Imagine recovering from wrist surgery in just three to six days instead of waiting four to six weeks. That scenario is no longer a distant hope — it is happening right now. The advancements in carpal tunnel syndrome 2026 are transforming the way doctors diagnose, treat, and help patients recover from one of the most common nerve conditions in the world. From ultrasound-guided releases that require only a tiny incision to artificial-intelligence-powered diagnostics that catch the problem earlier than ever, 2026 marks a turning point for the estimated 3–6% of adults who develop carpal tunnel syndrome (CTS) during their lifetime. Whether someone works at a desk, operates heavy machinery, or is pregnant and dealing with sudden wrist pain, the options available today are more precise, less invasive, and faster-healing than anything seen before.
This article explores every major development — surgical innovations, diagnostic breakthroughs, non-surgical alternatives, and emerging technologies — so readers can make informed decisions about their wrist health in 2026 and beyond.
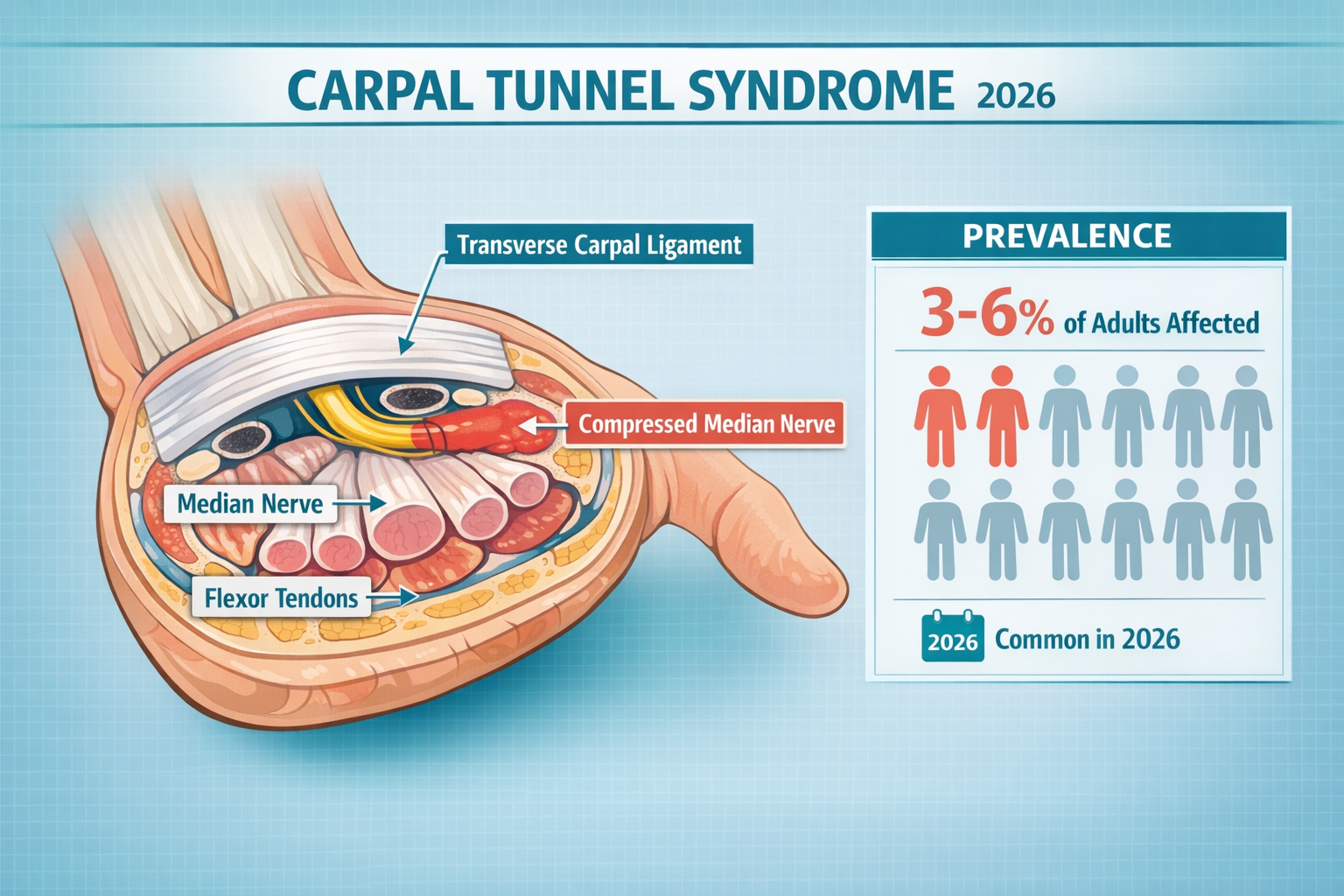
Before diving into the latest breakthroughs, it helps to understand the condition itself. Carpal tunnel syndrome occurs when the median nerve — which runs from the forearm through a narrow passageway (the carpal tunnel) in the wrist — becomes compressed. This compression causes numbness, tingling, weakness, and pain in the hand and fingers.
Risk FactorDetailsRepetitive hand motionsTyping, assembly-line work, vibrating toolsPregnancy & hormonal changesFluid retention swells the carpal tunnelChronic conditionsDiabetes, rheumatoid arthritis, thyroid disordersWrist anatomyNaturally smaller carpal tunnels increase riskAgeMost common between ages 40–60
CTS affects people across every profession and age group. It can even appear in children and teens, though this is less common. For a deeper look at the condition's causes and symptoms, visit this comprehensive carpal tunnel syndrome overview.
Several forces have converged to make 2026 a landmark year for CTS care:
One of the most significant advancements in carpal tunnel syndrome 2026 diagnostics is the widespread adoption of high-resolution ultrasound (HRUS). A narrative review published in NeuroSci in January 2026 by Đula Đilvesi, Bojan Jelača, and colleagues outlined how HRUS is reshaping early detection.
Traditional diagnosis has long relied on:
While these methods remain valuable, HRUS adds a dynamic, real-time visual layer. Doctors can now:
"High-resolution ultrasound allows clinicians to see the median nerve in motion — something no electrical test can do. This dynamic assessment is changing the diagnostic landscape for carpal tunnel syndrome." — Adapted from Đilvesi et al., NeuroSci, January 2026
This matters because misdiagnosis of carpal tunnel syndrome remains a real challenge. Conditions like cervical radiculopathy, thoracic outlet syndrome, and pronator syndrome can produce similar symptoms. HRUS helps distinguish CTS from these look-alikes with greater confidence.
While still in its early stages, artificial intelligence is being integrated into ultrasound platforms to:
These tools reduce operator dependency and make high-quality diagnostics available in more settings — including primary care offices and minor surgery centers.
Surgery remains the most effective long-term treatment for moderate-to-severe CTS. The AAOS guidelines (incorporated into 2026 reviews) recommend surgical intervention for patients with progressive neurological deficits, and studies show that surgery achieves two-fold higher nerve normalization rates compared to conservative management alone.
What has changed dramatically is how the surgery is performed.
The traditional approach involves a 3–5 cm incision in the palm to directly visualize and cut the transverse carpal ligament, relieving pressure on the median nerve.
Pros:
Cons:
Open CTR remains a reliable option, especially in complex cases or revision surgeries. For patients considering this approach, understanding what to expect during carpal tunnel surgery recovery is essential.
Endoscopic release uses a small camera (endoscope) inserted through one or two tiny incisions (approximately 1 cm) to cut the ligament from the inside.
Key 2026 data points:
Pros:
Cons:
The growth of endoscopic techniques reflects a broader trend in the carpal tunnel release systems market, where innovation is being driven by patient demand for faster recovery.
Perhaps the most exciting of the advancements in carpal tunnel syndrome 2026 is the maturation of ultrasound-guided release.
On January 21, 2026, Sonex Health announced the publication of the largest multi-center study ever conducted comparing ultrasound-guided CTR to traditional open release. The findings were striking:
MetricUltrasound-Guided CTROpen CTRLong-term efficacyComparableComparableTypical recovery time3–6 days4–6 weeksIncision size~3–4 mm (needle-based)3–5 cmScarringMinimalModerateAnesthesiaLocal onlyLocal or regionalSettingOffice-basedOperating room or clinic
Pioneered at Mayo Clinic, Thread Carpal Tunnel Release is a variation of ultrasound-guided CTR. It uses a thin thread-like device to cut the ligament under ultrasound visualization. Early clinical experience shows:
One important counterpoint: ultrasound-guided techniques have a steeper learning curve than traditional open release. Surgeons need specific training in musculoskeletal ultrasound and procedural guidance. However, as training programs expand and more physicians gain experience, accessibility is improving rapidly.
For a broader look at how surgical and non-surgical options compare, explore this guide on advances in carpal tunnel syndrome management.
FeatureOpen CTREndoscopic CTRUltrasound-Guided CTRIncision size3–5 cm~1 cm~3–4 mmVisualizationDirectCamera (endoscope)UltrasoundAnesthesiaLocal/regionalLocal/regionalLocal onlyRecovery time4–6 weeks2–3 weeks3–6 daysGrip strength returnSlowerModerateFastestScar tendernessCommonLess commonRareLong-term efficacyExcellentExcellentExcellentLearning curveStandardModerateSteepSettingOR or clinicOR or clinicOffice-based
Not every case of carpal tunnel syndrome requires surgery. For mild-to-moderate CTS — or for patients who prefer to start with conservative care — several non-surgical options have shown meaningful results.
Wearing a neutral-position wrist splint, especially at night, remains a first-line treatment. Nighttime splinting prevents the wrist from flexing during sleep, which can worsen nerve compression. Choosing the right device matters — this guide to selecting the best carpal tunnel brace or splint can help.
A single corticosteroid injection into the carpal tunnel can provide significant short-term relief (weeks to months). However, the benefits tend to diminish over time, and repeated injections carry risks including tendon weakening.
Targeted exercises — nerve gliding, tendon gliding, and wrist stretches — can reduce symptoms and improve function. In 2026, therapy protocols are increasingly personalized based on ultrasound findings and patient-specific biomechanics. Learn more about effective carpal tunnel physical and occupational therapy techniques.
Home-based stretching kits, such as the Carpal Solution stretching system, have gained attention. Proponents report up to 97% success rates in achieving symptom remission over 6–10 weeks. While these claims should be evaluated critically, the principle of consistent, targeted stretching is well-supported by rehabilitation science.
Prevention and symptom management go hand-in-hand with workstation design. In 2026, ergonomic tools have become more sophisticated:
For product recommendations, check out this roundup of ergonomic gadgets for preventing carpal tunnel.
The AAOS guidelines integrated into 2026 practice recommend surgery when:
For a full exploration of alternatives, visit this resource on carpal tunnel surgery alternatives.
The advancements in carpal tunnel syndrome 2026 extend beyond what is already in clinical practice. Several emerging technologies are poised to reshape CTS care in the coming years.
Researchers highlighted by Đilvesi and colleagues in their January 2026 review emphasize the growing role of regenerative biologics in CTS management:
Robotic surgical platforms — already used in cardiac, urological, and ophthalmic surgery — are being adapted for hand and wrist procedures. The potential benefits include:
While robotic-assisted carpal tunnel release is not yet mainstream, pilot programs at academic medical centers are generating early data. The integration of robotics with real-time ultrasound guidance could eventually create a fully image-guided, robot-assisted procedure that combines the best of both technologies.
Smart wristbands and gloves equipped with pressure sensors and accelerometers are being developed to:
These devices bridge the gap between clinical visits, giving doctors continuous insight into a patient's daily wrist mechanics.
Research is underway on bioabsorbable spacers that can be placed in the carpal tunnel after ligament release. These implants:
One of the most common concerns for CTS patients is how quickly they can return to their jobs. The answer depends on both the surgical technique used and the nature of the work:
Work TypeOpen CTREndoscopic CTRUltrasound-Guided CTRDesk/office work2–3 weeks1–2 weeks3–7 daysLight manual labor4–6 weeks3–4 weeks1–2 weeksHeavy manual labor6–8 weeks4–6 weeks2–4 weeks
These timelines are general estimates. Individual recovery varies based on age, overall health, CTS severity, and adherence to post-operative therapy. For a detailed breakdown, see this guide on returning to work after carpal tunnel syndrome for desk jobs vs. manual labour.
Many CTS patients report that symptoms are worst at night. This happens because people tend to flex their wrists during sleep, increasing pressure on the median nerve. Strategies include:
Carpal tunnel syndrome during pregnancy is common due to fluid retention. In most cases, symptoms resolve after delivery. However, when they persist or are severe, treatment options — including splinting, therapy, and occasionally injection — should be discussed with a healthcare provider. Learn more about carpal tunnel syndrome and pregnancy.
Even after successful treatment, CTS symptoms can return. Prevention strategies include:
A central theme across the 2026 literature is the shift toward individualized, evidence-based treatment planning. Rather than applying a one-size-fits-all approach, leading researchers — including the Đilvesi team — advocate for integrating:
"The future of carpal tunnel syndrome management lies in combining ultrasound imaging, regenerative biologics, and precision surgical techniques into a personalized treatment pathway for each patient." — Adapted from Đilvesi, Jelača, et al., NeuroSci, January 2026
This approach ensures that a 28-year-old software developer with mild intermittent tingling receives a very different treatment plan than a 55-year-old carpenter with severe thenar atrophy — even though both carry the same diagnosis.
Empowered patients get better outcomes. Here are key questions to bring to a consultation:
The advancements in carpal tunnel syndrome 2026 represent a genuine leap forward. Patients now have access to diagnostic tools that catch the condition earlier, surgical techniques that heal faster, and non-surgical options that are more targeted than ever. The convergence of high-resolution ultrasound, ultrasound-guided release, endoscopic innovation, and emerging technologies like regenerative biologics and robotic-assisted surgery means that CTS treatment is no longer a choice between "live with it" and "major surgery."
The wrist is small, but its impact on daily life is enormous. In 2026, the tools to protect it have never been better. 💪



