Impetigo Pictures: A Visual Guide to Identification & Treatment in 2026
Uncertainty about skin conditions can be distressing, especially when dealing with children. When you notice unusual sores or rashes, a common first step is to search for "impetigo pictures" to understand what you might be facing. This comprehensive guide, updated for 2025, aims to provide clarity on impetigo, a highly contagious bacterial skin infection, by offering a detailed visual and descriptive overview. Understanding what impetigo looks like, its different forms, and how it progresses is crucial for early detection and effective management.
Key Takeaways
Impetigo is a contagious bacterial skin infection, primarily affecting children aged 2-10. It often begins in areas of minor skin trauma.
The hallmark sign is honey-colored or yellowish-gold crusts that form after fluid-filled blisters rupture and ooze.
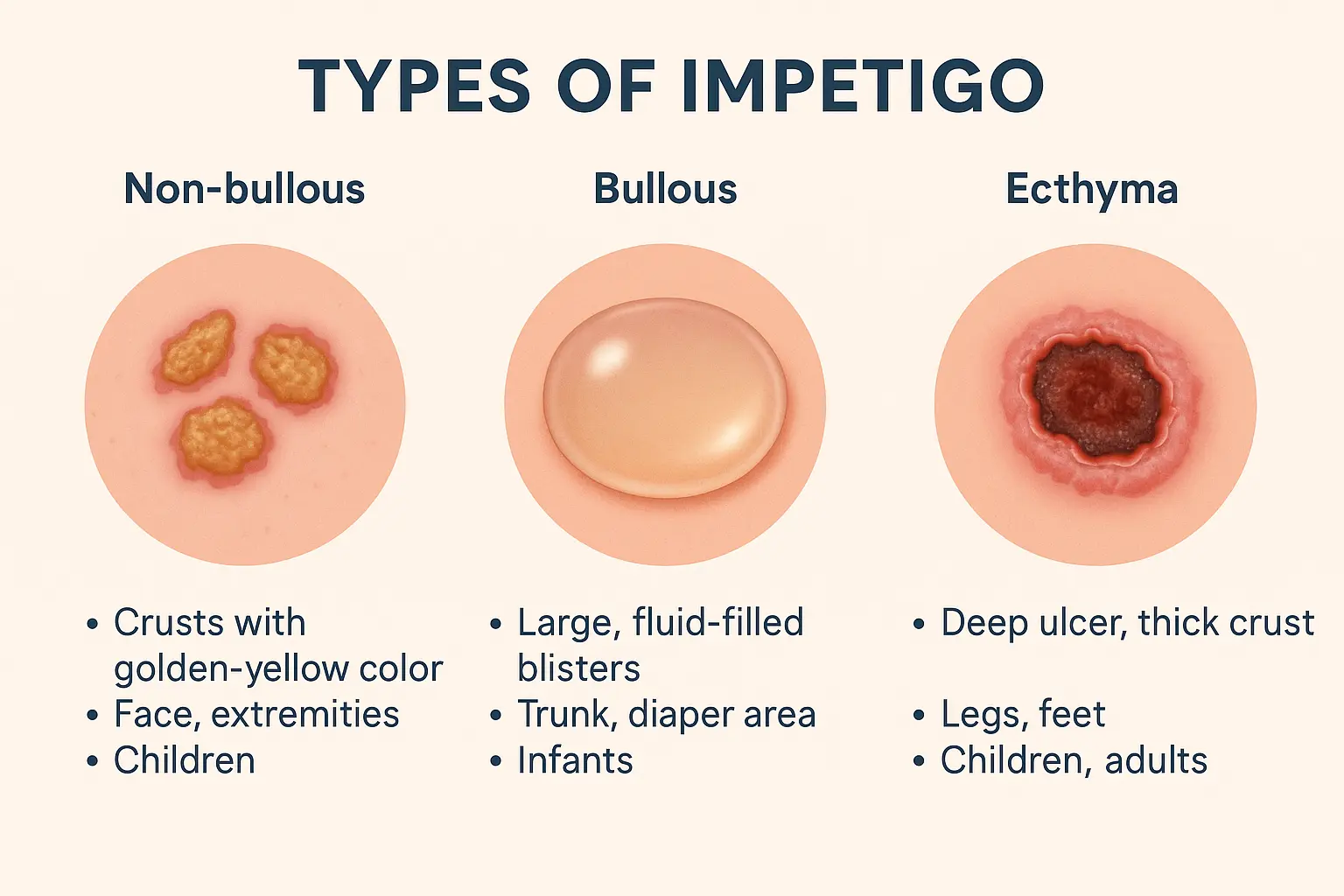
There are three main types: Non-bullous (most common, crusted sores), Bullous (large, fluid-filled blisters), and Ecthyma (deeper, ulcerating lesions that may scar).
Early identification through visual cues (impetigo pictures) is vital for prompt treatment and preventing spread to others.
Treatment typically involves antibiotics (topical or oral), and proper hygiene is crucial for preventing recurrence and transmission.
Understanding Impetigo: What the Pictures Show
Impetigo is a common superficial skin infection caused by Staphylococcus aureus or Streptococcus pyogenes bacteria [1]. While it can affect anyone, it is particularly prevalent among children between the ages of 2 and 10, often occurring in warmer months when outdoor activities and minor skin injuries are more frequent. The infection is highly contagious, spreading through direct contact with fluid from the sores or contaminated items.
The Appearance of Impetigo: Identifying Key Features
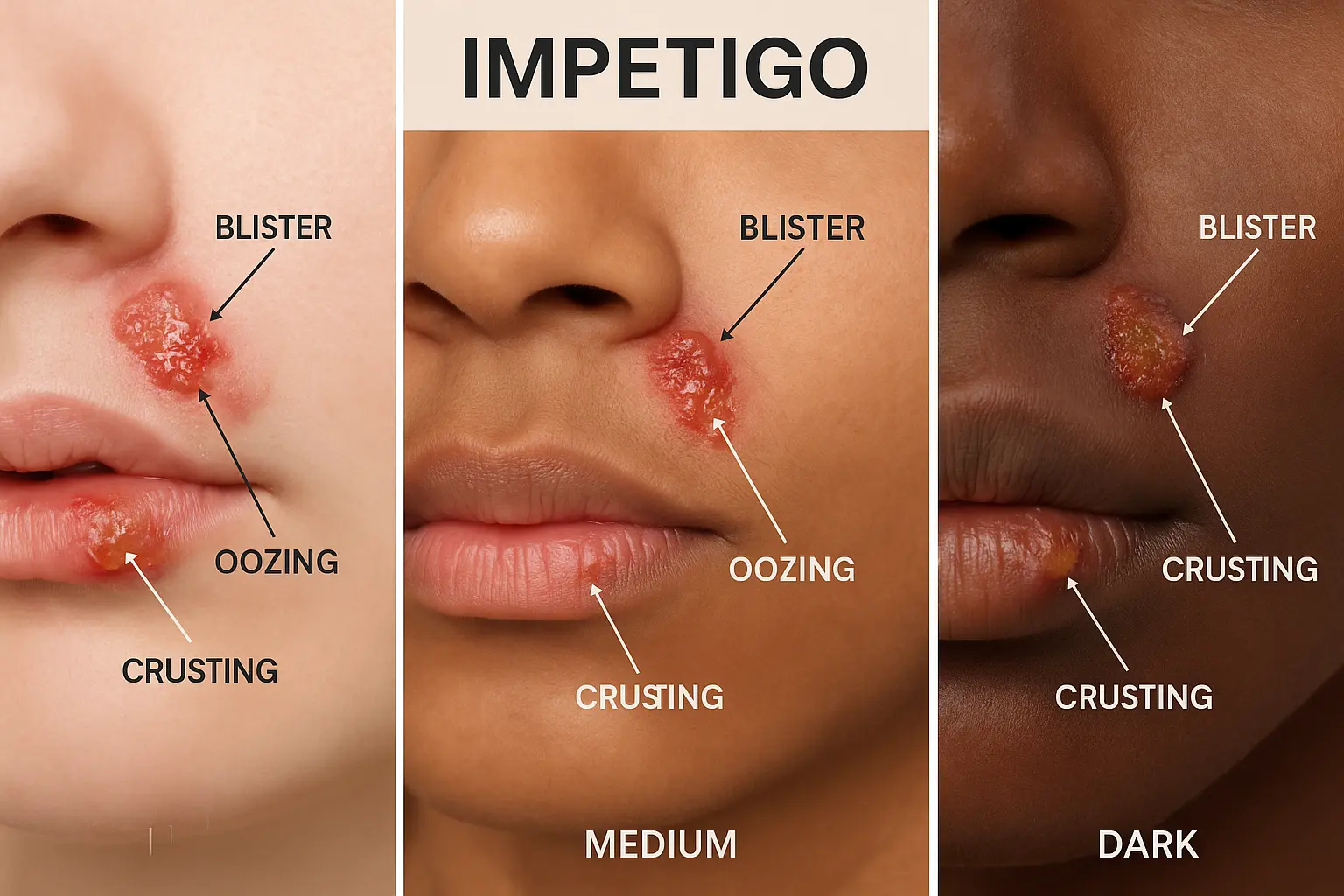
When viewing impetigo pictures, several characteristic features stand out. The infection typically starts as reddish sores. On lighter skin tones, these might appear pink or red, while on darker skin tones, they can manifest as dark red, purple, brown, or gray patches [2]. These initial sores are often clustered, especially around the nose and lips, but can also appear on hands, arms, legs, the scalp, and even the hairline.
Within a short period, often 1-3 days after bacterial exposure, these reddish bumps evolve into fluid-filled blisters. These blisters can range in size from a dime to a quarter and are quite fragile. They may burst within days, revealing moist, red skin underneath. It is at this stage that the most recognizable visual cue of impetigo emerges: the formation of honey-colored or yellowish-gold crusts [2]. These crusts are the result of the fluid from the ruptured blisters drying.
Visual Progression of Impetigo Lesions:
Reddish Bumps: Initial small, red spots, sometimes itchy.
Fluid-Filled Blisters: These bumps quickly develop into fragile, fluid-filled sacs.
Rupture and Oozing: The blisters burst, releasing fluid.
Honey-Colored Crusts: The hallmark sign, as the oozing fluid dries into distinctive golden-yellow scabs.
The sores are contagious as long as fluid is actively weeping from the blisters. Once they are fully scabbed over, or after 24 hours of starting antibiotic treatment, the risk of transmission significantly decreases [3].
Where Does Impetigo Usually Appear?
Impetigo has preferred sites of infection, largely due to common areas of minor skin trauma or contact.
Face: The most common location is around the nose and mouth, as these areas are frequently touched, scratched, or exposed to nasal secretions that may contain bacteria.
Hands and Arms: These areas are prone to cuts, scrapes, and insect bites, providing entry points for bacteria.
Legs: Similar to arms, legs can sustain minor injuries, especially in active children.
Scalp and Hairline: Scratches or existing skin conditions in these areas can also lead to impetigo.
Diaper Area: Particularly in infants and toddlers, the diaper area can develop impetigo, often due to moisture and friction.
It is important to note that impetigo often starts in areas where the skin barrier is already compromised, such as through small cuts, insect bites, eczema flare-ups, or scratches [4]. This makes proper wound care and management of underlying skin conditions vital in prevention.
"The distinctive honey-colored crusts are the most reliable visual indicator for identifying impetigo, a feature clearly showcased in most comprehensive impetigo pictures."
For more general information on various skin lesions and their appearances, exploring resources like the 25 Types of Skin Lesions Explained can be helpful in understanding the broader context of dermatological conditions.
Different Types of Impetigo: A Deeper Look Through Impetigo Pictures
While the term "impetigo" often brings to mind the classic honey-crusted sores, there are actually three distinct types, each with its own visual characteristics and severity. Understanding these differences through impetigo pictures is crucial for accurate diagnosis and appropriate treatment.
1. Non-Bullous Impetigo (Crusted Impetigo)
This is by far the most common form of impetigo, accounting for approximately 70% of all cases [5].
Visual Characteristics: Non-bullous impetigo typically begins as small, red sores or bumps, similar to insect bites or pimples. These lesions quickly progress into fluid-filled blisters that are quite fragile and rupture easily. Once ruptured, they ooze a clear or yellowish fluid, which then dries to form the characteristic honey-colored or yellowish-gold crusts. These crusts are usually firmly adherent and, when removed, reveal a red, moist, eroded area underneath. The sores typically range from dime to quarter size.
Location: Most commonly found on the face (especially around the nose and mouth), hands, and arms.
Symptoms: The lesions are often itchy, but usually not painful. Fever is uncommon.
Causative Agents: Primarily caused by Staphylococcus aureus, sometimes by Streptococcus pyogenes.
Who it Affects: Predominantly children.
Example of Non-Bullous Impetigo in Impetigo Pictures: Imagine a child's chin with several small, irregular patches of golden-brown crusts, almost as if honey has dried on the skin. The skin immediately surrounding these crusts might appear slightly reddened.
2. Bullous Impetigo
Bullous impetigo is less common than the non-bullous form but is characterized by more distinct, larger blisters.
Visual Characteristics: Unlike the small, easily ruptured blisters of non-bullous impetigo, bullous impetigo presents with larger, fluid-filled blisters (bullae) that are typically clear and transparent, then become cloudy. These blisters are usually more durable and may remain intact for a longer period before rupturing. When they do rupture, they leave behind raw, shallow erosions surrounded by a thin, varnish-like crust, which is often less thick and less "honey-colored" than in non-bullous impetigo. The blisters can be up to 1-2 cm in diameter.
Location: Often appears on the trunk, arms, legs, and the diaper area, particularly in infants and children under 2 years [6].
Symptoms: These blisters are usually painless, but can be itchy. Mild fever and general malaise can sometimes occur.
Causative Agents: Exclusively caused by certain strains of Staphylococcus aureus that produce a toxin that causes the skin to separate.
Who it Affects: Most commonly infants and young children, but can occur in adults, especially those with compromised immune systems.
Example of Bullous Impetigo in Impetigo Pictures: Picture an infant's arm with several raised, clear or slightly cloudy blisters ranging from pea-sized to grape-sized. Some may have already burst, leaving smooth, red, moist areas that are beginning to form a thin, shiny crust.
3. Ecthyma
Ecthyma is considered a more severe and deeper form of impetigo. It affects not just the superficial epidermis but extends into the dermis (deeper skin layer).
Visual Characteristics: Ecthyma lesions begin similar to impetigo but evolve into painful, large blisters that quickly break down. Instead of forming superficial crusts, these lesions develop into deep, punched-out ulcers with raised, hardened edges. The base of the ulcer is typically covered by a thick, dark brown or black crust. These lesions are significantly more painful than impetigo sores and heal slowly.
Location: Most commonly found on the legs and buttocks, often affecting areas previously injured.
Symptoms: Pain is a prominent feature, along with regional lymphadenopathy (swollen lymph nodes) and sometimes fever.
Causative Agents: Usually caused by Streptococcus pyogenes, but Staphylococcus aureus can also be involved.
Complications: Due to the deeper involvement, ecthyma can leave visible scars after healing [7].
Who it Affects: Can affect anyone, but is more common in individuals with poor hygiene, weakened immune systems, or those with neglected impetigo.
Example of Ecthyma in Impetigo Pictures: Visualize an adult's lower leg with a circular, eroded lesion about an inch in diameter. Its center is depressed and covered with a dark, thick scab, while the edges of the lesion are red, inflamed, and slightly raised. The surrounding skin might show signs of inflammation and tenderness.
FeatureNon-Bullous ImpetigoBullous ImpetigoEcthymaCommonalityMost common (70%)Less commonRarest, most severePrimary LesionSmall vesicles/pustules, rapidly crustingLarge, flaccid bullae (blisters)Vesicles/bullae evolving into deep ulcersCrust AppearanceThick, honey-colored, adherentThin, varnish-like, often less goldenThick, dark brown/black, hardDepth of InfectionEpidermis (superficial)Epidermis (superficial)Dermis (deep)PainUsually painless, may be itchyUsually painless, may be itchyPainfulScarring PotentialRareRareHighCommon LocationsFace (nose/mouth), hands, armsTrunk, limbs, diaper areaLegs, buttocksTypical Age GroupChildren 2-10 yearsInfants, young childrenAny age, often with predisposing factorsCausative BacteriaS. aureus, S. pyogenesS. aureusS. pyogenes, S. aureus
Recognizing these distinctions in impetigo pictures is the first step toward seeking appropriate medical advice. For any concerns about unusual skin lesions, especially those that are painful or spreading, a consultation with a healthcare professional is always recommended. Our clinic, for instance, offers specialized services for various skin concerns, and you can learn more about our approach at The Minor Surgery Center.
What Causes Impetigo and How Does It Spread?
Understanding the origins and transmission of impetigo is vital for both treatment and prevention. This section delves into the bacterial culprits, risk factors, and the highly contagious nature of this common skin infection, with insights that complement the visual understanding gained from impetigo pictures.
The Bacterial Culprits
Impetigo is primarily caused by two types of bacteria:
Staphylococcus aureus (Staph): This is the most common cause of impetigo, particularly bullous impetigo [8]. Staph bacteria are often found living harmlessly on the skin or in the nose of healthy individuals. However, if the skin barrier is broken, they can enter and cause infection.
Streptococcus pyogenes (Group A Strep): This bacterium is also a frequent cause, especially of non-bullous impetigo. It's the same bacterium responsible for strep throat.
In some cases, both types of bacteria can be involved in the infection.
How Does Impetigo Spread?
Impetigo is notoriously contagious, spreading easily from person to person through direct contact with the fluid from the impetigo sores.
Direct Contact: The most common mode of transmission is skin-to-skin contact with an infected person. If someone touches an impetigo lesion and then touches their own broken skin, the bacteria can transfer and initiate a new infection.
Contaminated Objects: Sharing personal items such as towels, bedding, clothing, toys, or razors can also spread the bacteria. For example, if a child with impetigo uses a towel and another child uses the same towel, the bacteria can be transferred.
Minor Skin Trauma: Impetigo often starts in areas where the skin's protective barrier has been compromised. This includes:
Cuts and Scrapes: Everyday injuries provide an entry point for bacteria.
Insect Bites: Mosquito bites, flea bites, or spider bites can break the skin, making it vulnerable.
Eczema and Dermatitis: Conditions that cause dry, itchy, or broken skin create ideal entry points for bacteria.
Scratches: Constant scratching, especially with unwashed hands, can introduce bacteria into the skin.
Other Skin Conditions: Conditions like chickenpox can also predispose individuals to impetigo.
Risk Factors for Impetigo
Certain factors increase the likelihood of developing impetigo:
Age: Children aged 2-10 years are most susceptible. Their immune systems are still developing, and they are more prone to minor injuries and close contact with other children.
Crowded Environments: Places like schools, daycare centers, and sports teams where people are in close proximity increase the risk of transmission.
Warm, Humid Climates: Impetigo incidence peaks in warmer months, as bacteria thrive in such conditions, and increased sweating can soften the skin.
Poor Hygiene: Infrequent hand washing or inadequate wound care can contribute to the spread and development of the infection.
Weakened Immune System: Individuals with compromised immune systems (e.g., due to illness like diabetes, HIV, or certain medications) are more vulnerable.
Pre-existing Skin Conditions: As mentioned, conditions like eczema, scabies, or even poison ivy can make the skin more susceptible to bacterial invasion.
Understanding these factors allows for better prevention strategies. For instance, knowing that minor skin trauma is a common entry point emphasizes the importance of promptly cleaning and covering cuts and scrapes.
The Incubation Period
Symptoms of impetigo typically appear within 1 to 3 days after bacterial exposure to the skin [9]. Once the initial lesions become visible, they tend to progress rapidly, evolving from small bumps to blisters and then crusts within about a week. The infected areas remain contagious while fluid is actively weeping from the blisters. The contagious period usually ends once the sores are fully scabbed over or after 24 hours of starting antibiotic treatment [3].
For more information on general skin health and conditions, our blog provides a wealth of resources.
Diagnosing Impetigo: Beyond Impetigo Pictures
While impetigo pictures are incredibly useful for initial recognition, a formal diagnosis by a healthcare professional is always necessary. This section discusses the diagnostic process, when to seek medical attention, and potential complications if impetigo is left untreated.
Clinical Diagnosis
In most cases, a doctor can diagnose impetigo simply by examining the characteristic appearance of the skin lesions. The presence of the distinctive honey-colored crusts is often sufficient for a clinical diagnosis. The doctor will inquire about:
Symptoms: When the sores appeared, how they have progressed, and if there's any pain or itching.
Exposure: Any recent contact with individuals who have similar sores.
Risk Factors: History of skin trauma, eczema, or time spent in crowded environments.
When Is Lab Testing Necessary?
While often not required, a doctor might recommend further testing in certain situations:
Unusual Presentation: If the lesions do not look typical of impetigo, or if they are extensive and severe.
Lack of Response to Treatment: If the infection doesn't improve after a course of antibiotics, a culture may be taken to identify the specific bacteria and determine its antibiotic sensitivity (which antibiotics will be most effective).
Recurrent Infections: For individuals who experience repeated bouts of impetigo, identifying the exact strain of bacteria can help tailor treatment and prevention strategies.
A bacterial culture involves gently swabbing the fluid from a blister or beneath a crust and sending it to a lab for analysis.
When to See a Doctor
It's important to consult a healthcare professional if you suspect impetigo, especially if:
You or your child develop new skin lesions that resemble impetigo.
The lesions are spreading rapidly or become more painful.
You or your child experience fever or swollen lymph nodes.
You have a weakened immune system or other underlying health conditions.
The sores do not improve after a few days of home care.
Early diagnosis and treatment are crucial to prevent the infection from worsening, spreading to others, and avoiding potential complications.
Potential Complications of Untreated Impetigo
While impetigo is generally a benign condition, neglecting treatment can lead to more serious issues:
Cellulitis: This is a deeper and more serious bacterial infection of the skin and underlying tissues. It can cause red, swollen, warm, and painful skin, and may require intravenous antibiotics.
Ecthyma: As discussed earlier, untreated impetigo, especially if left to worsen or in individuals with compromised immunity, can progress to ecthyma, leaving scars.
Post-streptococcal Glomerulonephritis (PSGN): This is a rare but serious kidney complication that can occur after impetigo caused by Streptococcus pyogenes. It affects the kidneys' filtering units and can lead to symptoms like dark urine, swelling, and high blood pressure. This complication is more common in children and usually occurs several weeks after the skin infection.
Scarring: While uncommon with non-bullous and bullous impetigo, ecthyma can definitely leave visible scars.
Spread of Infection: Untreated impetigo continues to be highly contagious, potentially spreading to other family members, classmates, or teammates.
Therefore, prompt medical attention is paramount. A visit to a clinic specializing in minor surgeries and skin conditions, such as The Minor Surgery Center, can ensure a timely and accurate diagnosis, and lead to an effective treatment plan.
Treatment Options for Impetigo in 2025
Effective management of impetigo typically involves antibiotics and diligent hygiene practices. The goal of treatment is to clear the infection, prevent its spread, and minimize the risk of complications.
Topical Antibiotics
For mild cases of impetigo, especially non-bullous impetigo with localized lesions, topical antibiotic creams or ointments are often the first line of treatment.
Mupirocin (Bactroban): This is a widely prescribed topical antibiotic that is very effective against the bacteria that cause impetigo. It's usually applied directly to the sores 2-3 times a day for 5-7 days.
Retapamulin (Altabax): Another effective topical antibiotic.
Fusidic Acid (Fucidin): Commonly used in some regions.
How to Apply Topical Antibiotics:
Gently Clean the Area: Before applying, gently wash the affected skin with soap and water to remove crusts and debris. This helps the antibiotic penetrate better.
Apply Thin Layer: Dab a thin layer of the cream or ointment over the sores.
Cover (Optional): Your doctor might recommend covering the treated area with a gauze dressing to prevent scratching and further spread.
Wash Hands: Always wash your hands thoroughly before and after applying the medication.
Topical antibiotics are generally well-tolerated with few side effects. The sores often start to heal within a few days of consistent application.
Oral Antibiotics
Oral antibiotics are typically prescribed for:
More widespread or severe cases of impetigo.
Bullous impetigo.
Ecthyma (due to its deeper nature).
If topical antibiotics are not effective.
When there's a risk of complications, such as post-streptococcal glomerulonephritis.
Common oral antibiotics include:
Cephalexin (Keflex): A common choice, usually taken for 7-10 days.
Dicloxacillin: Another effective option.
Clindamycin: Used if there is a concern for methicillin-resistant Staphylococcus aureus (MRSA) or if the patient is allergic to penicillin.
Azithromycin or Clarithromycin: May be used for penicillin-allergic patients or certain bacterial strains.
It is crucial to complete the entire course of oral antibiotics, even if the sores appear to be healing. Stopping early can lead to a recurrence of the infection or antibiotic resistance.
Important Note: Antibiotics, whether topical or oral, should only be used under the guidance of a healthcare professional. Self-medication is not advised.
General Care and Hygiene
Alongside antibiotics, meticulous hygiene plays a critical role in managing impetigo and preventing its spread and recurrence.
Hand Washing: Frequent and thorough hand washing with soap and water is essential for both the infected individual and their caregivers.
Keep Sores Clean: Gently wash the affected areas with mild soap and water daily. This helps remove crusts and prevents bacterial buildup.
Trim Fingernails: Keep fingernails short to prevent scratching, which can worsen lesions and spread bacteria.
Cover Sores: Keep impetigo sores covered with gauze or bandages, especially during the day, to prevent scratching and transmission.
Avoid Sharing Personal Items: Do not share towels, washcloths, clothing, bedding, or toys with others.
Separate Laundry: Wash infected individuals' clothes, towels, and bedding separately in hot water.
Disinfect Surfaces: Regularly clean and disinfect surfaces and toys that might have come into contact with the sores.
Stay Home from School/Daycare: Children with impetigo should stay home until the sores are no longer contagious (typically 24 hours after starting antibiotics or once fully crusted over) to prevent outbreaks.
When to Consider Other Treatments or Referrals
In rare cases where impetigo is recurrent or severe, or if underlying conditions are suspected, a doctor might consider:
Nasal Swabs: If a patient experiences recurrent impetigo, a nasal swab may be taken to check for Staphylococcus aureus colonization in the nose. If positive, a topical antibiotic might be prescribed for nasal application to reduce recurrence.
Dermatology Referral: For persistent, unusual, or severe cases, a referral to a dermatologist might be recommended.
Treatment of Underlying Conditions: If impetigo is secondary to conditions like eczema or scabies, treating these primary conditions is crucial for long-term management.
For specific dermatological concerns or if you're looking for specialized care for skin conditions, understanding your options for clinics and specialists is important. For example, learning about the best skin cancer clinic in your area can be helpful for various skin health needs beyond impetigo.
Preventing Impetigo: Strategies for 2025
Preventing impetigo is largely about good hygiene, prompt wound care, and managing risk factors. Given its highly contagious nature, proactive measures are essential, especially in households with children.
1. Excellent Hygiene Practices
The cornerstone of impetigo prevention lies in consistent and thorough hygiene.
Frequent Hand Washing: Emphasize washing hands frequently with soap and water for at least 20 seconds, especially after playing outdoors, before eating, and after using the restroom. This is crucial for everyone in the household.
Regular Bathing/Showering: Daily bathing or showering helps keep the skin clean and reduces the bacterial load. Use a mild soap that doesn't excessively dry out the skin.
Nail Care: Keep fingernails trimmed short and clean. This minimizes the risk of bacteria accumulating under the nails and reduces skin damage from scratching.
2. Prompt and Proper Wound Care
Since impetigo often exploits breaks in the skin, proper care for minor injuries is paramount.
Clean Cuts and Scrapes: Immediately clean any cuts, scrapes, insect bites, or other skin injuries with soap and water.
Apply Antiseptic: Consider applying an over-the-counter antiseptic ointment (e.g., bacitracin or petroleum jelly) to minor wounds, and cover them with a bandage to protect against dirt and bacteria.
Manage Existing Skin Conditions: For individuals with conditions like eczema, ensure they are actively managed to keep the skin barrier intact. Moisturize regularly and follow treatment plans for flare-ups to prevent cracks and irritation that could serve as entry points for bacteria.
3. Avoiding the Spread
Once impetigo is present in a household or community, preventing its spread is critical.
Do Not Share Personal Items: Strictly avoid sharing towels, washcloths, razors, clothing, combs, or any other personal items. Each person should have their own.
Separate Laundry: If someone has impetigo, wash their bedding, towels, and clothing separately in hot water with detergent.
Cover Sores: Ensure impetigo sores are covered with loose clothing or gauze bandages to prevent contact with others and to deter scratching.
Stay Home When Contagious: Children with impetigo should not attend school or daycare until cleared by a doctor, typically 24 hours after starting antibiotic treatment or when the sores have crusted over and are no longer oozing.
Disinfect Surfaces: Regularly clean and disinfect frequently touched surfaces and toys, especially in shared environments.
4. Environmental Considerations
While not always controllable, some environmental factors can be managed.
Maintain Cleanliness in Shared Spaces: In schools, daycares, and gyms, emphasize good hygiene practices and regular cleaning of equipment and surfaces.
Avoid Overcrowding: Where possible, reduce overcrowding, which can facilitate easier bacterial transmission.
By diligently implementing these preventive strategies in 2025, individuals and communities can significantly reduce the incidence and spread of impetigo. Education, combined with visual aids like impetigo pictures, plays a crucial role in raising awareness and promoting early action.
For more information on preventing skin infections and maintaining overall skin health, exploring resources on topics such as Building a Skin-Healthy Lifestyle can provide valuable insights.
When Impetigo Mimics Other Conditions: Differentiating Through Impetigo Pictures
Sometimes, other skin conditions can look similar to impetigo, making self-diagnosis challenging even with reference to impetigo pictures. It's crucial to understand these distinctions because treatment for other conditions can be very different. Here's a brief overview of conditions that might be mistaken for impetigo:
1. Herpes Simplex (Cold Sores or Fever Blisters)
Similarities to Impetigo: Cold sores also appear as small, fluid-filled blisters, often around the mouth and nose, which can crust over.
Key Differences:
Blisters: Herpes blisters are typically grouped together on a red base and often feel tingly or itchy before they appear.
Crust: While cold sores crust over, the crust is usually thinner and less honey-colored than impetigo.
Recurrence: Herpes is a viral infection that recurs in the same location, often triggered by stress, fever, or sun exposure. Impetigo is bacterial and typically doesn't recur in the exact same spot without new bacterial exposure or skin trauma.
Pain: Cold sores are often quite painful and tender.
2. Contact Dermatitis
Similarities to Impetigo: An allergic reaction or irritation from contact dermatitis can cause red, itchy rashes, sometimes with small blisters that can weep and crust.
Key Differences:
Cause: Contact dermatitis is an inflammatory reaction to an irritant or allergen (e.g., poison ivy, nickel, certain cosmetics). Impetigo is bacterial.
Distribution: Rashes often appear in the exact pattern of contact with the offending substance.
Crust: The crusts are typically not the characteristic honey-colored type seen in impetigo.
Contagion: Not contagious.
3. Fungal Infections (e.g., Ringworm)
Similarities to Impetigo: Ringworm (tinea corporis) can cause red, itchy patches on the skin, sometimes with raised borders.
Key Differences:
Appearance: Ringworm often has a characteristic ring shape with a clearer center and scaly edges. Impetigo rarely presents in this pattern.
Crust: While scaling can occur, the thick, honey-colored crusts of impetigo are absent.
Cause: Fungal, not bacterial.
Contagion: Contagious, but through fungal spores.
4. Scabies
Similarities to Impetigo: Intense itching from scabies can lead to scratching, which can then cause secondary bacterial infections that may resemble impetigo.
Key Differences:
Primary Lesions: Scabies involves tiny burrows (tunnel-like lesions) and small, very itchy bumps, especially between fingers, on wrists, armpits, and genitals.
Symptoms: Extreme itching, often worse at night.
Cause: Mites, not bacteria.
5. Insect Bites
Similarities to Impetigo: Multiple insect bites (e.g., mosquito or flea bites) can cause red, itchy bumps. If scratched, these can become secondarily infected with bacteria, leading to lesions that look like impetigo.
Key Differences:
Initial Lesions: Clearly identifiable as insect bites (pustules or papules from the bite itself).
History: A clear history of insect exposure.
Progression: The impetigo-like appearance is a secondary infection, not the primary cause.
The Importance of Professional Assessment
Given these similarities, relying solely on impetigo pictures for diagnosis can be misleading. A healthcare professional, such as a family doctor or a dermatologist, has the expertise to differentiate between these conditions. They can take a thorough medical history, perform a physical examination, and, if necessary, conduct diagnostic tests (like a skin scraping for fungi or a bacterial culture) to confirm the diagnosis and ensure the correct treatment plan is initiated.
Attempting to treat a misdiagnosed condition can delay appropriate care, prolong suffering, and potentially lead to complications. When in doubt, always seek professional medical advice. For general skin health concerns or when dealing with unusual skin growths, understanding where to find specialized care, such as a best private dermatologist near me Ontario, can be incredibly beneficial.
Living with and Managing Impetigo in the Family
Impetigo is a common childhood infection, and while it can be concerning, it's highly treatable. Managing impetigo within a family setting requires diligence, patience, and clear communication to minimize disruption and prevent spread.
Managing a Child with Impetigo
Reassurance: Impetigo can look unpleasant, but reassure your child that it's a common condition and will clear up with treatment.
Adherence to Treatment: Strictly follow the doctor's instructions for antibiotic application or administration. Complete the full course of oral antibiotics, even if symptoms improve, to ensure the infection is fully eradicated and to prevent resistance.
Prevent Scratching: Keep your child's nails short. Consider putting mittens on infants or young children at night to prevent unconscious scratching. Scratching can spread the infection to other body parts or other individuals.
Explain Contagiousness: For older children, explain in simple terms why they need to wash their hands frequently and avoid sharing items.
School/Daycare Policy: Be aware of your school or daycare's policy on impetigo. Most require children to stay home until 24 hours after starting antibiotics or until lesions are dry and crusted.
Protecting Other Family Members
Isolation of Items: Designate separate towels, washcloths, and bedding for the infected family member. Wash these items separately in hot water.
Frequent Cleaning: Regularly clean and disinfect surfaces, especially in bathrooms and common areas. Pay attention to toys and objects that the infected person may have touched.
Hand Sanitizer: Encourage the use of alcohol-based hand sanitizer if soap and water are not immediately available, though soap and water are preferred for removing bacteria.
Avoid Close Contact: While difficult, try to minimize skin-to-skin contact with the infected person, especially when the sores are weeping.
Preventing Recurrence
While one episode of impetigo does not guarantee future infections, some individuals are more prone to recurrence.
Continued Good Hygiene: Maintain excellent hygiene practices even after the infection has cleared.
Monitor Skin: Be vigilant for any new cuts, scrapes, or insect bites, and clean them promptly.
Address Underlying Conditions: If your child has eczema or another chronic skin condition, ensure it is well-managed, as these can make the skin more susceptible to impetigo.
Nasal Carrier State: In cases of frequent recurrence, a doctor might test for Staphylococcus aureus colonization in the nose. If positive, a topical antibiotic ointment might be prescribed for nasal application to reduce the bacterial reservoir.
The Psychological Impact
While primarily a physical condition, impetigo can have a minor psychological impact, particularly on children. The visible sores can lead to feelings of self-consciousness, embarrassment, or anxiety about being different. Parents should:
Offer Emotional Support: Reassure your child and validate their feelings.
Educate Others: Inform school staff or close family members about the condition and its treatment, emphasizing that it's temporary and treatable.
Focus on Healing: Shift the focus from the appearance of the sores to the process of healing and recovery.
By taking a holistic approach that combines medical treatment with rigorous hygiene and empathetic support, families can effectively navigate an impetigo infection and minimize its impact. Always remember that for any persistent or concerning skin lesions, seeking professional medical advice is the most responsible course of action. For diverse dermatological needs, exploring clinics that offer services like mole, cyst, and skin tag removal can be beneficial for ongoing skin health.
Conclusion
Impetigo, while a common and highly contagious bacterial skin infection, is entirely manageable with prompt identification and appropriate treatment. This detailed guide, complete with descriptive insights on what to look for in impetigo pictures, aims to empower individuals and families with the knowledge needed to recognize the condition early. From the characteristic honey-colored crusts of non-bullous impetigo to the larger blisters of bullous impetigo and the deeper, ulcerating lesions of ecthyma, visual recognition is the first critical step.
Understanding the bacterial causes, common risk factors like minor skin trauma and crowded environments, and the rapid progression of lesions is essential for both prevention and effective management. While impetigo pictures provide invaluable clues, a professional medical diagnosis is paramount to ensure the correct course of action, differentiate it from other conditions, and prevent potential complications such as cellulitis or, rarely, kidney issues.
Treatment typically involves topical or oral antibiotics, coupled with stringent hygiene practices such as frequent hand washing, keeping sores clean and covered, and avoiding the sharing of personal items. These measures are not only crucial for clearing the infection but also for preventing its spread to others and minimizing the risk of recurrence.
In 2025, armed with this comprehensive knowledge, you can approach suspected cases of impetigo with confidence and clarity. Early action protects not only the affected individual but also the wider community.
Actionable Next Steps:
Observe Closely: If you notice any suspicious red sores or blisters, especially with honey-colored crusts, refer back to the impetigo pictures and descriptions in this guide.
Seek Medical Advice: Do not hesitate to consult a healthcare professional, such as your family doctor or a dermatologist, for a definitive diagnosis and treatment plan. Early intervention is key.
Implement Hygiene Protocols: If diagnosed, immediately begin strict hygiene practices for yourself and your family: wash hands frequently, keep sores clean and covered, and avoid sharing personal items.
Complete Treatment: Adhere to the full course of prescribed antibiotics, even if symptoms improve quickly, to ensure complete eradication of the bacteria.
Preventive Measures: Continue practicing good hygiene, prompt wound care, and managing any underlying skin conditions to reduce the risk of future infections.
For further information on various dermatological concerns or to book a consultation, please visit The Minor Surgery Center.
.webp)
.webp)

.webp)



