Dermatofibroma vs Neurofibroma: A Comprehensive Guide to Understanding These Skin Growths
When you discover a small bump or nodule on your skin, it's natural to feel concerned. Two common benign skin growths that often cause confusion are dermatofibroma and neurofibroma. While both present as skin nodules, understanding the differences between dermatofibroma vs neurofibroma is crucial for proper diagnosis, treatment, and peace of mind. These distinct conditions arise from different cell types, have unique characteristics, and require different approaches to management. This comprehensive guide will help you understand everything you need to know about these two skin conditions.
Key Takeaways
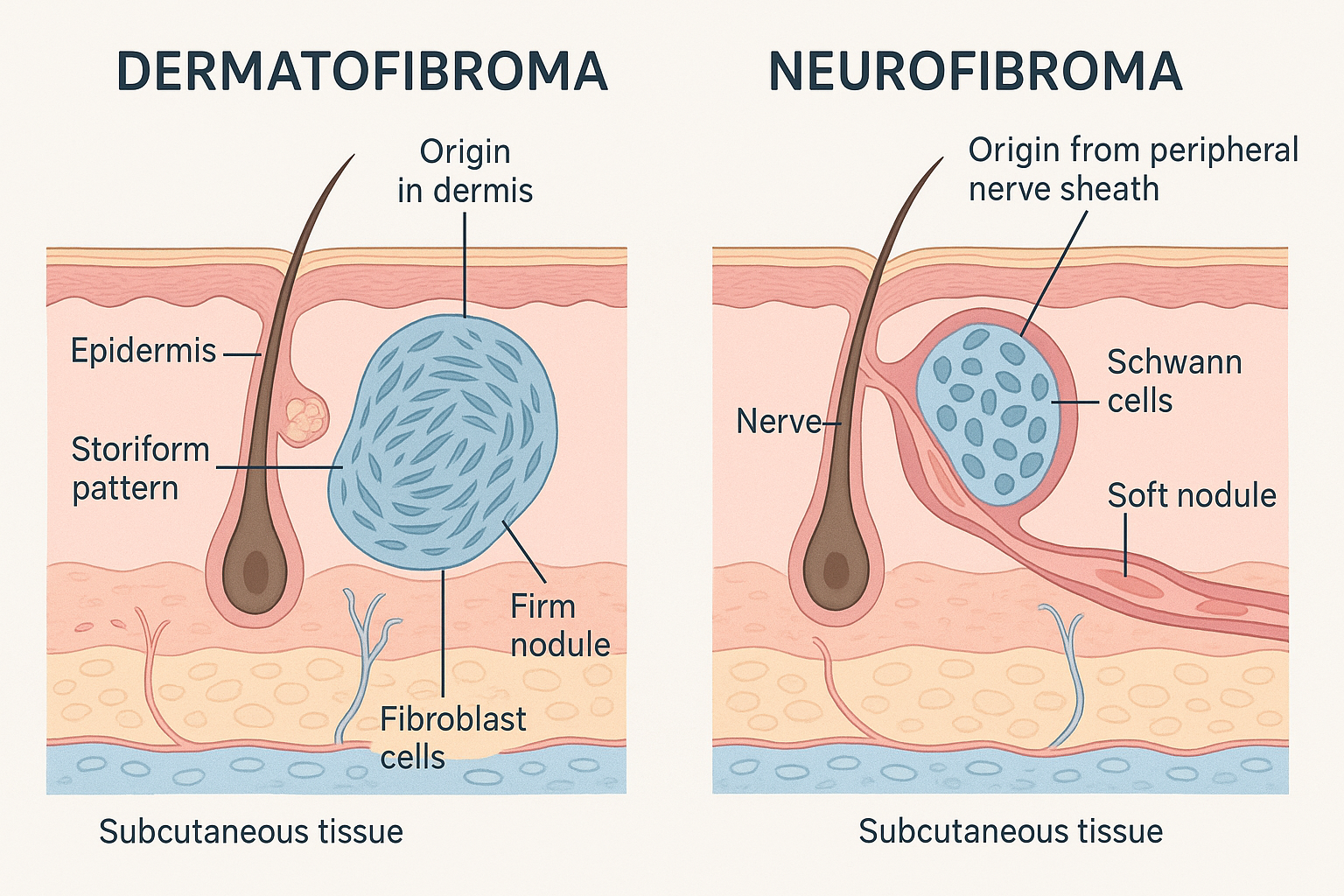
🔬 Different Origins: Dermatofibromas originate from fibroblasts in the skin's dermis layer, while neurofibromas arise from peripheral nerve sheaths
👆 Distinct Texture: Dermatofibromas feel firm and fixed on palpation, whereas neurofibromas are soft and compressible with a characteristic "buttonhole sign"
📍 Location Patterns: Dermatofibromas commonly appear on lower legs, while neurofibromas typically develop on the trunk, head, neck, and extremities
⚠️ Malignancy Risk: Both are generally benign, but plexiform neurofibromas carry increased transformation risk, while dermatofibromas rarely become malignant
🔍 Diagnosis Matters: Proper clinical examination, dermoscopy, and sometimes biopsy are essential for accurate differentiation and appropriate management
Understanding Dermatofibroma: The Firm Skin Nodule
What Is a Dermatofibroma?
A dermatofibroma is a common benign fibrous nodule that develops within the dermis layer of the skin. These growths consist primarily of spindle-shaped fibroblasts and histiocytoid cells arranged in a distinctive storiform (pinwheel-like) pattern [1]. Dermatofibromas are among the most frequently encountered skin lesions in dermatology practices, affecting people of all ages, though they're most common in adults between 20 and 45 years old.
The exact cause of dermatofibromas remains unclear, but current evidence suggests they may result from reactive fibroblast proliferation following minor trauma, insect bites, or local inflammation [2]. Some researchers propose they may have a heterogeneous origin, meaning different dermatofibromas might develop through various mechanisms.
Clinical Characteristics of Dermatofibroma
Dermatofibromas present with several distinctive features that help distinguish them from other skin growths:
Appearance and Color
Firm, raised nodules typically brown to skin-colored
May appear pink, red, or even black in some cases
Usually measure 0.5 to 1.5 cm in diameter
Have moderately defined borders with a slightly spiculated appearance
Texture and Feel
Firm and fixed to underlying tissue
Non-tender unless irritated or traumatized
Exhibit the characteristic "dimple sign" or "pinch sign" when squeezed from the sides (the center dimples inward)
Common Locations
Lower legs are the most frequent site (especially in women)
Can also occur on arms, trunk, and other body areas
Usually solitary, though multiple lesions can occur
Types and Variants of Dermatofibroma
Several histological variants of dermatofibroma exist, each with slightly different characteristics:
Variant TypeKey FeaturesClinical SignificanceCommon DermatofibromaStandard presentation, storiform patternMost frequent type, excellent prognosisCellular DermatofibromaIncreased cellularity, deeper extension25% local recurrence rate after excision [3]Aneurysmal DermatofibromaBlood-filled spaces, may appear darkerCan mimic vascular lesionsAtypical DermatofibromaNuclear atypia, increased mitosesRequires complete excision, rare progressionLipidized DermatofibromaContains lipid-laden cellsBenign variant, no special concerns
Understanding Neurofibroma: The Nerve Sheath Growth
What Is a Neurofibroma?
A neurofibroma is a benign peripheral nerve sheath tumor that originates from the endoneurium and supporting structures of peripheral nerves [4]. Unlike dermatofibromas, neurofibromas are comprised of multiple cell types including Schwann cells, fibroblasts, perineural cells, and mast cells. These tumors can occur sporadically or as part of neurofibromatosis type 1 (NF1), a genetic disorder.
Neurofibromas are caused by mutations in the NF1 gene located on chromosome 17. These mutations can be either:
Germline mutations: Inherited and present in all body cells (associated with NF1 syndrome)
Sporadic mutations: Occurring randomly in specific cells, leading to isolated neurofibromas
Clinical Types of Neurofibroma
Neurofibromas are classified into several distinct types based on their growth pattern and extent:
Localized Neurofibroma
The most common type, presenting as:
Soft, skin-colored to violaceous papules or subcutaneous nodules
Typically less than 2 cm in diameter
Exhibit the pathognomonic "buttonhole sign" – when pressed, the lesion invaginates into the underlying tissue like pushing a button through a buttonhole [5]
Can occur anywhere on the body, with predilection for trunk, head, neck, and extremities
Diffuse Neurofibroma
A less common variant characterized by:
Plaque-like thickening of skin
Predilection for head and neck region
May cause disfigurement when large
Infiltrates multiple tissue layers
Plexiform Neurofibroma
The most concerning type, featuring:
Involvement of multiple nerve fascicles
Characteristic "bag of worms" feel on palpation
Often present at birth or early childhood
May have overlying hyperpigmentation
Increased risk of malignant transformation to malignant peripheral nerve sheath tumor (MPNST) [6]
Can involve spinal nerves, causing neurological symptoms
Dermatofibroma vs Neurofibroma: Key Differences
Understanding the distinctions between these two conditions is essential for proper diagnosis and management. Here's a comprehensive comparison:
Origin and Cellular Composition
Dermatofibroma:
Originates from fibroblasts and fibrous tissue cells in the dermis
Composed primarily of spindle-shaped fibroblasts and histiocytes
Represents a proliferation of dermal connective tissue
Neurofibroma:
Arises from peripheral nerve sheaths and endoneurium
Contains Schwann cells, fibroblasts, perineural cells, and mast cells
Represents a true nerve sheath tumor
Etiology and Causes
Dermatofibroma:
Unclear etiology with multiple proposed mechanisms
Possibly reactive to trauma, insect bites, or inflammation
May have heterogeneous origins
No genetic syndrome association in most cases
Neurofibroma:
Caused by NF1 gene mutations on chromosome 17
Can be sporadic (isolated) or syndromic (part of NF1)
Clear genetic basis for development
Autosomal dominant inheritance pattern in NF1
Physical Examination Findings
The palpation characteristics provide crucial diagnostic clues when comparing dermatofibroma vs neurofibroma:
Dermatofibroma:
Firm and fixed consistency
Dimple sign positive – center dimples when squeezed from sides
Non-compressible
Usually solitary
Adherent to overlying skin
Neurofibroma:
Soft and compressible texture
Buttonhole sign positive – invaginates into underlying tissue when pressed
Plexiform type has "bag of worms" feel
Often multiple (especially in NF1)
Mobile under the skin
Location and Distribution Patterns
Dermatofibroma:
Lower legs most common (60-70% of cases)
Arms and trunk less frequently
Usually solitary lesions
Random distribution pattern
Neurofibroma:
Trunk, head/neck, and extremities equally affected
Diffuse type prefers head and neck
Plexiform type often on trunk
Multiple lesions common in NF1 patients
Appearance and Color
Dermatofibroma:
Brown to skin-colored most common
Can be pink, red, or black
Well-defined but slightly irregular borders
Surface usually smooth or slightly scaly
May have central clearing in older lesions
Neurofibroma:
Skin-colored to violaceous (purplish)
Plexiform types may have overlying hyperpigmentation
Borders often less defined
Surface typically smooth
May have associated café-au-lait spots (in NF1)
Diagnosis: How Doctors Differentiate Between These Conditions
Clinical Examination
The initial evaluation when comparing dermatofibroma vs neurofibroma involves:
Visual Inspection
Assessing color, size, and border characteristics
Looking for associated features (café-au-lait spots, freckling)
Noting distribution pattern (solitary vs. multiple)
Palpation Tests
Dimple/pinch sign for dermatofibroma
Buttonhole sign for neurofibroma
Assessing consistency (firm vs. soft)
Evaluating mobility and depth
Patient History
Duration of lesion presence
Growth pattern and changes
Associated symptoms (pain, itching, numbness)
Family history of neurofibromatosis
History of trauma or insect bites
Dermoscopy
Dermoscopy (examination with a specialized magnifying device) reveals distinct patterns:
Dermatofibroma Dermoscopic Features:
Central white scar-like area
Peripheral delicate pigment network
Vascular pattern with fine vessels
Sometimes crystalline structures
Neurofibroma Dermoscopic Features:
Homogeneous pattern
Fine telangiectasias
Skin-colored to pink background
Less distinctive features than dermatofibroma
Histopathological Examination
When clinical diagnosis is uncertain, biopsy with microscopic examination provides definitive diagnosis:
Dermatofibroma Microscopy:
Spindle-shaped fibroblasts in storiform (pinwheel) pattern
Collagen trapping at periphery
Variable cellularity
May contain hemosiderin, foam cells, or giant cells
Well-circumscribed but not encapsulated
Neurofibroma Microscopy:
Loose, haphazard arrangement of spindle cells
"Shredded carrot" appearance of collagen bundles [7]
Plexiform neurofibromas difficult to excise completely
Higher recurrence rates than dermatofibromas
May require nerve grafting for large lesions
Medical Therapy:
Selumetinib: FDA-approved MEK inhibitor for symptomatic, inoperable plexiform neurofibromas in NF1 patients [10]
Shows tumor shrinkage in 70% of patients
Oral medication with manageable side effects
Represents major advancement in NF1 treatment
Emerging Therapies:
Other MEK inhibitors under investigation
mTOR inhibitors showing promise
Gene therapy research ongoing
Clinical trials available for eligible patients
Living with These Conditions: Practical Considerations
Quality of Life Factors
For Dermatofibroma Patients:
Minimal impact on daily life
Cosmetic concerns may affect self-esteem
Occasional irritation from clothing or shaving
Generally no functional impairment
Excellent long-term prognosis
For Neurofibroma Patients:
Isolated Neurofibromas:
Similar minimal impact as dermatofibromas
Cosmetic concerns if multiple or large
Generally good quality of life
NF1 Patients with Multiple Neurofibromas:
Significant cosmetic impact possible
Potential functional impairment
Psychological effects of visible tumors
Need for ongoing medical surveillance
Risk of complications (vision problems, skeletal abnormalities, learning disabilities)
When to Seek Medical Attention
Consult a healthcare provider if you notice:
✅ New skin growths that are growing or changing ✅ Rapid increase in size of existing lesions ✅ Pain, tenderness, or neurological symptoms (numbness, tingling) ✅ Bleeding, ulceration, or discharge from lesions ✅ Multiple skin-colored nodules, especially with café-au-lait spots ✅ Family history of neurofibromatosis ✅ Cosmetic concerns affecting quality of life ✅ Functional impairment from lesion location
Genetic Counseling for Neurofibroma Patients
Individuals with multiple neurofibromas or diagnosed NF1 should consider:
Genetic Testing:
Confirms NF1 diagnosis
Identifies specific mutation
Helps predict disease course
Informs family planning decisions
Family Screening:
50% chance of passing NF1 to children
Early diagnosis enables better management
Screening for complications (optic gliomas, bone abnormalities)
Reproductive Options:
Preimplantation genetic diagnosis
Prenatal testing available
Informed decision-making support
Prevention and Risk Reduction
Can These Conditions Be Prevented?
Dermatofibroma:
No proven prevention strategies
Possible association with trauma suggests:
Protecting skin from injuries
Proper wound care after cuts or bites
Using insect repellent
However, many develop without identifiable trigger
Neurofibroma:
Cannot be prevented when genetic
Sporadic cases unpredictable
For NF1 families:
Genetic counseling before conception
Prenatal diagnosis options
Early detection enables better outcomes
Risk Factor Modification
While you cannot prevent these conditions entirely, you can:
Reduce Complications:
Protect lesions from trauma
Avoid excessive sun exposure (may darken dermatofibromas)
Maintain good skin hygiene
Monitor for changes systematically
Optimize Overall Health:
Regular dermatology check-ups
Maintain healthy lifestyle
Manage stress (may affect NF1 symptoms)
Stay informed about treatment advances
The Role of Healthcare Professionals
When Comparing Dermatofibroma vs Neurofibroma: Who to See
Primary Care Physician:
Initial evaluation of skin lesions
Basic differentiation and reassurance
Referral to specialists when needed
Coordination of care for NF1 patients
Dermatologist:
Expert clinical diagnosis
Dermoscopy examination
Skin biopsy when indicated
Treatment of dermatofibromas
Management of cutaneous neurofibromas
Neurologist:
Evaluation of neurological symptoms
Management of NF1 complications
Coordination with other specialists
Genetic Counselor:
Family history assessment
Genetic testing coordination
Risk counseling
Family planning guidance
Oncologist:
Management if malignant transformation occurs
Chemotherapy for MPNST
Clinical trial enrollment
Plastic/Reconstructive Surgeon:
Removal of large or complex lesions
Cosmetic reconstruction
Functional restoration
Latest Research and Future Directions
Advances in Understanding
Recent research has expanded our knowledge of dermatofibroma vs neurofibroma:
Dermatofibroma Research:
Molecular studies identifying driver mutations
Better understanding of cellular origins
Investigation of non-surgical treatment options
Improved diagnostic markers
Neurofibroma Research:
Detailed mapping of NF1 gene mutations
Understanding tumor microenvironment
Identification of therapeutic targets
Development of targeted medications
Promising Treatments on the Horizon
For Neurofibromas:
Additional MEK inhibitors showing efficacy
Combination therapies targeting multiple pathways
Immunotherapy approaches being explored
Gene editing technologies in preclinical studies
Topical treatments for cutaneous neurofibromas
For Dermatofibromas:
Improved laser technologies for less invasive treatment
Injectable treatments to dissolve lesions
Better understanding of when treatment is truly necessary
Clinical Trials and Participation
Patients with neurofibromas, especially those with NF1, may benefit from:
Finding Clinical Trials:
ClinicalTrials.gov database
NF patient advocacy organizations
Academic medical centers
Specialized NF clinics
Benefits of Participation:
Access to cutting-edge treatments
Close medical monitoring
Contributing to scientific knowledge
Potential for better outcomes
Common Myths and Misconceptions
Debunking False Information
Myth 1: "All skin bumps are cancerous"
❌ False: Both dermatofibromas and localized neurofibromas are benign
✅ Truth: While monitoring is important, most skin nodules are harmless
Myth 2: "Dermatofibromas will spread throughout the body"
❌ False: Dermatofibromas don't spread or metastasize
✅ Truth: They remain localized and stable
Myth 3: "Neurofibromas always mean you have NF1"
❌ False: Isolated neurofibromas occur without NF1
✅ Truth: Multiple neurofibromas plus other features suggest NF1
Myth 4: "You can prevent these growths with diet or supplements"
❌ False: No evidence supports dietary prevention
✅ Truth: These are genetic or reactive conditions not influenced by nutrition
Myth 5: "Removing one neurofibroma will cause more to grow"
❌ False: Surgical removal doesn't trigger new tumor growth
✅ Truth: New tumors in NF1 develop due to underlying genetic condition, not surgery
Cost Considerations and Insurance Coverage
Financial Aspects of Diagnosis and Treatment
Diagnostic Costs:
Clinical examination: Usually covered by insurance
Dermoscopy: Typically included in dermatology visit
Biopsy: Generally covered when medically indicated
Advanced imaging: Covered for neurofibromas with symptoms or NF1
Treatment Costs:
Dermatofibroma:
Observation: No cost
Surgical excision: $200-$800 (usually covered if symptomatic)
Cosmetic removal: May not be covered by insurance
Alternative treatments: Variable coverage
Neurofibroma:
Surgical excision: $500-$5,000+ depending on complexity
Selumetinib therapy: $10,000+ monthly (often covered for approved indications)
Ongoing surveillance: Covered for NF1 patients
Genetic testing: Increasingly covered by insurance
Obtain prior authorization for expensive treatments
Appeal denials with physician support
Explore patient assistance programs for medications
Consider flexible spending accounts for out-of-pocket costs
Pediatric Considerations
Dermatofibroma vs Neurofibroma in Children
Dermatofibromas in Children:
Less common than in adults
Same clinical features when present
Often discovered incidentally
Treatment approach similar to adults
Excellent prognosis
Neurofibromas in Children:
More common, especially with NF1
Plexiform type often present at birth
Requires different management approach:
Regular monitoring for complications
Developmental assessments
Educational support if needed
Family counseling and support
Special Pediatric Concerns:
Psychological impact of visible lesions
Bullying and social challenges
Growth-related changes in tumor size
Transition to adult care planning
Supporting Children with These Conditions
For Parents:
Educate child age-appropriately about condition
Connect with support groups and other families
Advocate for school accommodations if needed
Maintain regular medical follow-up
Address psychological and social needs
Celebrate child's strengths and abilities
For Healthcare Providers:
Use child-friendly language
Involve child in decision-making when appropriate
Coordinate multidisciplinary care
Provide resources for families
Screen for learning disabilities (NF1)
Monitor for complications
Dermatofibroma vs Neurofibroma: Making Informed Decisions
Questions to Ask Your Healthcare Provider
When diagnosed with either condition, consider asking:
About Diagnosis:
"Are you certain this is a dermatofibroma/neurofibroma?"
"Do I need a biopsy to confirm?"
"Should I have genetic testing for NF1?"
"What features make you confident in this diagnosis?"
About Treatment:
"Do I need treatment, or can I safely observe?"
"What are my treatment options and their pros/cons?"
"What are the risks of leaving this untreated?"
"How likely is recurrence after removal?"
"Are there non-surgical alternatives?"
About Follow-up:
"How often should I be monitored?"
"What changes should prompt me to return sooner?"
"Do I need imaging studies?"
"Should my family members be screened?"
About Prognosis:
"What is my long-term outlook?"
"What is the risk of malignant transformation?"
"Will this affect my quality of life?"
"Are there any restrictions on my activities?"
Building Your Healthcare Team
Optimal management of dermatofibroma vs neurofibroma may require:
Core Team Members:
Primary care physician for coordination
Dermatologist for skin evaluation and treatment
Pathologist for tissue diagnosis
Additional Specialists (for Neurofibromas/NF1):
Neurologist for neurological complications
Genetic counselor for family planning
Ophthalmologist for vision screening
Orthopedic surgeon for bone complications
Oncologist if malignancy develops
Mental health professional for psychological support
Support Resources:
Patient advocacy organizations
Support groups (in-person and online)
Educational materials and websites
Clinical trial coordinators
Patient Stories and Perspectives
Living with Dermatofibromas
Many patients with dermatofibromas report:
Common Experiences:
Initial concern about "mysterious bumps"
Relief upon learning they're benign
Minimal impact on daily activities
Occasional cosmetic concerns
Successful outcomes with removal when desired
Patient Advice:
"Don't panic when you find a dermatofibroma. Get it checked by a dermatologist, but know that these are usually harmless. I had mine for years before deciding to have it removed for cosmetic reasons, and the procedure was quick and easy."
Living with Neurofibromas
Patients with neurofibromas, especially those with NF1, share different experiences:
For Isolated Neurofibromas:
Similar to dermatofibroma experiences
Generally minimal life impact
Successful management with observation or removal
For NF1 Patients:
Journey of diagnosis and acceptance
Importance of comprehensive medical care
Value of support networks
Hope from new treatments like selumetinib
Advocacy for awareness and research
Patient Perspective:
"Being diagnosed with NF1 was overwhelming at first, but connecting with other families and staying informed about new treatments has made a huge difference. Regular monitoring gives me peace of mind, and knowing that treatments like selumetinib exist provides hope for the future."
The Importance of Awareness and Education
Why Understanding Dermatofibroma vs Neurofibroma Matters
For Patients:
Reduces anxiety about benign skin growths
Enables informed decision-making about treatment
Helps recognize when medical attention is needed
Facilitates productive conversations with healthcare providers
Empowers participation in care decisions
For Healthcare Providers:
Improves diagnostic accuracy
Guides appropriate treatment recommendations
Identifies patients needing genetic evaluation
Enables early detection of complications
Optimizes resource utilization
For Society:
Reduces unnecessary medical procedures
Advances research through awareness
Supports patients with NF1 and their families
Promotes genetic counseling when appropriate
Encourages funding for treatment development
Advocacy and Support Organizations
Several organizations provide resources and support:
For Neurofibromatosis:
Children's Tumor Foundation
Neurofibromatosis Network
NF Northeast
Regional NF support groups
International NF organizations
For General Dermatology:
American Academy of Dermatology
Dermatology Foundation
Patient advocacy groups for skin conditions
Resources Offered:
Educational materials and webinars
Patient conferences and events
Research updates and clinical trial information
Connection to specialized medical centers
Peer support and mentorship programs
Financial assistance information
Conclusion: Empowering Yourself with Knowledge
Understanding the differences between dermatofibroma vs neurofibroma is essential for anyone who has discovered a skin growth or been diagnosed with either condition. While both are generally benign, they differ significantly in their origin, characteristics, and management approaches.
Key Points to Remember
Dermatofibromas are firm, brown nodules arising from dermal fibroblasts, most commonly found on the lower legs. They exhibit a characteristic dimple sign and rarely require treatment beyond reassurance. The risk of malignant transformation is extremely low, making observation a safe and appropriate approach for most patients.
Neurofibromas are soft, compressible tumors originating from peripheral nerve sheaths, caused by NF1 gene mutations. They demonstrate a buttonhole sign on examination and may occur as isolated lesions or as part of neurofibromatosis type 1. While localized neurofibromas have minimal malignancy risk, plexiform neurofibromas require careful monitoring due to their 8-13% transformation risk.
Taking Action: Your Next Steps
If you have a skin growth and are uncertain whether it's a dermatofibroma, neurofibroma, or something else:
Schedule an evaluation with a dermatologist or primary care physician
Document changes with photographs and notes about size, color, or symptoms
Prepare questions for your healthcare provider using the guide in this article
Don't panic – remember that both conditions are typically benign
Follow through with recommended monitoring or treatment plans
If you've been diagnosed with either condition:
Understand your diagnosis by asking questions and reviewing reliable resources
Consider your options for observation versus treatment
Attend follow-up appointments as recommended
Monitor for changes that might indicate need for intervention
Connect with support if you have NF1 or multiple neurofibromas
Stay informed about new research and treatment advances
The Future Is Promising
Medical research continues to advance our understanding of both dermatofibroma and neurofibroma. New treatments, particularly for neurofibromas associated with NF1, offer hope for improved outcomes. The approval of selumetinib for plexiform neurofibromas represents a major breakthrough, and additional targeted therapies are in development.
Final Thoughts
Whether you're dealing with a dermatofibroma, neurofibroma, or simply seeking information, remember that knowledge is power. Understanding these conditions enables you to make informed decisions, communicate effectively with healthcare providers, and approach your situation with confidence rather than fear.
Both dermatofibromas and neurofibromas are manageable conditions with generally excellent prognoses. With proper diagnosis, appropriate monitoring, and timely intervention when needed, patients with either condition can maintain excellent quality of life.
Stay informed, stay proactive, and don't hesitate to seek expert medical advice when you have concerns about any skin growth. Your health and peace of mind are worth the investment in proper evaluation and care.
References
[1] Calonje, E., Brenn, T., Lazar, A., & McKee, P. H. (2020). McKee's Pathology of the Skin (5th ed.). Elsevier.
[2] Zelger, B. G., Steiner, H., Kutzner, H., & Maier, H. (2000). Cellular "fibrous histiocytoma" of the skin: Histological and immunohistochemical analysis. American Journal of Dermatopathology, 22(5), 413-422.
[3] Gleason, B. C., & Fletcher, C. D. (2008). Deep "benign" fibrous histiocytoma: Clinicopathologic analysis of 69 cases of a rare tumor indicating occasional metastatic potential. American Journal of Surgical Pathology, 32(3), 354-362.
[4] Ferner, R. E., & Gutmann, D. H. (2013). Neurofibromatosis type 1 (NF1): Diagnosis and management. Handbook of Clinical Neurology, 115, 939-955.
[5] Rodriguez, F. J., Folpe, A. L., Giannini, C., & Perry, A. (2012). Pathology of peripheral nerve sheath tumors: Diagnostic overview and update on selected diagnostic problems. Acta Neuropathologica, 123(3), 295-319.
[6] Miettinen, M. M., Antonescu, C. R., Fletcher, C. D., et al. (2017). Histopathologic evaluation of atypical neurofibromatous tumors and their transformation into malignant peripheral nerve sheath tumor in patients with neurofibromatosis 1. Human Pathology, 67, 1-10.
[7] Woodruff, J. M., Godwin, T. A., Erlandson, R. A., Susin, M., & Martini, N. (1981). Cellular schwannoma: A variety of schwannoma sometimes mistaken for a malignant tumor. American Journal of Surgical Pathology, 5(8), 733-744.
[8] Alves, J. V., Matos, D. M., & Barreiros, H. F. (2014). Dermatofibroma: A comprehensive review. Anais Brasileiros de Dermatologia, 89(3), 433-438.
[9] Tucker, T., Wolkenstein, P., Revuz, J., Zeller, J., & Friedman, J. M. (2005). Association between benign and malignant peripheral nerve sheath tumors in NF1. Neurology, 65(2), 205-211.
[10] Gross, A. M., Wolters, P. L., Dombi, E., et al. (2020). Selumetinib in children with inoperable plexiform neurofibromas. New England Journal of Medicine, 382(15), 1430-1442.