Imagine a tiny, innocent-looking mole on your skin. For most people, it's just a part of their unique canvas. But sometimes, this small spot can hide a secret: melanoma, a serious form of skin cancer. While detecting melanoma early often leads to successful treatment, what happens when it's found at a more advanced stage? What does "late-stage melanoma" truly mean, and what are the paths forward for those facing this challenging diagnosis?
This article aims to shed light on late-stage melanoma, breaking down the complexities of its diagnosis, treatment, and management. We'll explore the science behind how melanoma progresses, the groundbreaking therapies that offer new hope, and the crucial support systems that help patients and their families navigate this journey. Understanding this condition is the first step toward empowerment and finding the best possible care.
Key Takeaways
Late-stage melanoma means the cancer has spread: This includes Stage III, where it has reached nearby lymph nodes or skin, and Stage IV, where it has spread to distant organs like the lungs, liver, or brain.
Advancements in treatment offer new hope: While late-stage melanoma is serious, major breakthroughs in immunotherapy and targeted therapy have significantly improved outcomes and survival rates in recent years.
Diagnosis involves comprehensive testing: Doctors use various imaging scans (PET, CT, MRI) and biopsies to determine the extent of the cancer and guide treatment decisions.
Treatment is personalized and multi-faceted: It often involves a combination of surgery, radiation, immunotherapy, targeted therapy, and participation in clinical trials, tailored to the individual's specific cancer.
Support and symptom management are crucial: Living with late-stage melanoma requires a focus on managing symptoms, emotional well-being, and building a strong support team, including healthcare professionals and loved ones.
Understanding Melanoma: A Quick Overview
Before diving deep into late-stage melanoma, let's briefly understand what melanoma is and why early detection is so important.
What is Melanoma?
Melanoma is a type of skin cancer that develops in the melanocytes, the cells responsible for producing melanin, the pigment that gives your skin, hair, and eyes their color. While it's less common than other skin cancers like basal cell or squamous cell carcinoma, it's considered the most serious because of its ability to spread quickly to other parts of the body if not caught early.
Melanoma can appear as a new mole, or it can develop from an existing mole that changes in size, shape, or color. It can occur anywhere on the body, even in areas not exposed to the sun, such as the soles of the feet, palms of the hands, under fingernails, or even in the eyes and internal organs (though these are rare).
Why is Early Detection Crucial?
The survival rate for melanoma is significantly higher when it's detected and treated in its early stages. When melanoma is thin and confined to the top layer of the skin (epidermis), it can often be completely removed with a simple surgical procedure. This is why regular skin self-exams and professional skin checks are so vital.
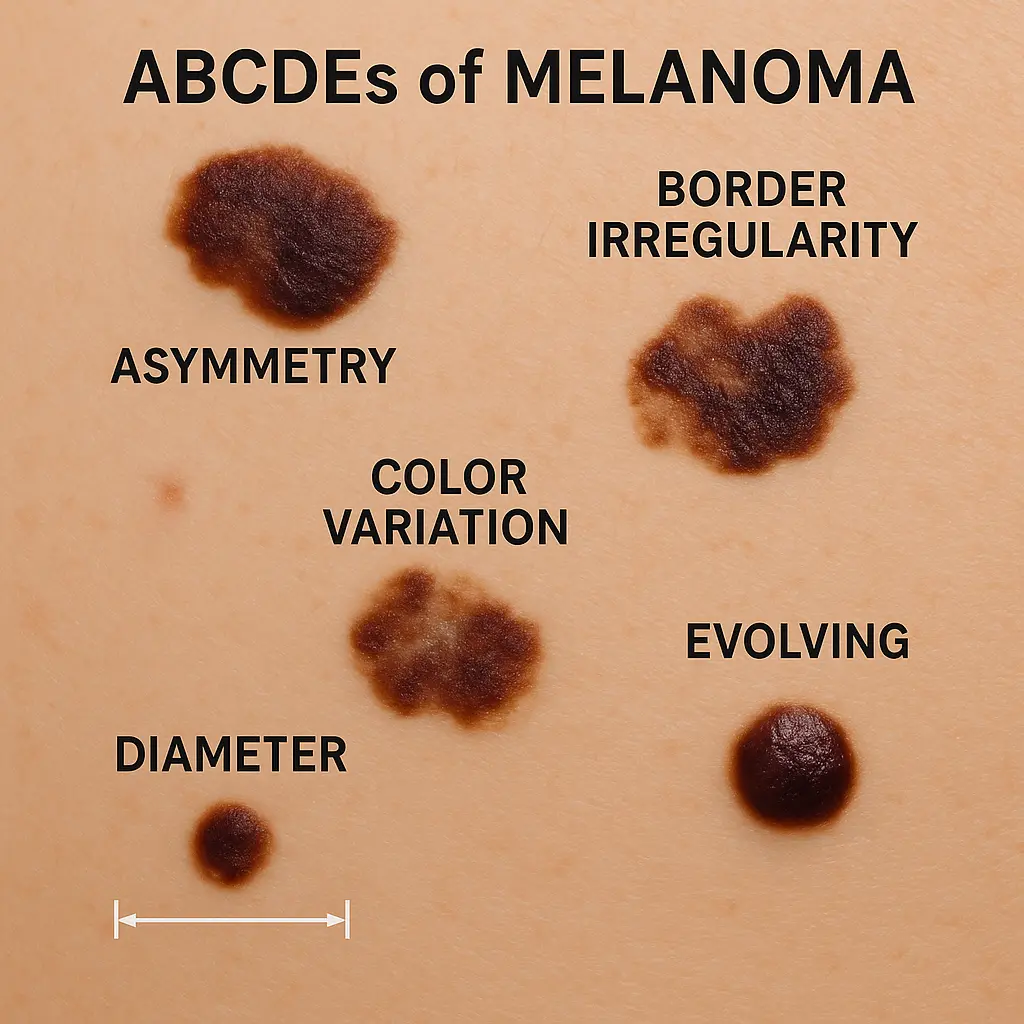
The "ABCDEs of Melanoma" are a helpful guide for identifying suspicious moles:
Asymmetry: One half of the mole doesn't match the other.
Border irregularity: The edges are ragged, notched, or blurred.
Color variation: The mole has different shades of brown, black, tan, or even red, white, or blue.
Diameter: The mole is larger than 6 millimeters (about the size of a pencil eraser), though melanomas can be smaller.
Evolving: The mole is changing in size, shape, color, or has new symptoms like itching, tenderness, or bleeding.
If you notice any of these changes, it's important to see a doctor right away. Early detection can make all the difference in treatment outcomes. For more information on skin conditions and general well-being, you can visit resources like https://www.theminorsurgerycenter.com/conditions.
The Staging of Melanoma: What Does it Mean?
When melanoma is diagnosed, doctors determine its "stage." Staging is a critical process that helps doctors understand how far the cancer has spread. This information is used to predict the likely course of the disease (prognosis) and to plan the most effective treatment.
The most widely used staging system for melanoma is the TNM system, developed by the American Joint Committee on Cancer (AJCC). TNM stands for:
T (Tumor): Describes the original (primary) tumor's thickness (Breslow depth), whether it's ulcerated (broken skin surface), and if it has spread to nearby skin or lymph vessels.
N (Nodes): Indicates whether the cancer has spread to nearby lymph nodes and, if so, how many lymph nodes are affected and the size of the spread.
M (Metastasis): Shows whether the cancer has spread to distant parts of the body (metastasis), such as other organs or distant skin sites.
Based on the TNM factors and other characteristics like mitotic rate (how fast cells are dividing) and LDH levels (a blood test that can indicate cancer spread), melanoma is assigned a stage from 0 to IV.
Stage 0 (Melanoma in Situ): The cancer cells are only in the very top layer of the skin (epidermis) and have not invaded deeper.
Stage I: The melanoma is thin (up to 2 mm thick) and has not spread to lymph nodes or distant sites. It may or may not be ulcerated.
Stage II: The melanoma is thicker (more than 2 mm thick) or has ulceration, but it has not spread to lymph nodes or distant sites.
While Stages 0, I, and II are considered early-stage, they still require careful treatment and follow-up. Our focus here is on the more advanced stages, where the cancer has spread beyond the primary tumor site.
Melanoma Late Stage: A Deep Dive into Stage III
Stage III melanoma is considered a late stage because the cancer has spread beyond the original tumor site to nearby areas. This means it's no longer just a localized skin problem.
Defining Stage III: Lymph Node Involvement and Beyond
In Stage III melanoma, the cancer has reached one or more of the following:
Nearby Lymph Nodes: This is the most common characteristic of Stage III. Lymph nodes are small, bean-shaped glands that are part of the body's immune system. They filter lymph fluid and trap foreign invaders, including cancer cells. If melanoma cells enter the lymphatic system, they can travel to and grow in nearby lymph nodes.
In-transit Metastases: These are small tumors that appear in the skin or under the skin (subcutaneous tissue) between the primary tumor site and the nearest group of lymph nodes. They are also sometimes called "satellite lesions" if they are very close to the primary tumor.
Microsatellites: These are small nests of melanoma cells found in the skin around the primary tumor but not connected to it. They are only visible under a microscope.
The involvement of lymph nodes or other regional spread indicates a higher risk of the cancer spreading further.
Subtypes of Stage III Melanoma
Stage III is further divided into sub-stages (IIIA, IIIB, IIIC, and IIID) based on the number of affected lymph nodes, whether the lymph nodes are enlarged enough to be felt (clinically detected) or only found under a microscope (microscopic), and the presence of ulceration, in-transit metastases, or satellite lesions. These sub-stages help doctors fine-tune prognosis and treatment plans. For instance, Stage IIID is the most advanced form of Stage III, indicating extensive regional spread.
Symptoms of Stage III Melanoma
While the primary tumor might still be the most noticeable symptom, Stage III melanoma can present with additional signs due to its spread:
Enlarged Lymph Nodes: You might feel a lump or swelling in the area of lymph nodes closest to the original melanoma (e.g., in the armpit if the melanoma was on the arm, or in the groin if it was on the leg). These lumps are often painless.
New Lumps or Bumps: The appearance of new, small, colored or skin-colored lumps in the skin or just under the skin near the original melanoma site (in-transit metastases or satellite lesions).
Changes in the Primary Tumor: The original melanoma might continue to change, grow, or become ulcerated (open sore).
It's important to note that sometimes, the only way to know if melanoma has spread to lymph nodes is through specific diagnostic tests, as the nodes may not be visibly enlarged.
Diagnosis for Stage III Melanoma
Diagnosing Stage III melanoma involves a combination of tests to confirm the spread and determine its extent:
Biopsy of the Primary Tumor: This is usually the first step to confirm melanoma. A small piece of the suspicious mole is removed and examined under a microscope.
Sentinel Lymph Node Biopsy (SLNB): If the primary melanoma is of a certain thickness (typically ≥0.8 mm), an SLNB is often recommended. This procedure involves injecting a blue dye or a radioactive substance near the melanoma. This substance travels to the first lymph node(s) that drain from the tumor area (the "sentinel" nodes). These nodes are then surgically removed and examined for cancer cells. If cancer cells are found, it confirms Stage III melanoma.
Lymph Node Dissection: If the sentinel lymph node biopsy is positive, or if cancer is found in other lymph nodes, a more extensive surgery called a complete lymph node dissection (CLND) may be performed to remove all or most of the lymph nodes in that area.
Imaging Scans: To check for spread to other parts of the body, doctors may order imaging tests like:
CT (Computed Tomography) Scan: Uses X-rays to create detailed cross-sectional images of organs and tissues.
PET (Positron Emission Tomography) Scan: Uses a special radioactive tracer to find areas of high metabolic activity, which can indicate cancer. Often combined with CT (PET-CT).
MRI (Magnetic Resonance Imaging) Scan: Uses powerful magnets and radio waves to create detailed images, especially useful for checking the brain and spinal cord.
Ultrasound: Can be used to examine lymph nodes for signs of enlargement or suspicious features.
These diagnostic steps are crucial for accurate staging and guiding treatment decisions. For general inquiries about clinic services and diagnostics, you may find information at https://www.theminorsurgerycenter.com/clinic.
Treatment Options for Stage III Melanoma
Treatment for Stage III melanoma is often multi-faceted and aims to remove visible cancer, reduce the risk of recurrence, and prevent further spread.
Surgery:
Wide Local Excision: The primary tumor and a margin of healthy tissue around it are removed.
Lymph Node Dissection: If cancer is found in the sentinel lymph nodes, a complete lymph node dissection may be performed to remove additional nearby lymph nodes. This can reduce the risk of regional recurrence.
Adjuvant Therapy (Treatment After Surgery): Even after successful surgery, microscopic melanoma cells might remain, increasing the risk of recurrence. Adjuvant therapies are given after surgery to kill these lingering cells and reduce the chance of the cancer coming back.
Immunotherapy: These drugs boost the body's own immune system to recognize and fight cancer cells.
PD-1 Inhibitors (e.g., nivolumab, pembrolizumab): These drugs block a protein called PD-1 on immune cells, essentially "releasing the brakes" on the immune system so it can attack cancer.
CTLA-4 Inhibitors (e.g., ipilimumab): These drugs block another protein, CTLA-4, which also helps activate the immune system against cancer.
Targeted Therapy: If the melanoma cells have specific genetic mutations (like the BRAF mutation, found in about half of all melanomas), targeted therapies can be very effective.
BRAF and MEK Inhibitors (e.g., dabrafenib/trametinib, vemurafenib/cobimetinib): These drugs specifically target the proteins produced by the mutated BRAF gene and the pathways they activate, blocking cancer growth.
Radiation Therapy: While not a primary treatment for melanoma, radiation may be used after surgery to the lymph node area, especially if many nodes were involved or if there's a high risk of recurrence. It uses high-energy rays to kill cancer cells.
The choice of adjuvant therapy depends on factors like the specific sub-stage of melanoma, the presence of genetic mutations, and the patient's overall health. This personalized approach is a hallmark of modern cancer care.
Melanoma Late Stage: Navigating Stage IV
Stage IV melanoma is the most advanced stage. It means the cancer has spread from the original site and nearby lymph nodes to distant parts of the body. This is also known as metastatic melanoma.
Defining Stage IV: Distant Metastasis
In Stage IV melanoma, cancer cells have traveled through the bloodstream or lymphatic system and formed new tumors (metastases) in organs far from the original melanoma site.
Common Sites of Metastasis
Melanoma can spread to almost any part of the body, but some sites are more common than others:
Lungs: Often one of the first organs to be affected.
Liver: Another common site for distant spread.
Brain: Melanoma has a tendency to spread to the brain, which can cause specific neurological symptoms.
Bones: Can cause pain and weaken bones.
Distant Skin/Subcutaneous Tissue: New melanoma lesions may appear on the skin or just under the skin far from the original tumor.
Other Organs: Less commonly, melanoma can spread to the gastrointestinal tract, heart, or other organs.
Symptoms of Stage IV Melanoma
The symptoms of Stage IV melanoma vary widely depending on where the cancer has spread. They can be general or specific to the affected organ:
General Symptoms:
Unexplained weight loss
Fatigue
Loss of appetite
Fever
Night sweats
Site-Specific Symptoms:
Lungs: Persistent cough, shortness of breath, chest pain.
Liver: Abdominal pain, jaundice (yellowing of skin or eyes), swelling in the legs or abdomen.
Brain: Headaches, seizures, changes in vision, speech, balance, or personality.
Bones: Bone pain, fractures.
Skin: New lumps or bumps on the skin that look like moles but are actually metastases.
It's crucial for patients to report any new or worsening symptoms to their medical team promptly.
Diagnosis for Stage IV Melanoma
Diagnosing Stage IV melanoma involves confirming the presence of distant metastases. This typically includes:
Comprehensive Imaging:
PET-CT Scan: This is often the preferred imaging test as it can identify cancer cells throughout the entire body.
MRI of the Brain: Essential for checking for brain metastases, even if no neurological symptoms are present, as melanoma commonly spreads to the brain.
CT Scans: May be used for specific areas like the chest, abdomen, or pelvis.
Biopsy of Metastatic Sites: If imaging shows suspicious areas, a biopsy of the new tumor (e.g., in the lung, liver, or a distant lymph node) is often performed to confirm it is melanoma. This also allows for genetic testing (e.g., for BRAF mutation) on the metastatic tissue, which can guide targeted therapy.
Blood Tests:
LDH (Lactate Dehydrogenase): Elevated LDH levels can sometimes indicate a higher tumor burden and are an important prognostic factor in Stage IV melanoma.
Other blood tests: To check general health, organ function, and potential side effects of treatments.
Treatment Options for Stage IV Melanoma
Treatment for Stage IV melanoma has undergone a revolution in recent years, offering significantly improved outcomes compared to a decade ago. The goal of treatment is typically to control the cancer's growth, manage symptoms, improve quality of life, and extend survival. Treatment plans are highly individualized.
Immunotherapy: These are now the cornerstone of treatment for many Stage IV melanoma patients. They harness the body's immune system to fight cancer.
PD-1 Inhibitors (e.g., pembrolizumab, nivolumab): These drugs are very effective and are often the first choice. They work by blocking a protein called PD-1 that cancer cells use to hide from the immune system.
CTLA-4 Inhibitors (e.g., ipilimumab): These drugs activate the immune system by blocking CTLA-4. Sometimes, PD-1 and CTLA-4 inhibitors are given together (combination immunotherapy) for a stronger immune response, though this can also increase side effects.
TIL (Tumor-Infiltrating Lymphocyte) Therapy: A type of adoptive cell therapy where immune cells (T-cells) are taken from a patient's tumor, grown in large numbers in the lab, and then infused back into the patient to fight the cancer. This is a more specialized treatment.
Oncolytic Virus Therapy (e.g., T-VEC): A modified virus (herpes simplex virus) is injected directly into melanoma tumors, where it replicates within the cancer cells, causing them to burst and die. It also stimulates an immune response against the cancer.
Targeted Therapy: If the melanoma cells have specific genetic mutations, targeted therapies can be very effective.
BRAF/MEK Inhibitors (e.g., dabrafenib/trametinib, encorafenib/binimetinib, vemurafenib/cobimetinib): These drugs are used for melanomas with a BRAF gene mutation (found in about 50% of cases). They block the activity of mutated proteins that drive cancer growth. These drugs can work very quickly to shrink tumors.
Chemotherapy: While once the main treatment for advanced melanoma, chemotherapy is now less commonly used due to the superior effectiveness of immunotherapy and targeted therapy. It may be considered for patients who don't respond to other treatments or in specific situations. Chemotherapy drugs work by killing rapidly dividing cells, including cancer cells, but they also affect healthy cells, leading to more side effects.
Radiation Therapy: Radiation uses high-energy beams to kill cancer cells. In Stage IV melanoma, it's primarily used for:
Pain Relief: To shrink tumors that are causing pain, especially in bones.
Brain Metastases: To control tumors in the brain and manage neurological symptoms. Stereotactic radiosurgery (SRS) is a precise form of radiation often used for brain metastases.
To treat specific sites: To shrink tumors that are causing problems in other organs.
Surgery: Even in Stage IV, surgery can play a role, particularly for:
Removing isolated metastases: If there are only a few tumors in distant sites (oligometastatic disease) and they can be safely removed, surgery might be an option.
Managing symptoms: To remove tumors causing pain, blockages, or other severe symptoms.
Debulking: Reducing the size of large tumors to alleviate pressure or improve function.
Clinical Trials: Participation in clinical trials offers access to new and experimental treatments that are not yet widely available. For many patients with late-stage melanoma, clinical trials represent a crucial option for innovative care. We will discuss this in more detail later.
The decision on which treatment approach to use is made by a multidisciplinary team of specialists, including oncologists, dermatologists, surgeons, radiation oncologists, and pathologists. They consider the specific characteristics of the melanoma, its location, the patient's overall health, and their preferences.
"The landscape of late-stage melanoma treatment has been completely transformed. What was once a dire diagnosis now often comes with significant hope, thanks to remarkable advancements in immunotherapy and targeted therapies."
Prognosis and Survival Rates for Late-Stage Melanoma
Understanding prognosis and survival rates can be challenging, as these are statistical averages and do not predict an individual's specific outcome. However, they provide a general idea of what to expect based on historical data.
Factors Influencing Prognosis
Several factors influence the prognosis for late-stage melanoma:
Stage at Diagnosis: Stage III has a better prognosis than Stage IV. Within Stage III, lower sub-stages (IIIA) generally have better outcomes than higher sub-stages (IIID).
Location of Metastases (for Stage IV): Melanoma that has spread to distant skin, subcutaneous tissue, or distant lymph nodes generally has a better prognosis than melanoma that has spread to internal organs like the lungs, liver, or brain. Spread to the brain is often associated with a less favorable prognosis.
Number of Metastases: Fewer metastatic sites generally lead to a better prognosis.
LDH Levels: Elevated levels of lactate dehydrogenase (LDH) in the blood are associated with a less favorable prognosis in Stage IV melanoma.
BRAF Mutation Status: Patients with BRAF mutations who are eligible for targeted therapy often have good initial responses.
Response to Treatment: How well the cancer responds to initial treatments is a major factor.
Overall Health and Performance Status: A patient's general health, ability to perform daily activities, and absence of other serious medical conditions can influence their ability to tolerate treatment and their overall outcome.
Age: Generally, younger patients tend to have better outcomes, though this can vary.
Survival Rates
Survival rates are typically reported as "5-year survival rates," which is the percentage of people who are still alive five years after their diagnosis. It's important to remember:
These are averages: They are based on large groups of people and cannot predict what will happen to any individual.
They reflect past data: Survival rates are based on diagnoses made years ago, and new treatments developed since then may have improved outcomes. This is particularly true for melanoma, where significant breakthroughs have occurred in the last decade.
General 5-Year Survival Rates for Melanoma (AJCC 8th Edition, based on diagnoses from 2010-2016):
Melanoma Stage5-Year Survival Rate (Approximate)Stage 099-100%Stage I93-97%Stage II70-85%Stage III32-78% (varies greatly by sub-stage)Stage IV15-30% (varies by site of metastasis)
Improvements in Survival Rates: The introduction of effective immunotherapies and targeted therapies, starting around 2011, has dramatically improved the outlook for patients with late-stage melanoma. While the statistics above reflect data from a period when these treatments were becoming more common, studies continue to show better survival rates in more recent cohorts. For example, some studies show 5-year survival rates for Stage IV melanoma now exceeding 50% for certain patient groups treated with modern therapies, a significant improvement from historical rates.
This means that while a late-stage diagnosis is serious, there is more hope than ever before. Many patients with Stage IV melanoma are living longer, with better quality of life, thanks to these groundbreaking treatments.
Managing Life with Late-Stage Melanoma
A diagnosis of late-stage melanoma affects not just the body but also the mind and spirit. Managing life with this condition involves comprehensive medical care, strong emotional support, and practical strategies to maintain quality of life.
Symptom Management and Palliative Care
Controlling symptoms is a central part of care for late-stage melanoma. This is where palliative care plays a vital role. Palliative care focuses on providing relief from the symptoms and stress of a serious illness, aiming to improve quality of life for both the patient and their family. It is not hospice care and can be provided alongside curative treatments.
A palliative care team can help with:
Pain management: Using medications and other therapies to control pain from tumors or treatment side effects.
Nausea and vomiting: Managing digestive issues.
Fatigue: Strategies to cope with extreme tiredness.
Shortness of breath: Addressing respiratory discomfort.
Anxiety and depression: Providing emotional support and resources.
Nutritional support: Helping with appetite loss or dietary needs.
Emotional and Psychological Support
Coping with a late-stage cancer diagnosis can be overwhelming. Feelings of fear, anxiety, sadness, and anger are common. It's important to seek support:
Counseling/Therapy: A therapist or counselor specializing in cancer can provide strategies for coping, help process emotions, and improve mental well-being.
Support Groups: Connecting with others who are going through similar experiences can reduce feelings of isolation and provide valuable insights and shared coping strategies. Many cancer centers offer these.
Family and Friends: Leaning on loved ones for emotional support and practical help is crucial.
Mindfulness and Relaxation Techniques: Practices like meditation, deep breathing, and yoga can help manage stress and improve mood.
Importance of a Multidisciplinary Team
Effective management of late-stage melanoma requires a team approach. Your care team may include:
Medical Oncologist: Specializes in cancer treatment using chemotherapy, immunotherapy, and targeted therapy.
Dermatologist: For skin checks and managing skin-related issues.
Surgical Oncologist: For removing tumors.
Radiation Oncologist: For radiation therapy.
Palliative Care Specialist: For symptom management and supportive care.
Pathologist: Analyzes biopsies and determines cancer characteristics.
Radiologist: Interprets imaging scans.
Oncology Nurse: Provides education, manages side effects, and coordinates care.
Social Worker/Patient Navigator: Helps with practical needs, financial concerns, and connecting to resources.
Dietitian: Provides nutritional guidance.
Psychologist/Counselor: Offers emotional support.
This team works together to create a comprehensive and personalized treatment plan.
Nutrition and Lifestyle
Maintaining good nutrition and a healthy lifestyle can support overall well-being during treatment:
Balanced Diet: Focus on nutrient-rich foods, including fruits, vegetables, lean proteins, and whole grains. Staying hydrated is also very important.
Gentle Exercise: If possible, light exercise like walking can help reduce fatigue, improve mood, and maintain strength. Always consult your doctor before starting any exercise program.
Adequate Rest: Prioritize sleep and allow for rest periods throughout the day.
Caregiver Support
The journey with late-stage melanoma also significantly impacts caregivers. They need support too. Resources for caregivers include:
Support groups for caregivers.
Respite care to allow caregivers to rest.
Counseling services.
It's vital for caregivers to look after their own physical and mental health to continue providing effective support.
The Role of Clinical Trials
Clinical trials are research studies that test new ways to prevent, detect, diagnose, or treat diseases. For patients with late-stage melanoma, clinical trials can be a very important option.
What are Clinical Trials?
Clinical trials are how doctors and scientists discover if new treatments are safe and effective. They are carefully designed and conducted under strict guidelines to protect the participants. There are different phases of clinical trials:
Phase I: Tests a new drug or treatment in a small group of people for the first time to evaluate its safety, determine a safe dosage range, and identify side effects.
Phase II: Evaluates the effectiveness of the new treatment and continues to assess its safety in a larger group of people.
Phase III: Compares the new treatment to the standard treatment to confirm its effectiveness, monitor side effects, and collect information that will allow the new treatment to be used safely.
Phase IV: Post-marketing studies conducted after a drug has been approved and marketed, to gather information on the drug's effect in various populations and any side effects associated with long-term use.
Why Consider Them?
For patients with late-stage melanoma, participating in a clinical trial offers several potential benefits:
Access to Cutting-Edge Treatments: You might receive a new treatment that is not yet available to the general public and could be more effective than standard therapies.
Close Monitoring: Participants are often monitored very closely by a dedicated research team, which can mean more frequent check-ups and detailed assessments.
Contributing to Medical Science: Your participation helps advance medical knowledge and can lead to new treatments that benefit future patients.
Hope: For some patients, clinical trials represent a pathway to continued treatment when standard options are exhausted or less effective.
How to Find Them
If you are considering a clinical trial, discuss it with your medical oncologist. They can help determine if you are eligible for any ongoing trials based on your specific diagnosis and health status. You can also search for trials through:
ClinicalTrials.gov: A comprehensive database of publicly and privately funded clinical studies conducted around the world.
Cancer Centers: Major cancer centers and academic hospitals often have many ongoing clinical trials.
Patient Advocacy Groups: Organizations focused on melanoma often list relevant clinical trials and provide resources.
It's important to understand the potential risks and benefits of any clinical trial before enrolling. Always ask your medical team detailed questions.
Prevention and Early Detection: The Ultimate Defense
While this article focuses on late-stage melanoma, it's impossible to overstate the importance of prevention and early detection. These are the ultimate defenses against the disease progressing to an advanced stage.
Skin Self-Exams
Regularly checking your own skin is a powerful tool for early detection. The American Academy of Dermatology recommends performing a skin self-exam monthly:
Know your skin: Become familiar with your moles, freckles, and other skin marks.
Use a full-length mirror and a hand mirror: To see all areas, including your back, scalp, buttocks, and genital area.
Pay attention to the "ugly duckling" rule: Look for any mole that stands out from the others on your skin.
Use the ABCDEs: Remember the criteria (Asymmetry, Border irregularity, Color variation, Diameter, Evolving) for identifying suspicious moles.
Document changes: Take photos of moles and measure them to track any changes over time.
Regular Dermatologist Visits
Even with diligent self-exams, it's crucial to have professional skin checks by a dermatologist, especially if you have risk factors for melanoma (e.g., many moles, fair skin, history of severe sunburns, family history of melanoma). A dermatologist has specialized training and tools (like a dermatoscope) to identify suspicious lesions that you might miss. They can also provide guidance on sun protection and mole monitoring. To learn more about professional care, you might explore resources like https://www.theminorsurgerycenter.com/faqs or consider reaching out for a consultation at https://www.theminorsurgerycenter.com/contact.
Sun Protection
Excessive exposure to ultraviolet (UV) radiation from the sun or tanning beds is the primary risk factor for melanoma. Protecting your skin from UV damage is essential:
Seek shade: Especially between 10 AM and 4 PM when the sun's rays are strongest.
Use broad-spectrum sunscreen: Apply generously to all exposed skin with an SPF of 30 or higher, and reapply every two hours, or more often if swimming or sweating.
Being proactive about your skin health is the best way to prevent melanoma from progressing to a late stage. If you notice any suspicious changes, don't delay in seeking medical advice. Early detection is key to successful treatment and better outcomes. For more general information on health and wellness, you can often find valuable articles on a https://www.theminorsurgerycenter.com/blog
Understanding Melanoma Stages
Stage III Melanoma: When it Spreads to Nearby Lymph Nodes
At Stage III, melanoma has grown deeper into the skin or has spread to nearby lymph nodes, or to small areas of skin around the main tumor (called satellite tumors or in-transit metastases) but has not yet reached distant organs.
Lymph Node Involvement: Cancer cells are found in one or more lymph nodes close to the original tumor.
In-transit Metastases: Small tumors appear between the primary tumor and the nearest lymph node basin.
No Distant Spread: The cancer has not spread to distant parts of the body like the lungs, liver, or brain.
Treatment for Stage III often involves surgery to remove the primary tumor and affected lymph nodes, followed by additional treatments like immunotherapy or targeted therapy to reduce the chance of the cancer coming back.
Stage IV Melanoma: When it Spreads to Distant Organs
Stage IV is the most advanced stage of melanoma. At this point, the cancer has spread from the original tumor site and nearby lymph nodes to distant parts of the body. This spread is called metastasis.
Distant Organs: Common places for melanoma to spread include the lungs, liver, brain, bones, or other areas of the skin far from the original site.
Systemic Symptoms: Patients might experience symptoms like fatigue, weight loss, or pain, depending on where the cancer has spread.
Treatment for Stage IV melanoma focuses on controlling the cancer's growth and managing symptoms. It often involves powerful systemic therapies like immunotherapy or targeted therapy, which have greatly improved outcomes in recent years. Surgery and radiation might also be used for specific areas.
The progress in melanoma treatment over the past decade has been nothing short of revolutionary. Researchers continue to push the boundaries, offering even more hope for the future.
Ongoing Research
Scientists are actively researching several areas:
Understanding Resistance: Why some melanomas become resistant to immunotherapy or targeted therapy is a major focus. Research aims to find ways to overcome this resistance.
New Drug Targets: Identifying new genetic mutations or pathways within melanoma cells that can be targeted by new drugs.
Combination Therapies: Exploring new combinations of existing drugs (immunotherapy + targeted therapy, immunotherapy + radiation, etc.) to enhance effectiveness and reduce side effects.
Vaccines: Developing therapeutic vaccines that can train the immune system to recognize and attack melanoma cells.
Personalized Medicine: Advancing the ability to tailor treatments even more precisely to an individual's unique cancer based on its genetic makeup.
New Therapies on the Horizon
Several promising new therapies are in various stages of clinical trials:
New Immunotherapy Agents: Next-generation immune checkpoint inhibitors that target different pathways.
Cellular Therapies: Beyond TIL therapy, other forms of cell therapy (like CAR T-cell therapy adapted for solid tumors) are being explored.
Epigenetic Therapies: Drugs that modify how genes are expressed in cancer cells without changing the DNA sequence itself.
Personalized Medicine
The future of melanoma treatment is increasingly moving towards highly personalized medicine. This involves:
Comprehensive Genomic Profiling: Analyzing the specific genetic mutations and characteristics of an individual's tumor to identify the most effective targeted therapies or predict response to immunotherapy.
Liquid Biopsies: Blood tests that can detect circulating tumor DNA, offering a less invasive way to monitor treatment response and detect recurrence.
AI and Big Data: Using artificial intelligence and vast datasets to identify patterns and predict which treatments will work best for which patients.
These advancements mean that patients diagnosed with late-stage melanoma today have more options and a brighter outlook than ever before. Continuous research and innovation are driving us closer to a future where melanoma, even at its most advanced stages, can be managed effectively, offering extended and improved quality of life. For information regarding our team and expertise, please visit https://www.theminorsurgerycenter.com/team.
Conclusion
A diagnosis of late-stage melanoma can be daunting, but it is not a death sentence. The scientific breakthroughs of the last decade, particularly in immunotherapy and targeted therapy, have revolutionized the treatment landscape, offering new hope and significantly improved outcomes for many patients.
Understanding the staging, diagnostic processes, and diverse treatment options available is the first step in navigating this journey. Equally important is the focus on comprehensive support, including symptom management, emotional well-being, and the invaluable role of a multidisciplinary care team.
While research continues to push the boundaries of what's possible, the power of early detection and prevention remains paramount. Regular skin self-exams and professional checks, combined with diligent sun protection, are the best tools we have to catch melanoma before it progresses to advanced stages.
For those facing late-stage melanoma, remember that you are not alone. There is a vast network of medical professionals, support groups, and ongoing research dedicated to improving lives and fighting this disease. Stay informed, stay proactive, and lean on your support system as you navigate this challenging, yet increasingly hopeful, path.
Meta Title: Late-Stage Melanoma: Understanding & Treatment Advances Meta Description: Explore late-stage melanoma (Stage III & IV), its symptoms, advanced diagnostic methods, and revolutionary treatments like immunotherapy and targeted therapy. Find hope and support.