstruction to minimize swelling and bleeding. You'll be given specific instructions on when and how to remove it.
Pain Management: Most patients experience mild discomfort rather than severe pain. Over-the-counter pain relievers like acetaminophen (Tylenol) are usually sufficient. Avoid aspirin or ibuprofen unless approved by your surgeon, as they can increase bleeding.
Swelling and Bruising: Some swelling and bruising around the surgical site are normal, especially if the surgery was on the face. Applying a cold compress (ice pack) intermittently for the first 24-48 hours can help reduce this.
Bleeding: Minor oozing is common for the first 24 hours. Apply firm, constant pressure to the wound with a clean gauze for 15-20 minutes if bleeding occurs. If bleeding is heavy or persistent, contact your surgeon.
Wound Care Instructions 🧼
Your surgeon or nurse will provide detailed, specific instructions tailored to your wound. General guidelines often include:
Keep it Clean: Gently clean the wound daily with mild soap and water or as instructed. Pat dry.
Apply Ointment: Apply a thin layer of petroleum jelly (like Vaseline) or an antibiotic ointment (if recommended) to keep the wound moist. This helps prevent scab formation, which can hinder healing and worsen scarring.
Cover the Wound: Keep the wound covered with a non-stick bandage to protect it from dirt and injury. Change the bandage daily or as instructed.
Avoid Submerging: Do not submerge the wound in baths, swimming pools, or hot tubs until it is fully healed and sutures are removed. Showering is usually fine, but avoid direct water pressure on the wound.
Activity Restrictions: Avoid strenuous activities, heavy lifting, or bending at the waist for a period (usually 1-2 weeks) as recommended by your surgeon. These activities can increase blood pressure at the wound site, leading to bleeding or stretching of the scar.
Follow-Up Appointments ✅
You will have follow-up appointments to:
Remove Sutures: Typically 5-14 days after surgery, depending on the location.
Monitor Healing: The surgeon will check the wound's progress and address any concerns.
Discuss Scar Management: Advice on minimizing scar appearance.
Potential Side Effects and Complications ⚠️
While Mohs surgery is generally safe, like any surgical procedure, it carries some potential risks:
Bleeding: Minor bleeding is common; significant bleeding is rare.
Infection: Though precautions are taken, infection can occur. Signs include increased redness, swelling, pain, warmth, or pus.
Scarring: All surgery leaves a scar. Mohs aims to minimize it, but the final appearance depends on wound size, location, and individual healing.
Nerve Damage: Temporary or, rarely, permanent numbness or weakness can occur if a nerve is close to the surgical site.
Pain and Discomfort: Usually mild and manageable with over-the-counter pain relievers.
Bruising and Swelling: Common and usually resolves within a few weeks.
Itching: The healing wound may feel itchy.
Allergic Reaction: To anesthetic, tape, or ointments.
Always contact your surgeon's office if you experience unusual pain, excessive bleeding, signs of infection, or any other concerning symptoms.
Scarring and Cosmetic Outcomes
One of the major advantages of Mohs surgery is its focus on maximizing healthy tissue preservation, which directly contributes to better cosmetic outcomes. However, it's important to have realistic expectations about scarring.
Understanding Scars ✨
Anytime the skin is cut, a scar will form. The size, shape, and visibility of the scar depend on several factors:
Original Wound Size and Depth: Larger and deeper wounds naturally result in more noticeable scars.
Location: Scars on areas with more tension (e.g., shoulders, chest) or high movement (e.g., joints) tend to be more prominent. Scars on the face often heal very well due to rich blood supply.
Individual Healing: Genetics play a significant role. Some people are prone to raised (hypertrophic or keloid) scars.
Reconstruction Method: Different repair techniques can lead to different scar appearances.
Post-Operative Care: Diligent wound care significantly impacts the final scar.
Minimizing Scar Appearance 💪
Your Mohs surgeon will employ techniques to minimize scarring, but you also have a role in scar management:
Follow Wound Care Instructions: Keeping the wound clean and moist is paramount.
Protect from Sun: New scars are very sensitive to sunlight and can hyperpigment (turn dark) if exposed. Use broad-spectrum sunscreen (SPF 30+) diligently or cover the scar with clothing.
Massage: Once the wound is fully closed and sutures are removed, gentle massage with a moisturizing cream or silicone gel can help soften and flatten the scar.
Silicone Products: Silicone sheets or gels can be very effective in improving scar appearance, especially for raised scars.
Avoid Tension: For weeks to months after surgery, avoid putting excessive tension on the healing scar, which can cause it to widen.
Patience: Scars mature over time. It can take 6-12 months, or even longer, for a scar to fully fade and flatten.
Scar Revision Options 🎨
If, after the scar has fully matured, you are still unhappy with its appearance, there are options for scar revision. These might include:
Steroid Injections: To flatten raised scars.
Laser Treatments: To improve redness, texture, or pigmentation.
Dermabrasion or Microneedling: To smooth scar texture.
Surgical Scar Revision: In some cases, a surgeon can re-excise and meticulously re-suture the scar to improve its appearance.
Your Mohs surgeon can advise you on the best approach for scar management and revision.
Long-Term Follow-Up and Skin Cancer Prevention
Undergoing Mohs surgery is a significant step in treating your current skin cancer, but it's also a reminder of the importance of ongoing skin health and cancer prevention.
Regular Skin Exams 🩺
If you've had one skin cancer, you are at a higher risk of developing another. Therefore, regular full-body skin exams are crucial:
Self-Exams: Perform monthly self-skin checks at home, looking for any new or changing moles, spots, or sores. Pay attention to areas exposed to the sun.
Dermatologist Exams: Schedule regular check-ups with your dermatologist, typically every 6 to 12 months, or as recommended based on your personal risk factors. Your dermatologist will examine your entire skin surface, including areas you can't easily see.
Sun Protection Strategies ☀️
The sun's ultraviolet (UV) radiation is the primary cause of most skin cancers. Protecting your skin from the sun is the most effective way to prevent new cancers and reduce the risk of recurrence.
Seek Shade: Especially between 10 AM and 4 PM when the sun's rays are strongest.
Wear Protective Clothing: Long-sleeved shirts, long pants, and wide-brimmed hats (at least 3 inches wide) offer excellent protection. Look for clothing with a UPF (Ultraviolet Protection Factor) rating.
Use Broad-Spectrum Sunscreen: Apply generously (about a shot glass full for your body) to all exposed skin.
SPF 30 or higher: Blocks 97% of UVB rays.
"Broad-spectrum": Protects against both UVA and UVB rays.
Water-resistant: If you're swimming or sweating.
Reapply every two hours, or more often if swimming or sweating.
Avoid Tanning Beds: Tanning beds emit dangerous UV radiation and significantly increase your risk of skin cancer.
Sunglasses: Protect your eyes and the delicate skin around them with sunglasses that block 99-100% of UVA and UVB rays.
By integrating these practices into your daily life, you can significantly reduce your risk of future skin cancers and maintain healthy skin for years to come. For more general information about skin health and conditions, you can explore resources like https://www.theminorsurgerycenter.com/blog.
Comparing Mohs to Other Skin Cancer Treatments
While Mohs surgery is the gold standard for many skin cancers, it's not the only option. Understanding how it compares to other treatments can help you appreciate its unique advantages.
1. Standard Surgical Excision (Excisional Surgery) 🔪
How it Works: The surgeon removes the visible tumor along with a predetermined margin of healthy-appearing skin (e.g., 4-6 mm). The tissue is then sent to an off-site lab for pathological examination.
Pros: Effective for many small, well-defined, non-aggressive skin cancers, especially on the trunk or limbs.
Cons:
Blind Margins: The surgeon doesn't know if all cancer cells are removed until days later when lab results return. If margins are positive, a second surgery is often needed.
Less Tissue Sparing: A larger margin of healthy tissue is removed upfront, which can lead to larger defects and scars, especially in cosmetically sensitive areas.
Mohs Advantage: Real-time microscopic control ensures complete removal on the same day, minimizing tissue removal and reducing the need for repeat surgeries.
2. Radiation Therapy ☢️
How it Works: High-energy X-rays are used to destroy cancer cells. It's typically administered over several weeks in multiple sessions.
Pros: Non-invasive (no cutting), can be an option for patients who cannot undergo surgery due to health reasons or for large, inoperable tumors.
Cons:
Lower Cure Rates: Generally has lower cure rates than surgery, especially for recurrent cancers.
Side Effects: Can cause skin redness, irritation, fatigue, and long-term changes to the skin (thinning, scarring, telangiectasias).
No Immediate Confirmation: Cancer cells are not immediately confirmed as removed.
Long Treatment Course: Requires multiple visits over weeks.
Mohs Advantage: Higher cure rates, immediate confirmation of clear margins, and a single-day procedure.
3. Cryosurgery (Freezing) 🥶
How it Works: Liquid nitrogen is used to freeze and destroy cancer cells.
Pros: Quick, relatively simple, and non-invasive.
Cons:
Limited Precision: The depth of freezing is hard to control, leading to potential under-treatment (recurrence) or over-treatment (excessive scarring).
No Margin Control: No tissue is sent for pathology, so there's no microscopic confirmation of complete removal.
Not for Aggressive Cancers: Not suitable for large, deep, or aggressive tumors.
Mohs Advantage: Precision, microscopic control, and higher cure rates.
How it Works: Medicated creams applied to the skin to destroy superficial cancer cells.
Pros: Non-invasive, can be done at home.
Cons:
Limited to Superficial Cancers: Only effective for very superficial BCCs or SCCs in situ (Bowen's disease). Not suitable for invasive, nodular, or aggressive cancers.
Inflammatory Reaction: Can cause significant redness, scabbing, and irritation during treatment.
No Margin Control: No microscopic confirmation of complete removal.
Long Treatment Course: Requires daily application for weeks or months.
Mohs Advantage: Precision, microscopic control for invasive cancers, and a single-day treatment for definitive removal.
5. Curettage and Electrodessication (Scraping and Burning) 🔥
How it Works: The tumor is scraped off with a sharp instrument (curette), and the base is then burned with an electric current to destroy remaining cells and stop bleeding. This process is often repeated.
Pros: Quick, relatively simple, can be effective for small, superficial BCCs and SCCs.
Cons:
Less Precise: Relies on the surgeon's tactile feel rather than microscopic confirmation of margins.
Not for Aggressive Cancers: Not recommended for large, deep, recurrent, or aggressive tumors.
Scarring: Can leave a round, depressed scar.
Mohs Advantage: Microscopic precision leads to higher cure rates and better cosmetic outcomes, especially for challenging tumors.
This comparison highlights why Mohs surgery is often recommended for specific, more challenging skin cancers where precision, high cure rates, and cosmetic outcomes are paramount.
Cost of Mohs Surgery and Insurance Coverage
Understanding the financial aspect of Mohs surgery is an important part of your preparation.
Factors Influencing Cost 💲
The total cost of Mohs surgery can vary based on several factors:
Number of Stages: Each stage of cancer removal and microscopic examination adds to the cost. The more complex the cancer, the more stages may be needed.
Location of the Tumor: Cancers on the face, hands, or other complex areas may require more intricate reconstruction, potentially increasing costs.
Type of Reconstruction: Simple primary closures are less expensive than complex flaps or grafts.
Anesthesia: Mohs is typically performed under local anesthesia, which is less costly than general anesthesia. If sedation is used, it may add to the cost.
Geographic Location: Costs can vary by region and clinic.
Surgeon's Fees: The surgeon's experience and reputation can influence fees.
Facility Fees: Costs associated with using the surgical facility and its equipment.
Pathology Fees: The on-site lab work is a significant component of Mohs.
Insurance Coverage 🛡️
Mohs surgery is considered a medically necessary procedure for treating skin cancer and is generally covered by most health insurance plans, including Medicare and Medicaid. However, the extent of coverage can vary:
Deductibles: You will likely be responsible for meeting your plan's deductible before insurance coverage kicks in.
Co-pays/Co-insurance: Once your deductible is met, you will typically pay a co-pay or co-insurance percentage of the approved amount.
Out-of-Pocket Maximums: Most plans have an annual out-of-pocket maximum, after which the plan pays 100% of covered services.
Pre-authorization: Some insurance companies require pre-authorization for Mohs surgery. Your clinic's billing department will usually handle this.
In-Network vs. Out-of-Network: Ensure your Mohs surgeon and the facility are in-network with your insurance plan to minimize your out-of-pocket costs.
It is highly recommended to contact your insurance provider directly before your surgery to understand your specific benefits, coverage limits, and any required pre-authorizations. The clinic's billing staff can often assist you with this process and provide an estimate of costs. For billing and insurance questions, you might find it helpful to contact the clinic directly at https://www.theminorsurgerycenter.com/contact.
Choosing a Mohs Surgeon and Clinic
Selecting the right Mohs surgeon and clinic is a crucial decision that can significantly impact your treatment outcome and experience.
Key Factors to Consider:
Board Certification and Fellowship Training:
Board-Certified Dermatologist: Ensure the surgeon is board-certified in dermatology.
Mohs Fellowship Training: Crucially, confirm they have completed a fellowship in Mohs Micrographic Surgery and Dermatologic Oncology, ideally one accredited by the American College of Mohs Surgery (ACMS). This ensures they have the specialized training in surgical technique, pathology, and reconstruction.
Why it matters: This dual expertise means the same doctor performing the surgery is also the one interpreting the slides in real-time, leading to the highest precision and safety.
Experience:
Volume of Procedures: Ask about the number of Mohs procedures the surgeon performs annually. A high volume often indicates extensive experience with various types and complexities of skin cancers.
Experience with Your Specific Cancer: Inquire if they have particular expertise with the type of skin cancer you have (e.g., recurrent BCC, SCC on the nose).
On-Site Lab and Team:
Accredited Lab: A dedicated, on-site Mohs laboratory is essential for the real-time analysis that defines Mohs surgery. Ensure the lab is properly equipped and staffed by trained histotechnicians.
Support Staff: A professional, compassionate, and well-trained support staff (nurses, medical assistants, administrative staff) contributes to a smooth and comfortable experience.
Communication Style and Patient Comfort:
Clear Explanations: The surgeon should explain the procedure clearly, answer all your questions, and discuss potential outcomes and risks in an understandable way.
Empathetic Approach: Look for a surgeon and staff who make you feel comfortable and address your concerns with empathy.
Patient Reviews: Online reviews can offer insights into other patients' experiences with the surgeon and clinic.
Facility Accreditation and Environment:
Accreditation: While not always required for office-based surgery, accreditation by bodies like the Accreditation Association for Ambulatory Health Care (AAAHC) can indicate a commitment to high standards of patient care and safety.
Cleanliness and Comfort: The clinic should be clean, well-organized, and provide a comfortable waiting area, especially since Mohs surgery can involve waiting periods.
Insurance and Billing:
Insurance Acceptance: Confirm that the clinic accepts your insurance plan and is in-network.
Billing Transparency: The clinic should be transparent about costs and help you understand your financial responsibilities.
Where to Find a Qualified Mohs Surgeon:
American College of Mohs Surgery (ACMS): Their website has a "Find a Mohs Surgeon" tool that lists fellowship-trained and board-certified members.
Referrals: Your referring dermatologist or primary care physician can often provide excellent recommendations.
Online Directories: Reputable medical directories can help you find qualified specialists in your area.
Choosing a Mohs surgeon is a partnership. Take your time, do your research, and don't hesitate to ask questions to ensure you feel confident in your choice. For general information about clinics and their services, you can visit https://www.theminorsurgerycenter.com/clinic.
Frequently Asked Questions (FAQs) About Mohs Surgery
Here are answers to some common questions patients have about Mohs surgery.
Q1: How long does Mohs surgery take?
A1: The total time can vary greatly. The initial excision takes about 15-20 minutes. However, each subsequent stage of lab processing and microscopic examination takes about 45-60 minutes. Depending on the number of stages needed and the complexity of reconstruction, the entire process can take anywhere from a few hours to a full day. It's best to plan to be at the clinic for most of the day.
Q2: Will I be asleep during the surgery?
A2: No, Mohs surgery is almost always performed under local anesthesia. This means the surgical area will be completely numb, but you will be awake and alert. You will be able to talk to the surgical team during the procedure. This avoids the risks and recovery associated with general anesthesia.
Q3: Will it hurt?
A3: You will feel a slight sting when the local anesthetic is injected, similar to a dental shot. Once the area is numb, you should not feel any pain during the excision. You might feel some pressure or tugging. After the anesthetic wears off, you may experience mild discomfort, which is usually manageable with over-the-counter pain relievers.
Q4: Will I have a scar?
A4: Yes, any time the skin is cut, a scar will form. However, Mohs surgery is designed to remove the minimum amount of tissue necessary, leading to the smallest possible scar. Your surgeon will also use advanced reconstructive techniques to optimize the cosmetic outcome. Scars typically fade and improve significantly over 6-12 months.
Q5: Can the cancer come back after Mohs surgery?
A5: While Mohs surgery has the highest cure rate (up to 99% for new BCCs and SCCs), no treatment can guarantee 100% success. There is always a small chance of recurrence. However, due to its precision, Mohs significantly reduces this risk compared to other methods. Regular follow-up skin exams are essential to detect any recurrence or new skin cancers early.
Q6: What should I bring with me on the day of surgery?
A6: Bring something to read or do during the waiting periods (book, tablet, headphones), snacks and drinks (if allowed by the clinic), and comfortable clothing. If you have a list of questions, bring that too. Don't forget your insurance card and photo ID.
Q7: When can I go back to work or my normal activities?
A7: This depends on the location of the surgery, the size of the wound, and your type of work. Many people can return to light activities the next day. However, strenuous activities, heavy lifting, and bending should be avoided for 1-2 weeks to prevent bleeding or stretching of the wound. Your surgeon will provide specific post-operative instructions.
Q8: What if I am on blood thinners?
A8: It is crucial to discuss all medications, especially blood thinners, with your Mohs surgeon well in advance of your procedure. In many cases, it is safer to continue blood thinners, but your surgeon will make a personalized recommendation based on your health and the specific medication. Do NOT stop any prescribed medication without consulting your surgeon and the prescribing doctor.
Q9: Can Mohs surgery be used for melanoma?
A9: Mohs surgery is generally not the primary treatment for invasive melanoma. Standard surgical excision with wider margins is typically preferred. However, Mohs may be considered for a specific type of early, non-invasive melanoma called lentigo maligna (melanoma in situ), especially on the face, due to its ability to spare tissue.
Conclusion
Mohs Micrographic Surgery represents a pinnacle of precision and effectiveness in the treatment of skin cancer. Its unique ability to combine surgical removal, immediate microscopic examination of 100% of the tumor margins, and on-site reconstruction offers patients the highest possible cure rates while preserving the maximum amount of healthy tissue. This makes it an invaluable option for challenging skin cancers, particularly those located in cosmetically or functionally sensitive areas.
While the process involves waiting periods and the recovery requires diligent wound care, the long-term benefits of Mohs surgery – including superior outcomes, minimized scarring, and reduced risk of recurrence – make it the preferred choice for many patients.
If you or a loved one has been diagnosed with skin cancer, discussing Mohs surgery with a fellowship-trained Mohs surgeon is an important step. They can assess your specific situation, explain if Mohs is the right choice for you, and guide you through every step of the journey, helping you achieve the best possible health and cosmetic outcome. Remember, early detection and appropriate treatment are key to successfully managing skin cancer.