When your hand goes numb at night, the automatic assumption is often carpal tunnel syndrome. But what if the tingling affects your pinky and ring finger instead of your thumb? This scenario reveals a crucial diagnostic distinction that many people—and even some healthcare providers—overlook. Carpal Tunnel and the Ulnar Nerve: When Numbness Is Not Just in the Thumb and Index Finger represents a complex diagnostic challenge that requires understanding the distinct patterns of nerve compression affecting the hand and wrist.
The location of numbness and tingling in your fingers serves as a roadmap to identifying which nerve is compressed. While carpal tunnel syndrome affects the median nerve and causes symptoms in the thumb, index, and middle fingers, ulnar nerve entrapment creates an entirely different symptom pattern. This distinction is not merely academic—it directly impacts treatment decisions, recovery timelines, and long-term outcomes.
• Finger location matters: Carpal tunnel affects thumb and index finger, while ulnar nerve problems cause numbness in pinky and ring finger
• Two main ulnar nerve compression sites: Cubital tunnel at the elbow (most common) and Guyon's canal at the wrist (rare)
• Both conditions cause nighttime symptoms: Hands "falling asleep" during sleep is common to both median and ulnar nerve compression
• Treatment success varies: About 50% of ulnar nerve cases improve with conservative treatment, while surgical intervention may be necessary for severe cases
• Early diagnosis prevents complications: Delayed treatment can lead to permanent weakness and muscle atrophy in both conditions
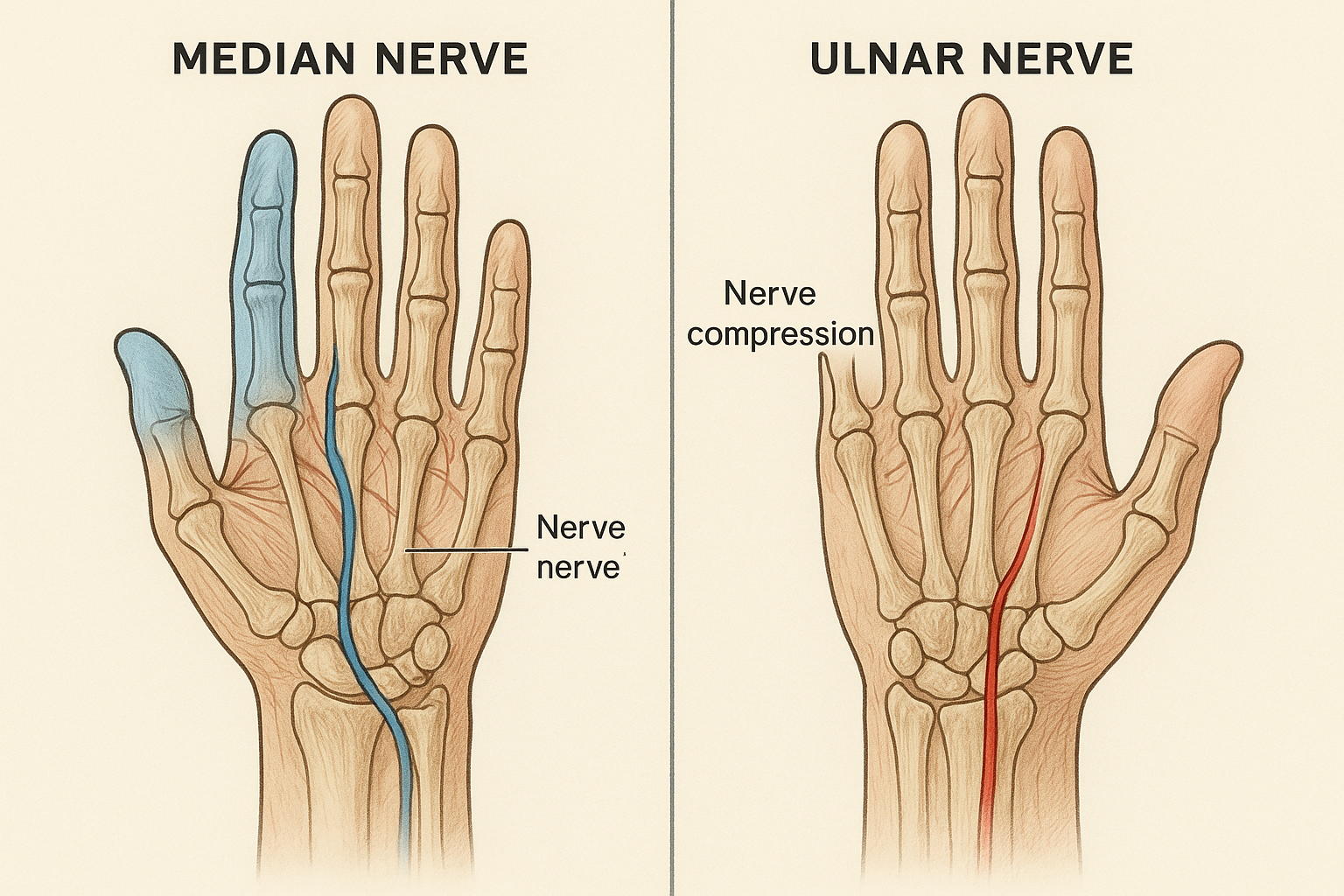
The human hand receives sensation and motor control from three primary nerves: the median, ulnar, and radial nerves. Each nerve has a specific territory it controls, creating distinct symptom patterns when compressed or damaged.
The median nerve travels through the carpal tunnel at the wrist, a narrow passageway formed by bones and ligaments. This nerve provides sensation to:
When the median nerve becomes compressed in the carpal tunnel, it creates the classic carpal tunnel syndrome pattern of numbness and tingling in these specific fingers.
The ulnar nerve takes a different route, traveling along the pinky side of the arm and hand. It can become compressed at two main locations:
The ulnar nerve provides sensation to:
Understanding these anatomical territories helps explain why carpal tunnel and ulnar nerve conditions create such different symptom patterns.
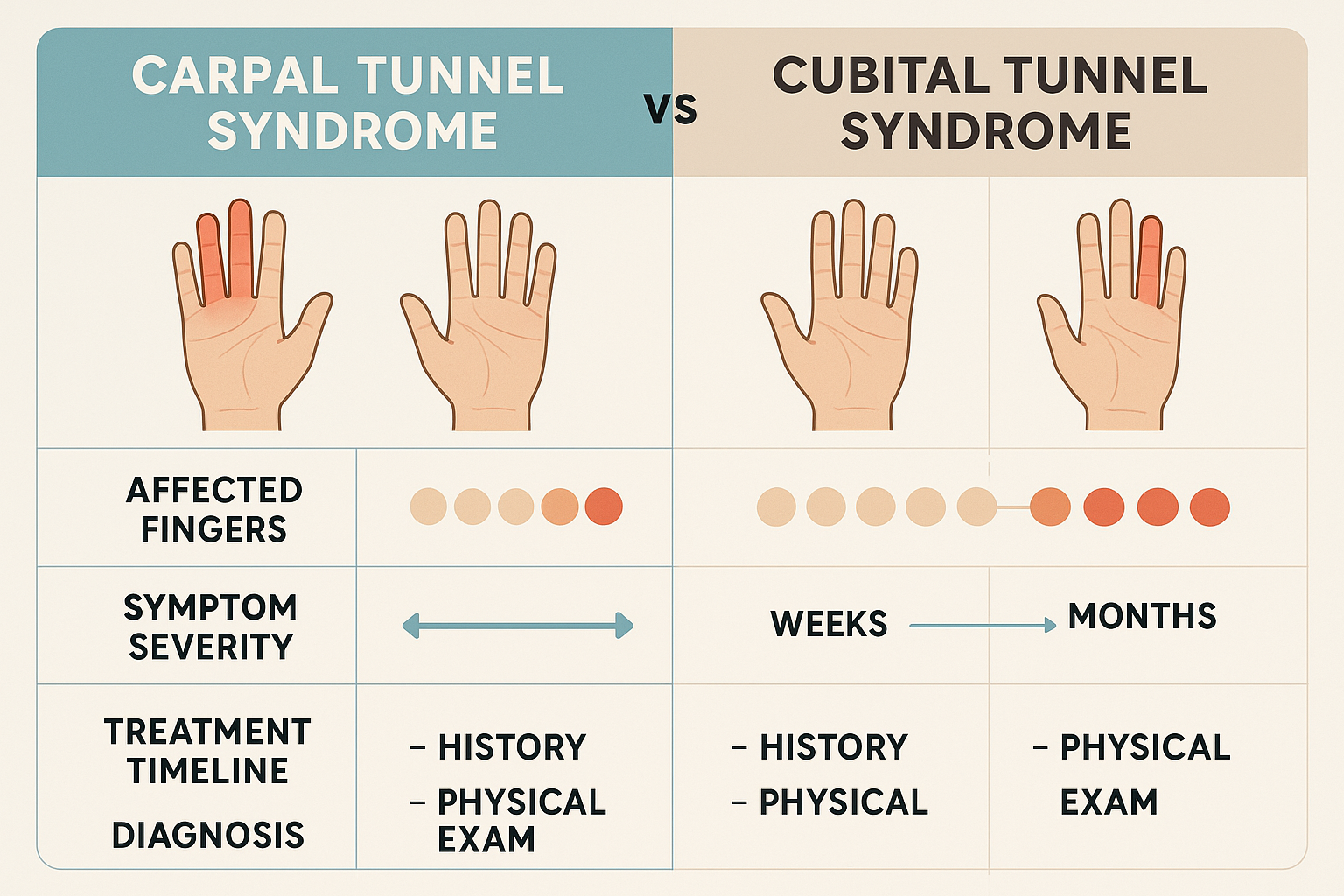
FeatureCarpal Tunnel SyndromeUlnar Nerve EntrapmentAffected FingersThumb, index, middlePinky, ringCommon LocationWrist (carpal tunnel)Elbow (cubital tunnel) or wrist (Guyon's canal)Weakness PatternThumb weaknessPinky weaknessNight SymptomsVery commonCommonMuscle AtrophyThumb musclesSpace between thumb and index finger
Both conditions share some common characteristics that can make initial diagnosis challenging:
Nighttime Symptoms 🌙
Activity-Related Triggers
Cubital tunnel syndrome represents the second most common peripheral neuropathy affecting the upper extremities, following carpal tunnel syndrome. This condition occurs when the ulnar nerve becomes compressed as it passes through the cubital tunnel at the elbow.
Repetitive Elbow Flexion
Direct Pressure
Anatomical Factors
Cubital tunnel syndrome typically develops gradually, with symptoms progressing through distinct stages:
Early Stage
Moderate Stage
Advanced Stage
Understanding these progression patterns helps patients recognize when to seek professional evaluation and treatment.
While cubital tunnel syndrome affects the ulnar nerve at the elbow, Guyon's canal syndrome involves compression of the same nerve as it passes through a small tunnel at the wrist. This condition is significantly less common than its elbow counterpart.
Location Specificity
Common Causes
Guyon's canal syndrome can be particularly challenging to diagnose because:
The key diagnostic differentiator remains the finger distribution—numbness in the pinky and ring finger points to ulnar nerve involvement, regardless of whether the compression occurs at the elbow or wrist.
In some cases, patients may experience symptoms suggesting both carpal tunnel and ulnar nerve problems. This scenario requires careful evaluation to determine whether:
Cervical Radiculopathy Mimics Nerve compression in the neck can create symptoms that mimic both carpal tunnel and ulnar nerve entrapment. Key differences include:
Thoracic Outlet Syndrome This condition involves compression of nerves and blood vessels between the collarbone and first rib, potentially affecting:
Double Crush Syndrome Some patients experience nerve compression at multiple sites along the same nerve pathway, requiring comprehensive evaluation and potentially multiple treatment approaches.
For complex cases involving multiple symptoms or unclear diagnoses, consulting with specialists experienced in comprehensive nerve evaluation becomes essential.
Accurate diagnosis of nerve compression conditions requires a systematic approach combining clinical evaluation with appropriate testing.
History Taking
Physical Examination
Nerve Conduction Studies
Electromyography (EMG)
Ultrasound
MRI
Treatment approaches for both carpal tunnel and ulnar nerve entrapment follow similar principles, progressing from conservative measures to surgical intervention based on severity and response.
Activity Modification
Splinting and Bracing
Physical Therapy Comprehensive programs addressing:
Patients interested in specific exercise programs can explore carpal tunnel exercises and stretches for detailed guidance.
Anti-inflammatory Treatments
Research indicates that approximately 50% of patients with ulnar nerve entrapment achieve significant symptom relief through conservative treatment alone. Success factors include:
When conservative treatment fails or symptoms are severe, surgical options become necessary:
Carpal Tunnel Release
Cubital Tunnel Surgery
Guyon's Canal Release
For patients considering surgical options, understanding carpal tunnel surgery recovery expectations provides valuable preparation guidance.
Preventing nerve compression conditions requires understanding risk factors and implementing protective strategies in daily activities.
Computer Workstation Setup
Ergonomic Tools and Equipment Modern technology offers numerous solutions for reducing nerve compression risk:
Exploring ergonomic gadgets for preventing carpal tunnel can provide specific product recommendations and usage guidelines.
Preventing Nighttime Compression
Understanding carpal tunnel and sleeping positions offers detailed strategies for improving nighttime comfort.
Exercise and Recreation
Daily Life Activities
The long-term outlook for patients with carpal tunnel and ulnar nerve conditions depends on several factors:
Timing of Treatment
Severity at Diagnosis
Patient Compliance
Untreated Progression Without appropriate treatment, both conditions can lead to:
Post-Surgical Considerations While surgery often provides excellent results, potential complications include:
Pregnancy can significantly impact both carpal tunnel and ulnar nerve symptoms due to:
Detailed information about carpal tunnel during pregnancy helps expectant mothers understand their options.
Younger Patients
Older Adults
Several medical conditions can increase the risk of nerve compression:
Recognizing when symptoms require professional evaluation is crucial for optimal outcomes:
Immediate Evaluation Needed
Progressive Symptoms Requiring Attention
Primary Care Evaluation
Specialist Consultation
For patients seeking specialized care, finding the right treatment center with experience in nerve compression conditions is essential.
Carpal Tunnel and the Ulnar Nerve: When Numbness Is Not Just in the Thumb and Index Finger represents a critical diagnostic distinction that directly impacts treatment success and long-term outcomes. Understanding that finger location serves as a roadmap to nerve involvement—with carpal tunnel affecting the thumb and index finger versus ulnar nerve problems causing pinky and ring finger symptoms—empowers patients to seek appropriate care and communicate effectively with healthcare providers.
The key to successful management lies in early recognition, accurate diagnosis, and appropriate treatment selection. While approximately 50% of ulnar nerve cases respond well to conservative treatment, the remaining cases may require surgical intervention to prevent permanent complications. Similarly, carpal tunnel syndrome benefits from early intervention, whether through ergonomic modifications, splinting, or surgical release when conservative measures prove insufficient.
Remember that nerve compression conditions are highly treatable when addressed promptly and appropriately. By understanding the distinct patterns of carpal tunnel and ulnar nerve problems, patients can become active participants in their diagnosis and treatment, leading to better outcomes and improved quality of life.
SEO Meta Information:
Meta Title: Carpal Tunnel vs Ulnar Nerve: Finger Numbness Guide 2025
Meta Description: Learn the key differences between carpal tunnel and ulnar nerve problems. Discover which fingers are affected, treatment options, and when to seek help for hand numbness.



